
Abstract
Extraction of global structural regularities provides general ‘gist’ of our everyday visual environment as it does the gist of abnormality for medical experts reviewing medical images. We investigated whether naïve observers could learn this gist of medical abnormality. Fifteen participants completed nine adaptive training sessions viewing four categories of unilateral mammograms: normal, obvious-abnormal, subtle-abnormal, and global signals of abnormality (mammograms with no visible lesions but from breasts contralateral to or years prior to the development of cancer) and receiving only categorical feedback. Performance was tested pre-training, post-training, and after a week’s retention on 200 mammograms viewed for 500 ms without feedback. Performance measured as d’ was modulated by mammogram category, with the highest performance for mammograms with visible lesions. Post-training, twelve observed showed increased d’ for all mammogram categories but a subset of nine, labelled learners also showed a positive correlation of d’ across training. Critically, learners learned to detect abnormality in mammograms with only the global signals, but improvements were poorly retained. A state-of-the-art breast cancer classifier detected mammograms with lesions but struggled to detect cancer in mammograms with the global signal of abnormality. The gist of abnormality can be learned through perceptual/incidental learning in mammograms both with and without visible lesions, subject to individual differences. Poor retention suggests perceptual tuning to gist needs maintenance, converging with findings that radiologists’ gist performance correlates with the number of cases reviewed per year, not years of experience. The human visual system can tune itself to complex global signals not easily captured by current deep neural networks.
Similar content being viewed by others

Medical experts often report having a gut feeling about the state of a radiograph when briefly looking at certain medical imaging cases, where they get the impression that something might be wrong but are not able to pinpoint the exact image elements that made them feel that way. These anecdotes suggest medical experts might rapidly access first impressions of abnormality. However, there is more than just anecdotal evidence for this notion: it is also supported by human observer studies, which have shown that radiologists are able to discriminate between normal and abnormal medical images with above-chance accuracy within 200–500 ms for chest radiographs (Kundel & Nodine, 1975), pathology images, or mammograms (Evans et al., 2013a, 2013b), the latter of which will be the focus of the current study. Thus, medical experts indeed possess the perceptual ability to rapidly extract a signal that indicates abnormality from images in their field of expertise.
This shows an incredible perceptive power, which is furthered by research demonstrating that the ability does not rely on the presence of a localizable signal like a lesion. Indeed, radiologists can recognize this gist of abnormality in patches of the abnormal mammogram that do not contain a lesion, or even from the breast contralateral to the abnormality (Evans et al., 2016), both of which do not contain any localizable abnormalities. Even more striking, when normal mammograms from women who went on to develop cancer in the next two to three years were intermixed with normal and abnormal mammograms, they were rated as significantly more abnormal than the normal images (Brennan et al., 2018; Evans et al., 2019). Thus, the gist of abnormality signal can be detected without localizable abnormalities. For mammograms containing a single mass, it has been suggested that radiologists can sometimes access coarse location information (Carrigan et al., 2018), although this study did remove image artefacts and large calcifications from the breast tissue. Together, these findings point to a rapidly extracted global signal of image statistics that allows medical experts to detect whether the imaged tissue is normal or abnormal, which might provide access to coarse location information, but does not require local information to function. This description fits closely with the process of gist extraction that has been widely described in the scene processing literature.
Gist extraction is a perceptual process that allows observers to quickly retrieve the global meaning, or gist, of visual input. After as little as 20–30 ms, humans can accurately discriminate between man-made and natural environments, so-called superordinate categories (Joubert et al., 2009), recognize forests, fields, rivers, and other basic scene categories (Greene & Oliva, 2009), or determine the presence or absence of broad categories such as animals (Bacon-Macé et al., 2005) or vehicles (VanRullen & Thorpe, 2001). Indeed, there is a wide range of research showing that humans can extract surprisingly complex information from rapidly presented visual information, which fits closely with the observations in rapid medical image perception.
The key characteristics of gist extraction are that it occurs rapidly, globally (across the whole image) with a loss of specific local information and does not require focused attention. Instead, it occurs without prior location of items and in a non-selective manner. For example, gist can be extracted from scenes in the periphery in parallel with a demanding foveal letter discrimination task (Li et al., 2003) or from two, or even four scenes in parallel with minimal drops in performance (Rousselet et al., 2004) or scenes presented in medium-to-far periphery (Boucart et al., 2013; Larson & Loschky, 2009), clearly showcasing the global and non-selective nature of the process. In addition, gist extraction does not require prior configuration of the visual system: it occurs when monitoring for multiple cue categories simultaneously (Evans et al., 2011a, 2011b), or even when the target category is post-cued after a rapid serial visual presentation (Evans et al., 2011a, 2011b; Potter et al., 2014). However, it also means that information about the locations of specific elements that make up the scene is not consciously accessible (Evans & Treisman, 2005). Overall, scene gist extraction clearly occurs rapidly, globally, and without the need of focused attention or preselection, which fits closely with the observations of what we will refer to as the gist of (medical) abnormality.
But which signals are extracted by this global, rapid process to contribute to the formation of our gist understanding? As every image is built up from spatial frequencies at various orientations, shared categorical regularities between a gist category might be captured in similarities in spatial structural regularities, as described by Portilla and Simoncelli (2000)’s statistics. The statistic they define are extracted using spatial filters of specific sizes and orientations and are applied to noise to create an artificial ‘metamer’, that contains the same spatial structural regularities, but no recognizable objects. Such a metamer is indistinguishable from the original in two alternative forced choice tasks (2-AFC) at 200 ms viewing time (Freeman & Simoncelli, 2011), suggesting that spatial structural regularities capture essential aspects of scenes that are accessed during gist extraction. The idea of a statistical signature of an image fits with the Efficient Coding Hypothesis (Simoncelli, 2003), as reducing an image to its spatial structural regularities would allow efficient encoding of its essential information. Mammogram content is even more closely related to its spatial frequency content than scene images, due to most of the content being textural. For example, previous research has shown that low-pass filtering strongly reduced gist extraction, while high-pass filtered mammograms retained most gist information (Evans et al., 2016). Spatial structural regularities might be more similar between images from the same category and thus allow for flexible perceptual rules for gist categorization.
Oliva and Torralba (2001) further explained these spatial structural regularities with a focus on human perception through gist descriptors, which similarly captured spatial frequency patterns on a global spatial scale, the global spatial envelope. Gist descriptors can be represented as scores on scales such as expansiveness and openness. Patterns in these feature scores have been shown to be more similar within than between scene categories. Additionally, false alarms made by observers could often be predicted by similarities in gist predictors (Greene & Oliva, 2009). This supports the idea that shared patterns of frequencies and textures could play an important role in the flexible, yet reliable gist categorization of scenes, which could reasonably be extended to mammograms.
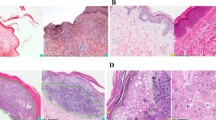
To allow for its non-selective and global nature, gist extraction must be highly flexible, especially as it must generalize across a wide range of exemplars that all fall under one gist category. For example, we can recognize the gist category of a scene environment in a variety of conditions, such as viewing angles, lighting, and specific objects (Fig. 1A, B), and the same applies to mammograms, as these can also vary widely in their appearance, size, shape, density, and texture (Fig. 1C, D). However, previous experience influences our ability to extract gist accurately, as human observers performed considerably worse on scene gist extraction for photographs from aerial compared to terrestrial viewpoints (Loschky et al., 2015). Thus, our brain might develop a set of general perceptual rules of expected spatial regularities for each gist category, based on previous experience, that are flexible enough to generalize across variations, but specific enough to allow it to distinguish a beach from a river, or a normal from an abnormal mammogram.

Scene exemplars for beaches (A) and playgrounds (B) that illustrate the variation in viewing angle, lightning, configuration, and specific objects. Mammogram exemplars containing subtle abnormalities (C) or no abnormalities (D) illustrating the variation in shape, size, and textural patterns
However, it is not yet known how people acquire these sets of expectations or sensitivity to emergent statistics needed to extract the gist of novel categories, whether that is a natural scene category, or a more abstract categorization of a medical image. Since the learning of natural scene categories happens during normal development, this learning must be able to occur under natural viewing conditions and should not rely on detailed feedback that explicitly explains which features make the scene a beach. Rather, the learning would be expected to reliably occur with broad feedback consisting of just categorical information (‘We are at a beach’). This learning would be in line with the principles of statistical learning, the process through which humans can extract naturally occurring statistical patterns in space and/or time (Turk-Browne et al., 2005).
Indeed, statistical learning leads observers to recognize temporal or spatial statistical regularities and patterns in auditory or visual stimuli after a multitude of exposures without explicit instructions on what to learn (Turk-Browne, 2012). For example, passively viewing a stream of symbols produced strong familiarity feeling for viewed patterns (Fiser & Aslin, 2002a). Interestingly, children as young as 9 months old pay more attention to arrays containing previously seen shape arrangements than new arrangements (Fiser & Aslin, 2002b), suggesting that statistical learning takes place from early on in our development. While the previous examples used simple shapes, statistical learning also extends to more complex stimuli, such as scene images. Observers report more familiarity with scene sequences, such as a kitchen followed by a forest, that were previously seen in a visual stream (300 ms each) without being instructed to pay attention to the order of scene categories (Brady & Oliva, 2007).
Statistical learning is often investigated in the context of temporally separated stimuli, but as previously stated, it also occurs over spatial regularities, which would form the basis for gist category learning. Indeed, observers become familiar with the configurations of complex objects in a grid through repeated exposure (Fiser & Aslin, 2001), and they can decrease their reaction time in a search task due to repeated configurations of distractor arrays without recognition of repeated arrays occurring (Chun & Jiang, 1998), as they implicitly learn to recognize the regularities in contextual cues, or in other words, invariant visual properties, allowing them to interact with the environment more efficiently (Chun, 2000). Similarly, someone might learn to recognize the invariant global properties of a forest, beach, or even an abnormal mammogram through statistical learning of spatial regularities. Statistical learning with global feedback allowed observers to recognize camouflaged objects by learning the general statistics of the background (Chen & Hegdé, 2012). Thus, in our definition of statistical, implicit learning, no assumptions are made about the unconscious nature of the learning or complete lack of awareness of learned patterns, but only that it consists of learning through repeated exposure without explicit instructions or feedback on which features or patterns to extract. We expect that statistical learning through repeated perceptual exposure to novel categories and their group labels would allow observers to acquire the gist of a new category.
To investigate the learning of gist signals, a category is needed in which observers can be trained to improve. Previous training research has shown that the speed of gist extraction from natural scenes is already optimized and at ceiling levels, as extensive training across 15 days did not significantly speed up the reaction time of a 2-AFC animal absent/present task (Fabre-Thorpe et al., 2001). While accuracy increased slightly and average reaction time decreased slightly for familiarized stimuli, this did not transfer to new stimuli and was mostly driven by an increase in speed/accuracy for the most difficult familiarized targets with RTs above 400 ms. Thus, the processes underlying gist extraction for scenes of categories are already highly efficient in adults and do not seem to be able to be further compressed or enhanced. Thus, scenes cannot be used to investigate the processes involved in the learning of a new category of gist. However, it does underline the fact that scene categories must be deeply familiar to the average human observer, which would only be possible if the global gist is learned through the rare instances of explicit feedback (‘these exact features make this a beach/forest/mountain’) or, as we hypothesize, is largely learned through the frequent global feedback moments we encounter in daily life (‘you are in a forest’). Interestingly, expertise within a specific object category, such as cars, will increase the ability to rapidly detect scenes containing that object category, but not others (e.g. humans), in a simultaneous presentation of two scenes (Reeder et al., 2016), adding support to the idea that expertise in a category might influence rapid detection of that category, similar to what is seen in medical experts.
For the gist of medical abnormality, previous research has repeatedly shown that, as expected, naïve observers are unable to extract this signal (Evans et al., 2013a, 2013b; Raat et al., 2021), showing that the general population is not familiar with this gist signal representing a medical abnormality. Interestingly, however, a recent study trained naïve observers to recognize obviously visibly abnormal mammograms (microcalcifications/breast mass) with above-chance accuracy after approximately 600 cases of training (Hegdé, 2020), showing that non-medically trained observers can develop the perceptual ability to recognize obvious abnormalities on free-viewing tasks. This indicates that naïve observers can, at the very least, learn to recognize perceptual characteristics of lesions in mammograms a localized signal, which suggests they might also be able to be trained to recognize the gist signals of abnormality in the overall tissue.
Thus, this study’s aims are twofold: to investigate whether/how people can learn the categorization of a new gist signal (medical abnormality) and to explore which perceptual features in mammograms might drive this gist signal. We will evaluate whether naïve observers can learn to rapidly recognize the gist of a new category after repeated perceptual exposure through training with global feedback, and if this learning is retained after the end of training. Global feedback is defined as the ground truth of the trial, without additional instructions on the location of abnormalities or potential features that might indicate the ground truth. In other words, the task and label are both made explicit, but since no further guidance on which content to use is provided, only implicit/statistical learning can be used. Since the gist of abnormality is a global signal, learning to recognize the gist of abnormality should improve performance on not only mammograms with visible abnormalities, but also on mammograms with only global signals of abnormality, such as contralateral mammograms or those taken prior to the development of localizable cancer, similar to the ability of trained medical experts (Brennan et al., 2018; Evans et al., 2016, 2019). Based on the framework of gist development, and the previous findings of Hegdé (2020), training is expected to induce learning of the gist of medical abnormality, and this is expected to improve performance for mammograms with and without local abnormalities.
As an extension to the training findings, we will also evaluate the performance of a state-of-the-art machine learning model on the same images and compare it to human perception. Human statistical, implicit learning shares key similarities with the concept of deep learning, a computational method where each decision is compared to the feedback of a simple label, inducing learning through backpropagation of the error between the decision and ground truth, which can lead to tuning towards statistical regularities in the input (Voulodimos et al., 2018). Both describe conceptually similar processes that could underlie learning without explicit rules or instructions. As one type of computational modelling, deep learning was developed based on observed brain architecture and processing (Voulodimos et al., 2018). Deep learning models can capture complex visual patterns, allowing for object (Ouyang et al., 2016; Simonyan & Zisserman, 2012; Palmeri et al., 2004; Xu et al., 2016).
Another interesting observation was the change in rating time, as participants became significantly faster after training. This increase in rating speed could potentially be a marker of the development of expertise. Decreases in reaction times have previously been described to occur in naïve learning to categorize aerial photographs (Lloyd et al., 2002) and training on face-like artificial object categorization (Wong et al., 2009). However, other studies reported no consistent changes in reaction time after training subordinate and superordinate level bird categorization (Devillez et al., 2019; Jones et al., 2020). Additionally, the interpretation of our findings is complicated by the fact that this study used a 0–100 rating scale, operated using a mouse. Thus, it is also possible that participants habituated to using the slider and became faster at reaching their desired rating score. Overall, this increase in rating speed is an interesting observation, but a different design is needed to be certain that this effect is caused by changes in decision-making time rather than adeptness at the rating task.
Deep neural network performance in detecting cancer
With the aim of further understanding how gist expertise develops we examined whether a DNN, analogous to human implicit learning, was able to capture the same image statistics that humans might be using when learning to detect the gist of the abnormal. We use a DNN specifically developed for malignancy detection, which was pre-trained on mammograms, to evaluate its performance on the mammograms we used for training and testing our human learners. This is assessed using the DNN’s calculated malignancy probability scores (Wu et al., 2019), the probability that that mammogram contained a malignant abnormality. Each unilateral mammogram in the training image set and test image set was scored by both the single breast classifier image-only (SBC) and SBC + heatmaps (SBC + HM) DNN. The DNN also provided benign probability scores, the probability that a mammogram contained a benign abnormality, which showed the same pattern of results as discussed below (see Appendix 6).
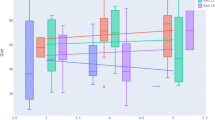
Histograms of DNN malignancy probability scores show more overlap between the normal and global cases than between the obvious/subtle and normal cases (Fig. 6), indicating that both the SBC and SBC + HM were less able to distinguish global and normal from each other. The finding illustrates an apparent difficulty for the SBC and SBC + HM to distinguish the global gist signal of cancer compared to the visible obvious and subtle cancers.

Distribution of single breast classifier (SBC) and SBC + Heatmap (SBC + HM) malignancy probability scores on the full image set of mammograms split into 25 bins for each of the image type categories, with a combined plot showing the overlap between normal (red), obvious (green), subtle (blue), and global (yellow) scores
Similarly, AUC calculations (Table 1) show that the SBC and SBC + HM both performed well in discriminating the obvious and subtle mammograms from the normal mammograms on malignancy probability, whereas AUC dropped considerably for the global mammograms, although it did remain above-chance levels for all except the malignancy-SBC on the global mammograms in the test set. The increase in AUC for SBC + HM shows that heatmaps improved the DNN’s ability to detect the probability of malignancy in mammograms, especially in more subtle cases. These results on our mammography image lend support to the reported increase in performance with the added heat map described in the original publication (Wu et al., 2019).
Most critically, the low or even at-chance performance (AUC: 0.505 SBC on the test set) on the globally abnormal mammograms shows that mammograms with the global signal of abnormality are especially obscure and difficult to detect. This adds to the significance of our finding that human observers were able to learn to detect abnormalities in these mammograms, performing above chance on the test set with which the SBC struggled severely. It also demonstrates that the chosen test set was representative of, or potentially even more difficult than, the overall mammography data set, and learning was not a result of coincidentally easier stimuli in the test set.
Next, a direct comparison of human and SBC scores was made to see if similar image statistics might be used by human observers and machine learning models. This was done by correlating the average rating from the ‘learner’ group of observers to the malignancy probability scores of the SBC and SBC + HM. Spearman’s rank correlations were performed between the DNN malignancy probabilities and the average of the human learner scores given pre- and post-perceptual training (Table 2). Before perceptual training, the correlation between SBC malignancy and human scores was non-significant (p = 0.137), while the correlation between SBC + HM and human scores was (p = 0.005). At the post-training test, the average human score across the 200 test mammograms correlated significantly with both the SBC and SBC + HM malignancy and benign scores (all p < 0.01, see Table 2). Comparing pre- and post-perceptual training correlations showed that the correlation coefficient increased after the human observers completed their perceptual training. After training, human scores more closely agreed with the classifier judgements—mammograms that were judged as more abnormal by humans also received higher malignancy probability scores.
The finding that agreement between human and SBC scores increased after training has interesting implications. It suggests that the gist of abnormality signal learned by human observers during perceptual training is partially captured by the DNN as well. This adds validity to our findings, as the human observers learned signals that were also detected by an ‘expert’ in the form of a DNN, demonstrating they were able to learn image features of abnormality. Additionally, the finding that the correlation coefficient was markedly higher for the SBC + HM (0.318) than SBC (0.207) suggests that the added heatmap might capture additional perceptual features used by the trained human observers. This suggests that the SBC + HM and similar deep neural networks could be used to investigate the perceptual features in mammograms contributing to the gist signal, for example by performing network dissection, a technique where layers of the network are investigated to extract the content that is activating nodes in these layers (Bau et al., 2020).
Conclusion
In conclusion, perceptual training with global feedback can result in the learning of the gist of a new category, although there are individual differences in both pre-training sensitivity to global structural regularities and ability to further learn the gist signal, and the new gist signal is poorly retained if exposure is not maintained. This suggests that gist categorization might be a case of ‘use it or lose it’, although retention or complete tuning of the visual system to a new category might be obtained after extended exposure. The exposure in our study only amounted to approximately 9 h task time, and 6470 instances viewed with feedback, which is substantially less than in real-world learning of gist categories.
Furthermore, human perceptual expertise on difficult, ambiguous cases containing only global signals of abnormality (contralateral, prior) is still not matched by state-of-the-art neural networks, as indicated by the markedly lower, or even at-chance performance of the DNN on mammograms with global abnormalities that human observers were able to learn in our perceptual training paradigm. The global signal of abnormality is extremely difficult to detect and requires considerable perceptual expertise. On the other hand, we also observed an increase in agreement between the human observers and DNN after perceptual training, which indicates a potential overlap in image statistics used to classify mammograms as normal or abnormal. Finding out what these image statistics are could teach us more about the gist of abnormality and could help find ways to improve image filtering for both human observers and machine learning models. Together, these findings solidly emphasize the need for continued research into medical perceptual expertise with human observers in its own right, especially into more ambiguous global signals that would be vital for early cancer detection. But it also reinforces the need of combining these lines of research with the thriving field of machine learning research, especially since recent research has suggested benefits of combining radiologists’ gist ratings with machine learning models to reach higher levels of performance than either could on their own (Gandomkar et al., 2021; Wurster et al., 2019).
We based our study on drawing a clear parallel between scene gist and the gist of abnormality in radiographs, and it would be beneficial to generalize the current results on learning to a wider area of gist extraction. The parallels between the two types of gist extraction would imply that the current findings of implicit learning should generalize to the learning of scene gist as well. However, as far as the authors are aware, this area has not yet been investigated in the known literature. A potential avenue to answering this question for scene gist could be developmental research with young children, especially as previous research has shown that infants already exhibit signs of statistical learning (Fiser & Aslin, 2002b). However, previous research on the development of rapid perceptual processing is very limited (but see Sweeny et al. (2015). Overall, developmental research often suffers from complications, such as communication of task instructions or difficulties in directing attention, a lack of control over previous exposure, individual differences, and other developmental processes occurring at the same time (Johnson, 2011; Maurer, 2013). These factors make it less suitable to investigate the acquisition of the gist of a novel category.
Overall, the current study shows a strong case for how implicit learning would allow the learning of a new category of any gist, including scenes. What is more, our finding that gist extraction abilities can develop separately from medical knowledge reinforces the viability of the idea, suggested by Voss et al. (2010), of using trained naïve observers, not to ‘usurp’ radiologists’ ratings, but to create a more accessible ‘model observer’ to use for further dissemination of the gist of abnormality signal. This training regime can be used for training of novice radiologists and screening radiographers or even as a refresher training for expert radiologists who over their careers see a considerable reduction in cases they read. Further research is needed to measure the effectiveness of our training paradigm on these populations, and to explore explanatory parameters for individual differences in pre-training performance, learning ability, and learning rate/speed, for example by investigating the potential variation in the length of perceptual training required to achieve perceptual learning across different participants.




