
Abstract
Purpose
To study the role of artificial intelligence (AI) in develo** diabetic macular edema (DME) management recommendations by creating and comparing responses to clinicians in hypothetical AI-generated case scenarios. The study also examined whether its joint recommendations followed national DME management guidelines.
Methods
The AI hypothetically generated 50 ocular case scenarios from 25 patients using keywords like age, gender, type, duration and control of diabetes, visual acuity, lens status, retinopathy stage, coexisting ocular and systemic co-morbidities, and DME-related retinal imaging findings. For DME and ocular co-morbidity management, we calculated inter-rater agreements (kappa analysis) separately for clinician responses, AI-platforms, and the “majority clinician response” (the maximum number of identical clinician responses) and “majority AI-platform” (the maximum number of identical AI responses). Treatment recommendations for various situations were compared to the Indian national guidelines.
Results
For DME management, clinicians (ĸ=0.6), AI platforms (ĸ=0.58), and the ‘majority clinician response’ and ‘majority AI response’ (ĸ=0.69) had moderate to substantial inter-rate agreement. The study showed fair to substantial agreement for ocular co-morbidity management between clinicians (ĸ=0.8), AI platforms (ĸ=0.36), and the ‘majority clinician response’ and ‘majority AI response’ (ĸ=0.49). Many of the current study’s recommendations and national clinical guidelines agreed and disagreed. When treating center-involving DME with very good visual acuity, lattice degeneration, renal disease, anaemia, and a recent history of cardiovascular disease, there were clear disagreements.
Conclusion
For the first time, this study recommends DME management using large language model-based generative AI. The study’s findings could guide in revising the global DME management guidelines.
Similar content being viewed by others


Introduction
Diabetic retinopathy (DR) is one of the many serious eye complications associated with diabetes mellitus [1, 2]. Diabetic macular edema (DME) is one of two reasons for sight-threatening DR, the other being proliferative DR. In India, the prevalence of DME is less than 10% (range: 2.4 − 8.9%) [3,4,5,6]. The absolute number of people with DME in India is significant due to the rising number of diabetics. Various treatment modalities exist for the management of DME, and the selection of treatment depends primarily on the availability of retinal specialists and treatment facilities, as well as the patient’s economic status and underlying ocular and systemic conditions [7]. Because the prevalence of diabetes mellitus, and thus DR and DME, varies across the globe, several countries and regions have developed their own independent guidelines for the screening and management of DR and DME [8,9,10,11,12]. Similarly, the All-India Ophthalmology Society (AIOS) and the Vitreo-Retinal Society of India (VRSI) [national guidelines] have collaborated to develop a consensus statement on the practice points of DME management in India, with the objective of describing the preferred practice patterns for DME management in different clinical situations [13].
Several discussions have centered on the potential advantages and disadvantages of incorporating artificial intelligence (AI) into medicine, including ophthalmology. To date, several papers have been published using deep machine learning-based algorithms to identify and guide DME treatment using color fundus photographs and optical coherence tomography (OCT) images [14,15,16,17]. Concerns have been raised about data acquisition, data bias, identifying ground truth, comparing different algorithms, machine learning challenges, its application to different groups of people, and human barriers to AI adoption in health care [18]. A large language model (LLM) or natural language processing is a form of generative AI algorithm that understands, summarizes, generates, and predicts new text-based content using deep learning techniques and massively large data sets [19]. Many such open source LLM-based generative AI algorithms are currently freely and easily available, including OpenAI’s ChatGPT3.5v and ChatGPT4.0v, BARD from Google, Bing AI from Microsoft, and others [20]. Most researchers and clinicians believe that AIs based on LLM, when integrated into the electronic health record, could aid in the development of the best DME treatment strategy [21]. To the best of our knowledge, we could not find any literature that explored the role of LLM-based AI in DME management.
Thus, the primary objective of this study was to investigate the role of AI in formulating treatment recommendations for DME management by generating and comparing its responses to those of clinicians in different AI-generated clinical case situations. The authors also intended to compare the recommendations obtained collectively by clinicians and different AI platforms to the national guidelines for DME management for the case situations described in this study.
Methods
This was a prospectively conducted questionnaire-based study. The first stage of the study began by asking ChatGPT 3.5v (OpenAI, San Francisco, CA, USA) to generate 25 hypothetical clinical cases involving diabetes mellitus and providing information about the DR and DME status for each eye separately. This was accomplished by instructing the ChatGPT to use the pointers listed below while creating the clinical case. The following pointers were included: (1) patient demographics - age and gender; (2) diabetes type, duration, and control; (3) recent onset visual symptoms; (4) visual acuity (VA) of both eyes in Snellen’s format; (5) lens status - whether clear lens, cataractous lens, pseudophakia, or aphakia; (6) clinical fundus findings description - include cases of both non-proliferative and proliferative disease; (7) presence of systemic co-morbidities such as renal disease, hypertension, anemia, cardiovascular disease, and a deranged lipid profile; (8) co-existing pregnancy for female cases; (9) OCT findings on macular edema location i.e., center-involving DME (CIDME) or non-center-involving DME (NCIDME) and central macular thickness of both eyes, and (10) fundus fluorescein angiography findings on focal or diffuse leakage or macular ischemia, particularly in NCIDME cases.
The AI generated 25 hypothetical clinical patients and 50 clinical ocular case situations. They were then presented in a text format without any clinical images to a group of three experts (NR, NKY, SB) from various institutions to validate the clinical details and imaging findings in the case scenarios in order to make them appear as close to an actual clinical situation as possible. The experts’ recommendations were taken into account. The final version of the questionnaire identified 13 patients with identical ocular findings in both eyes. Thus, a total of 50 hypothetical case scenarios having 37 different ocular situations in 25 virtual patients was available for evaluation and analysis (Supplement 1). The final version of the clinical scenarios was then presented to a second group of five (VP, JC, RKR, PRK, DB) retina specialists/clinicians with at least five years of clinical experience in the field of retina, DR screening, and DME management. These retina specialists worked in a variety of settings, including government hospitals, independent private practices, tertiary eye care hospitals serving both free and paying patients, and tertiary eye care corporate hospitals serving only paying patients. Clinicians were asked to provide the single best treatment option for each eye in the case scenario, while kee** in mind that the patient was visiting the clinician for the first time for treatment and that the focus was on DME and ocular co-morbidity management. Any additional treatment for co-existing ocular co-morbidities like cataract, glaucoma, proliferative DR, etc., had to be mentioned separately as well. The maximum number of identical clinician responses in each category was used to determine the ‘majority DME management response’ and ‘majority ocular co-morbidity management response’ for the clinicians. Following that, the same set of clinical case scenarios was presented to three important AI platforms, which included ChatGPT 3.5v, ChatGPT 4.0v, and Bing AI. The text was fed into various AI platforms in such a way that the ophthalmologist appeared to be asking the AI for the best recommended treatment option based on the most recent available guidelines, with separate answers for each eye. After each case scenario, the AI received no feedback, and the case descriptions were entered sequentially without starting a new chat session. The formal responses for each case scenario were documented separately for DME management and co-existing ocular co-morbidity management based on the results generated by various AI platforms. For each specific case scenario, the ‘majority DME management response’ and ‘majority ocular co-morbidity management response’ were determined by identifying the most identical responses among the three distinct AI platforms in each category separately.
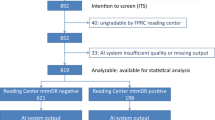
Based on clinician and AI platform responses, a consensus was reached on the most common response for each individual case scenario in order to determine the optimal treatment to be followed by a retina specialist in specific clinical situations. For each specific case scenario, the ‘majority’ DME management and ocular co-morbidity management responses were determined by identifying the response with the highest frequency among clinicians and AI platforms. A total of eight responses were considered, with five coming from clinicians and three from AI platforms (Fig. 1).

Flow chart depicting the methodology process
The AIOS-DR Task Force and the VRSI collectively published a consensus paper on the management of DME. The paper suggested treatment guidelines for DME management in a variety of clinical situations involving ocular and systemic co-morbidities. We looked at the treatment practices recommended by our group of clinicians and different AI platforms for similar clinical situations described in that paper. For that, the clinical situations from our current case list were divided into 4 categories: (a) DME management in cases with NCIDME; (b) DME management in cases with treatment-naïve and previously treated CIDME; (c) DME management in cases with co-existing ocular co-morbidities and (d) DME management in cases with co-existing systemic co-morbidities. The purpose of this exercise was to see if recommendations suggested collectively by the clinicians and different AI platforms were consistent with the National guidelines for DME management.
Given the nature of the study, this research was exempted from further approvals by the institutional review board.
Statistical analysis
The inter-rater reliability agreements among various clinicians, different AI platforms, and the ‘majority response’ for AI and clinician, separately for DME management and co-existing ocular co-morbidity management, were determined using Fleiss Kappa and Cohen’s Kappa (ĸ values) analysis. The calculations were performed on DATAtab: Online Statistics Calculator, developed by DATAtab E.U. in Graz, Austria. The calculator can be accessed at the following URL: https://datatab.net. The Kappa result is interpreted as follows: ĸ values ≤ 0 as indicating no agreement and 0.01–0.20 as none to slight, 0.21–0.40 as fair, 0.41– 0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect agreement [22].
Results
Inter-reliability agreement amongst and between clinicians and different AI platforms for management of DME
The Fleiss kappa test revealed that there was moderate agreement between the five clinicians, with ĸ = 0.60 (95% CI: 0.55–0.65). According to the Fleiss Kappa, there was a moderate agreement between ChatGPT 3.5, ChatGPT 4.0, and Bing AI, with ĸ = 0.58 (95% CI: 0.47–0.69). Cohen’s Kappa revealed a substantial agreement between ‘majority clinician response’ and ‘majority AI response’ for DME management, with ĸ = 0.69 (95% CI: 0.5–0.88). The Cohen’s kappa for the inter-rate reliability agreements between the individual AI platforms and the ‘majority clinician response’ was also calculated. ChatGPT 3.5v, ChatGPT 4.0v, and Bing AI had ĸ values of 0.5 (95% CI: 0.31–0.7), 0.61 (95% CI: 0.41–0.81), and 0.53 (95% CI: 0.34–0.72), respectively.
Inter-reliability agreement amongst and between clinicians and different AI platforms for management of co-existing ocular co-morbidities
There was substantial agreement among the five clinicians for the management of co-existing ocular morbidities, with ĸ=0.80 (95% CI: 0.72–0.88). The Fleiss kappa revealed a fair agreement between ChatGPT 3.5, ChatGPT 4.0, and Bing AI, with ĸ= 0.36 (95% CI: 0.23–0.48). Cohen’s kappa analysis revealed a moderate agreement (ĸ=0.49) between the ‘majority clinician response’ and the ‘majority AI response’. Using Cohen’s kappa analysis, the inter-rater reliability agreements between the individual AI platforms and the ‘majority clinician response’ were calculated. ChatGPT 3.5v, ChatGPT 4.0v, and Bing AI had ĸ values of 0.6, 0.28, and 0.32, respectively (Tables 1 and 2).
Further analysis of case scenarios was performed to determine whether the recommendations for DME management generated jointly by the clinician and AI were consistent with the National guidelines:
-
1.
Management of NCIDME:
In our study, we discovered eight (16%) eyes with NCIDME. These eyes all had 20/30 or better VA. In our study, the most common response for this specific situation was observation (n = 7, 88%) for DME management.
-
2.
Management of CIDME:
This study identified 22 (44%) eyes with CIDME. Half of the eyes (n = 11, 50%) had untreated CIDME, while the others had already been treated. Four (36%) of the eleven eyes had vision better than 20/30, four (36%) had visual acuities between 20/30 and 20/40, and three (28%) had vision worse than 20/50. Treatment with intravitreal injections was advised in three (75%) of the four eyes with VA ≥ 20/30. Intravitreal injections remained the most preferred treatment option for DME management in eyes with visual acuities ranging from 20/30 to 20/40 (3 out of 4 cases, 75%). In eyes with reduced VA, i.e., 20/50, intravitreal pharmacotherapeutic agents were the only treatment option. Only one (12%) of the eight eyes with good VA, i.e., vision acuity ≥ 20/40, had no visual symptoms. Patients reported visual symptoms in the remaining 7 (88%) cases. Treatment was considered in all eight eyes with good VA, regardless of visual complaints, according to the joint recommendations in our study.
The remaining 11 (50%) eyes with CIDME had previously been treated for DME. Six (55%) eyes had very good VA ranging from 20/20 to 20/30, three (27%) eyes had good VA ranging from 20/30 to 20/40, and two eyes (18%) had reduced VA, i.e., worse than 20/50. Two-thirds (4 eyes, 67%) of the eyes with very good VA, i.e., better than 20/30, were treated with intravitreal injections of steroids or anti vascular endothelial growth factors (VEGF) agents. Only intravitreal pharmacotherapeutic agents were used to treat eyes with VA ≤ 20/40.
-
3.
Management of CIDME with co-existing ocular co-morbidities:
Six (27%) of the 22 CIDME eyes also had proliferative DR. In such cases, DME was treated with intravitreal antiVEGF injections in three (50%) eyes, intravitreal steroids in one (17%) eye, and macular laser therapy in two (33%) eyes. Macular laser was preferred in two cases where the patient was pregnant at the time. The current study included six (27%) eyes with pseudophakia and CIDME. Treatment for DME was primarily considered with intravitreal steroid agents in four (67%) eyes and intravitreal antiVEGF agents in two (33%) eyes. The remaining 16 (73%) eyes were all phakic. Significant cataract was found in ten (63%) of the sixteen eyes. The rest of the lenses were clear. Treatment with an intravitreal antiVEGF agent was the only preferred treatment of choice in eyes with significant cataract for the management of DME. Cataract surgery was not considered in any of the ten eyes at the same time as intravitreal injection. None of the eyes with CIDME in the current case list had co-existing glaucoma. In the current case list, there was only one eye (5%) with CIDME that had previously undergone pars plana vitrectomy surgery. There were 2 (9%) eyes in the current study who had CIDME and co-existing peripheral lattice degeneration. Prophylactic barrage laser was not advised in both these cases prior to treatment with intravitreal injections.
-
4.
Management of CIDME with co-existing systemic abnormalities:
There were 15 (68%) eyes with CIDME in the current list of case scenarios that had poor diabetes control, i.e., HbA1c > 6.5%. In none of the clinical situations was DME management withheld in order to achieve metabolic control of diabetes. There were eleven (50%) eyes that had CIDME as well as renal disease and anemia. In such eyes, the most preferred treatment for CIDME was intravitreal antiVEGF agents in 8 eyes (73%) and intravitreal steroids in 3 (27%) eyes. In no case was DME treatment postponed to allow for renal status control. There were 18 (82%) eyes of CIDME with co-existing hypertension on the current list of cases. According to the clinicians’ and AI’s joint recommendations, treatment for CIDME with hypertension in the form of macular laser or intravitreal injections was considered immediately. There were five (23%) eyes with CIDME and a pregnancy. In these eyes, DME was treated with either a macular laser in four (80%) of them or intravitreal steroids in one (20%). In eyes with CIDME and concurrent pregnancy, an intravitreal antiVEGF agent was not considered the best treatment option. Thirteen (43%) of the current cases had DME and a history of cardiovascular disease. Eleven (50%) of these eyes had CIDME, and three (27%) of them had a history of cardiovascular disease within the previous three months. In patients with cardiovascular disease, regardless of its recent history, intravitreal antiVEGF injections were the preferred treatment option.
Discussion
In summary, this one-of-a-kind study involved noting treatment suggestions for DME and ocular co-morbidity management separately to a set of ocular case scenarios generated by the AI, comparing the responses provided by clinicians and different AI platforms to different clinical situations, and finally match the collective responses provided by the different AI platforms and clinicians to different clinical situations with the previously published recommendations by the AIOS-DR Task Force and the VRSI.
The prevalence of DME, as well as the availability of trained medical personnel, retinal imaging tools, and management options, varies by geographic region [4, 23, 24]. Furthermore, treatment practices differ significantly within a defined region based on a variety of factors such as the type of patient (urban versus rural), the patient’s economic status and countries resource settings, and the availability of treatment options such as intravitreal injections or lasers. As a result, different parts of the world establish their own treatment guidelines for DME management [8,9,10,11,12,13]. The International Council of Ophthalmology Guidelines for Diabetic Eye Care 2017 summarised and provided a comprehensive guide for DR screening, referral and follow-up schedules, and appropriate management of vision-threatening DR, including DME and proliferative DR, for countries with high, low, or intermediate resource levels [25]. We found varying levels of agreement among clinicians in this study for the management of DME as well as the management of ocular co-morbidities. The clinicians who participated in this study provided responses from different regions of the country, treating different groups of patients with varying social and economic backgrounds, which explains the varying levels of agreement among the clinicians.
The current role of AI in DME management is primarily limited to identifying and classifying DME using color fundus photographs and/or optical coherence tomography images, as well as predicting the response to antiVEGF therapy using machine learning or deep learning models [14, 15, 26]. Several chatbots developed using LLM-based generative AI applications have shown promising results in generalizing to previously unseen tasks, such as medical question-answering requiring scientific expert knowledge [27,28,29]. LLM understands the medical context, recalls and interprets relevant medical information, and produces a response in a text-based format in order to formulate an answer. Despite mixed results in ophthalmology, LLM appears to have potential for use in eye health care applications. LLM-based generative AI with ChatGPT3.5v and ChatGPT 4.0v has been used in retina for a variety of indications, including ICD for various case encounters [30, 31]. The use of LLM-based generative AI for DME management recommendations in the presence of other ocular co-morbidities has yet to be investigated. Furthermore, different chatbot applications react differently to the same situations [32]. Even in this study, the different AI platforms demonstrated varying levels of agreement for the same clinical case scenario. There was moderate agreement among the different AI platforms for the management of DME and fair agreement for the management of co-existing ocular morbidities. To address this issue, the ‘majority AI response’ was chosen as the preferred method for managing the DME using AI. To improve both the precision and speed of responses, the AI platform must have real-time access to the internet and receive the most up-to-date information. In this study, we discovered that ChatGPT 4.0v performed better and had closer agreements with clinician responses than the other two AI platforms for DME management, while ChatGPT3.5v performed better for co-existing ocular comorbidities management.
A complete ophthalmic examination, as well as a thorough ocular and systemic history, are required for DME management. Most globally accepted treatment guidelines for DME management available in the literature, including protocols developed by the Diabetic Retinopathy Clinical Research Network (DRCR.net), use limited criteria for guiding DME treatment, such as metabolic control status, VA, treatment-naive status, and the involvement of a 1-mm central subfield region on OCT by retinal thickening [8,9,10,11,12,13, 33, 34]. The AIOS-DR Task Force and the VRSI recently published consensus guidelines in 2021 that looked at some additional criteria such as the presence of co-existing ocular and systemic co-morbidities in addition to the above-mentioned criteria when planning DME management [13]. As a result, we compared the recommendations made by the clinicians and AI in this study for various clinical case scenarios to the consensus recommendations made by the AIOS-DR Task Force and the VRSI.
According to the current study recommendations, most eyes with NCIDME and good VA (i.e., 20/30) were only observed or rarely treated with topical non-steroidal anti-inflammatory drugs. According to the recommendations of the AIOS-DR Task Force and the VRSI, eyes with good VA should be observed and followed up on at monthly intervals to look for conversion to CIDME or deterioration in VA [13]. According to protocol R of the DRCR.net, topical non-steroidal anti-inflammatory drugs have no noticeable effect in eyes with NCIDME and good VA [35].
Intravitreal antiVEGF injections are the first line of treatment for naive CIDME [36, 37]. VA is the most important criterion for deciding to initiate treatment, selecting the right intravitreal pharmacotherapeutic antiVEGF agent for its management, and for prognosis purposes, according to most well-established DME treatment guidelines [8,9,10,11,12,13, 33, 34]. According to DRCR.net protocol V, eyes with treatment-naive CIDME and very good VA, i.e., ≥ 20/30, can be observed and followed up on a monthly basis instead of being treated with intravitreal antiVEGF injections [38]. In practice, however, treatment of naive CIDME eyes with very good VA is typically initiated with intravitreal antiVEGF injections only if the patient complains of visual symptoms. Intravitreal antiVEGF agents are typically used to treat naive CIDME eyes with VA below 20/30. The presenting VA also influences the choice of antiVEGF agents; for example, in eyes with acuity ≤ 20/50, intravitreal aflibercept injection is the preferred treatment option [39]. Regardless of presenting VA or patient visual symptoms, intravitreal antiVEGF injection was the only preferred treatment option in the current study recommendations for naive CIDME eyes. In the current study, intravitreal injections, either with antiVEGF agents or steroids, remained the mainstay of DME management for previously treated CIDME eyes. Intravitreal steroids are typically reserved for eyes that have persistent DME or do not respond to monthly antiVEGF injections [40, 41].
Proliferative DR and DME are both distinct patterns of retinal microvascular features indicative of small-vessel disease. Treatment-naive proliferative DR should be treated with pan-retinal photocoagulation, according to the AIOS-DR Task Force and the VRSI guidelines [13]. The presence or absence of vision-threatening traction determines the management regime of CIDME treatment in proliferative DR eyes. Traction that threatens or involves the fovea is an indication for vitrectomy surgery. Intravitreal injections, however, remain the mainstay of DME treatment in the presence of extramacular traction [42]. Intravitreal steroids are usually preferred in proliferative DR and DME eyes with extensive extramacular proliferations because intravitreal antiVEGF injections can worsen traction due to the crunch phenomenon [43]. The current study suggests that eyes with DME and proliferative DR without advanced fibrovascular proliferation be treated with intravitreal antiVEGF injections, whereas intravitreal steroid injections are preferred in DME eyes with proliferative DR and extensive fibrovascular proliferation.
The current study included a high proportion of cases with clear lenses, cataractous lenses, and pseudophakia, all of which co-existed with CIDME. In the absence of a visually disabling cataract, the AIOS-DR Task Force and the VRSI recommend that DME be stabilized first with intravitreal injections. However, in the presence of clinically significant cataracts with a poor view of the fundus, and preexisting DME, surgery along with intravitreal antiVEGF or steroid injections can be planned. In some cases, treatment can be scheduled two weeks after surgery and the subsequent protocol be followed [13]. The current study considered treating DME with intravitreal antiVEGF injections prior to cataract surgery. Vision in the study’s case scenarios ranged from 20/25 to 20/80, indicating moderate vision loss and visually insignificant cataract. This could be the reason why these eyes were treated for DME prior to cataract surgery rather than concurrently with cataract surgery. In the current study, intravitreal steroids were the preferred choice for DME management in pseudophakic eyes in two-thirds of the cases. According to national guidelines, the first step is to determine whether the macular edema in pseudophakic eyes is caused by DME or by Irvine-Gass syndrome. In the presence of DME without the presence of Irvine-Gass syndrome, treatment with antiVEGF injections can be initiated for CIDME, whereas topical or sub tenon’s steroids are recommended as first-line therapy for pseudophakic edema. Topical nonsteroidal anti-inflammatory drugs should be used first, followed by antiVEGF, in the presence of both DME and Irvine-Gass syndrome. It is reasonable to switch to steroids in eyes that have not responded to previous antiVEGF injections (after 3–6 injections) [13]. Many international experts around the world believe that intravitreal steroids injection with dexamethasone implant is a viable alternative first-line treatment option, particularly in pseudophakic eyes [44].
National guidelines recommend treating DME in eyes with established glaucoma, ocular hypertension, or steroid responders with either macular laser or antiVEGF injections. In these patients, steroids should be avoided [13]. There were no cases of CIDME and co-existing glaucoma in the current study’s case scenarios. As a result, comparisons with the National guidelines were not possible in this study. According to experts affiliated with the National guidelines, careful examination of the retinal periphery for identifying lesions that may predispose to retinal detachment, as well as prophylactic barrage laser treatment of those lesions, is recommended. In addition, the time between laser prophylaxis and antiVEGF injections should ideally be three weeks [13]. However, the current study’s joint experts (AI and clinicians) did not recommend prophylactic laser barrage to lattice degenerations prior to beginning DME treatment with intravitreal injections.
DME treatment in a vitrectomised eye is difficult. There is limited data on the preferred agent for treatment in these eyes. Furthermore, as the environment of the vitreous cavity changes, the pharmacokinetic parameters of antiVEGF may be affected. A recent study comparing the efficacy of ranibizumab injections for the treatment of DME in eyes with and without previous vitrectomy over a two-year period found similar results [45]. In a similar study, Koyanagi et al. found no significant differences in the mean changes in VA and central macular thickness between the two groups after 6 months [46]. However, some studies show that intravitreal antiVEGF injections have a lower efficacy in vitrectomised eyes [47]. Intravitreal dexamethasone implant has also been shown to be effective in both vitrectomised and non-vitrectomised eyes [48, 49]. Thus, current evidence suggests that both antiVEGF and steroids have a role in the treatment of DME in vitrectomised eyes.
Poor glycemic control is a risk factor for the progression of DR and DME. Strict glycemic control is beneficial at any stage of diabetes. Poor or fluctuating glycemic control can affect adherence to monthly intravitreal injections. However, in order to achieve good glycemic control, DME management should not be delayed. In the current study, DME management was not postponed in cases of poor diabetes control.
Little is known about the treatment of DME during pregnancy [50]. According to experts, watchful waiting may be used in cases of mild to moderate DME because the outcomes are similar in patients who receive prompt versus delayed DME treatment [51]. Because of potential adverse effects on develo** embryos or foetuses, intravitreal antiVEGF injections are not recommended during pregnancy. Women should therefore wait at least three months after their last intravitreal injection before conceiving. Ranibizumab is usually preferred over other antiVEGF agents because of its shorter half-life and faster plasma clearance [52]. When the disease permits it, focal laser or intravitreal steroids are the preferred treatment options for DME in pregnancy [50, 51].
The current study’s clinicians and AI jointly proposed the use of intravitreal antiVEGF or steroid injection in eyes with CIDME and deranged renal status. Diabetic nephropathy is often associated with other systemic co-morbidities that affect DME. Secondary hypertension, anemia, patients on or after dialysis, and renal transplantation, for example, may all have an impact on the presence of DME and its management [53,54,55]. VEGF inhibitors may have nephrotoxic effects, according to emerging evidence [56]. However, a recent study published by Ku et al. found no correlation between the use of intravitreal antiVEGF injections and a decrease in estimated glomerular filtration rate [57]. Several DME treatment guidelines recommend identifying the cause of hypertension and controlling it before beginning treatment with intravitreal antiVEGF injections [8, 9, 12, 13]. AntiVEGF injections are effective in eyes with DME and well-controlled hypertension [58]. According to studies, patients with DME or proliferative DR are more likely to have incident or fatal cardiovascular disease than those who do not have DME or PDR [59]. If a patient has had a stroke or myocardial infarction within the previous 3 months, the AIOS-DR Task Force and the VRSI recommend that antiVEGF treatment be avoided; instead, PRP or steroid treatments should be considered in these patients [13]. However, a recent systematic review and meta-analysis published by Ngo Ntjam et al. examined the incidence of major cardiovascular adverse events in patients receiving intravitreal administration of anti-vascular endothelial growth factor drugs. They confirmed that intravitreal antiVEGF injections did not cause serious cardiovascular events [60]. Even in this study, intravitreal antiVEGF injections were the preferred treatment option in DME patients with a history of cardiovascular disease. Table 3 summarizes study’s joint recommendations for managing DME and provides comparisons with the national recommendations for DME management.
There are a few weaknesses with this study. Regarding the clinical case scenarios generated by the AI, the number of case scenarios provided could have been greater, taking into account all possible permutations and combinations involving the DME status, as well as the ocular and systemic co-morbidity status. The clinical case scenarios could have been presented to a larger group of clinicians on a national and international scale, as well as to multiple AI applications. The term ‘majority’ clinician and AI responses used in this study may mislead readers and be misinterpreted as the best response from the entire fraternity of retina specialists and different AI platforms. In the current study, the AI and clinician responses were only compared to the National guidelines proposed by a group of experts affiliated with the AIOS-DR Task Force and the VRSI. The current study’s recommendations could have been compared to international DME management guidelines, making the study’s findings more globally acceptable. Nonetheless, the study has the advantage of adding a completely new dimension to the formulation of DME treatment guidelines by incorporating the role of LLM-based generative AI. The study also emphasizes the importance of considering the patient’s eye and body as a whole when planning DME management. It is possible to make these recommendations globally acceptable by addressing the aforementioned flaws in future DME and AI-related studies. Furthermore, in the future, these globally acceptable DME management recommendations could be integrated with the hospital’s electronic medical record system, alerting ophthalmologists to the best possible treatment option after considering the various factors that may influence DME developments and management. The AI has the capability to analyse and assess its recommendations based on the specific approaches used by different clinicians for managing DME by setting up prompts on the electronic medical record. In the future, AI will incorporate self-learning algorithms tailored to each clinician’s practices, allowing the algorithm to learn from a clinician’s recommendations for a particular patient. This adaptive learning process will help enhance the algorithm’s performance.
In conclusion, this study highlights the significance of AI in aiding experts in revising the existing treatment guidelines for managing DME. An optimal approach for the future would involve merging these treatment guidelines with the hospital’s electronic medical record software, enabling clinicians to promptly select the most effective treatment option for managing DME.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DME:
-
diabetic macular edema
- DR:
-
diabetic retinopathy
- AI:
-
artificial intelligence
- LLM:
-
large language model
- AIOS:
-
All-India Ophthalmological Society
- VRSI:
-
Vitreo-Retina Society of India
- OCT:
-
optical coherence tomography
- VA:
-
visual acuity
- CIDME:
-
center-involving diabetic macular edema
- NCIDME:
-
non-center involving diabetic macular edema
- VEGF:
-
vascular endothelial growth factor
- DRCR.net:
-
Diabetic Retinopathy Clinical Research Network
References
Sayin N. Ocular complications of diabetes mellitus. WJD. 2015;6:92.
Vieira-Potter VJ, Karamichos D, Lee DJ. Ocular complications of diabetes and therapeutic approaches. Biomed Res Int. 2016;2016:1–14.
Raman R, Rani PK, Reddi Rachepalle S, Gnanamoorthy P, Uthra S, Kumaramanickavel G, et al. Prevalence of diabetic retinopathy in India: Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetics Study report 2. Ophthalmology. 2009;116:311–8.
Raman R, Vasconcelos JC, Rajalakshmi R, Prevost AT, Ramasamy K, Mohan V, et al. Prevalence of diabetic retinopathy in India stratified by known and undiagnosed diabetes, urban–rural locations, and socioeconomic indices: results from the SMART India population-based cross-sectional screening study. Lancet Global Health. 2022;10:e1764–73.
Rema M, Premkumar S, Anitha B, Deepa R, Pradeepa R, Mohan V. Prevalence of diabetic retinopathy in urban India: the Chennai Urban Rural Epidemiology Study (CURES) eye study, I. Invest Ophthalmol Vis Sci. 2005;46:2328–33.
Narendran V, John RK, Raghuram A, Ravindran RD, Nirmalan PK, Thulasiraj RD. Diabetic retinopathy among self reported diabetics in southern India: a population based assessment. Br J Ophthalmol. 2002;86:1014–8.
Mathew C, Yunirakasiwi A, Sanjay S. Updates in the management of Diabetic Macular Edema. J Diabetes Res. 2015;2015:1–8.
Bakri SJ, Wolfe JD, Regillo CD, Flynn HW, Wykoff CC. Evidence-based guidelines for management of Diabetic Macular Edema. J VitreoRetinal Dis. 2019;3:145–52.
Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, Berg K, Chakravarthy U, Gerendas BS, et al. Guidelines for the management of Diabetic Macular Edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237:185–222.
Elyasi N, Hemmati H. Diabetic Macular Edema: Diagnosis and Management [Internet]. 2024. Available from: https://www.aao.org/eyenet/article/diabetic-macular-edema-diagnosis-and-management#:~:text=If%20VA%20is%20better%20than,anti%2DVEGF%20therapy%20with%20aflibercept.
AlQahtani AS, Hazzazi MA, Waheeb SA, Semidey VA, Semidey VA, Elgendy HK, et al. Saudi Arabia Guidelines for diabetic macular edema: a consensus of the Saudi Retina Group. Saudi Med J. 2021;42:131–45.
Chhablani J, Wong K, Tan GS, Sudhalkar A, Laude A, Cheung CMG, et al. Diabetic Macular Edema Management in Asian Population: Expert Panel Consensus guidelines. Asia-Pacific J Ophthalmol. 2020;9:426–34.
Giridhar S, Verma L, Rajendran A, Bhend M, Goyal M, Ramasamy K, et al. Diabetic macular edema treatment guidelines in India: All India Ophthalmological Society Diabetic Retinopathy Task Force and Vitreoretinal Society of India consensus statement. Indian J Ophthalmol. 2021;69:3076.
Shahriari MH, Sabbaghi H, Asadi F, Hosseini A, Khorrami Z. Artificial intelligence in screening, diagnosis, and classification of diabetic macular edema: a systematic review. Surv Ophthalmol. 2023;68:42–53.
Chakroborty S, Gupta M, Devishamani CS, Patel K, Ankit C, Ganesh Babu TC, et al. Narrative review of artificial intelligence in diabetic macular edema: diagnosis and predicting treatment response using optical coherence tomography. Indian J Ophthalmol. 2021;69:2999–3008.
Li L, Zhang W, Tu X, Pang J, Lai IF, ** C, et al. Application of Artificial Intelligence in Precision Medicine for Diabetic Macular Edema. Asia-Pacific J Ophthalmol. 2023;12:486–94.
Midena E, Toto L, Frizziero L, Covello G, Torresin T, Midena G, et al. Validation of an automated Artificial Intelligence Algorithm for the quantification of major OCT parameters in Diabetic Macular Edema. JCM. 2023;12:2134.
Raman R, Dasgupta D, Ramasamy K, George R, Mohan V, Ting D. Using artificial intelligence for diabetic retinopathy screening: policy implications. Indian J Ophthalmol. 2021;69:2993–8.
Types of artificial intelligence. https://www.javatpoint.com/types-of-artificial-intelligence.
Open Source Large Language Models (LLM. https://spotintelligence.com/2023/06/05/open-source-large-language-models/) [Internet]. [cited 2023 Nov 15]. Available from: https://spotintelligence.com/2023/06/05/open-source-large-language-models/.
Yu P, Xu H, Hu X, Deng C. Leveraging generative AI and large Language models: a Comprehensive Roadmap for Healthcare Integration. Healthc (Basel). 2023;11:2776.
McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22:276–82.
Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis (Lond). 2015;2:17.
Lundeen EA, Andes LJ, Rein DB, Wittenborn JS, Erdem E, Gu Q, et al. Trends in Prevalence and Treatment of Diabetic Macular Edema and Vision-threatening Diabetic Retinopathy among Medicare Part B fee-for-service beneficiaries. JAMA Ophthalmol. 2022;140:345.
Wong TY, Sun J, Kawasaki R, Ruamviboonsuk P, Gupta N, Lansingh VC, et al. Guidelines on Diabetic Eye Care. Ophthalmology. 2018;125:1608–22.
Kalavar M, Al-Khersan H, Sridhar J, Gorniak RJ, Lakhani PC, Flanders AE, et al. Applications of Artificial Intelligence for the detection, management, and treatment of Diabetic Retinopathy. Int Ophthalmol Clin. 2020;60:127–45.
Raimondi R, Tzoumas N, Salisbury T, Di Simplicio S, Romano MR et al. North East Trainee Research in Ophthalmology Network (NETRiON),. Comparative analysis of large language models in the Royal College of Ophthalmologists fellowship exams. Eye [Internet]. 2023 [cited 2023 Nov 18]; Available from: https://www.nature.com/articles/s41433-02302563-3.
Lin JC, Younessi DN, Kurapati SS, Tang OY, Scott IU. Comparison of GPT-3.5, GPT-4, and human user performance on a practice ophthalmology written examination. Eye [Internet]. 2023 [cited 2023 Nov 18]; Available from: https://www.nature.com/articles/s41433-023-02564-2.
Antaki F, Touma S, Milad D, El-Khoury J, Duval R. Evaluating the performance of ChatGPT in Ophthalmology. Ophthalmol Sci. 2023;3:100324.
Ong J, Hariprasad SM, Chhablani J, ChatGPT. GPT-4 in Ophthalmology: applications of large Language Model Artificial intelligence in Retina. Ophthalmic Surg Lasers Imaging Retina. 2023;54:557–62.
Ong J, Kedia N, Harihar S, Vupparaboina SC, Singh SR, Venkatesh R, et al. Applying large language model artificial intelligence for retina international classification of diseases (ICD) coding. J Med Artif Intell. 2023;6:21–1.
ChatGPT vs. Bing vs. Google Bard: Which AI Is the Most Helpful? https://www.cnet.com/tech/services-and-software/chatgpt-vs-bing-vs-google-bard-which-ai-is-the-most-helpful/ Accessed on 18th Nov 2023. [cited 2023 Nov 18]; Available from: https://www.cnet.com/tech/services-and-software/chatgpt-vs-bing-vs-google-bard-which-ai-is-the-most-helpful/.
Sun JK, Jampol LM. The Diabetic Retinopathy Clinical Research Network (DRCR.net) and its contributions to the treatment of Diabetic Retinopathy. Ophthalmic Res. 2019;62:225–30.
Diabetic Retinopathy Clinical Research Retina Network [Internet]. Available from: https://public.jaeb.org/drcrnet/pubs.
Friedman SM, Almukhtar TH, Baker CW, Glassman AR, Elman MJ, Bressler NM, et al. Topical nepafenec in eyes with noncentral diabetic macular edema. Retina. 2015;35:944–56.
Diabetic Retinopathy Clinical Research Network, Committee W, Aiello LP, Beck RW, Bressler NM, Browning DJ, et al. Rationale for the diabetic retinopathy clinical research network treatment protocol for center-involved diabetic macular edema. Ophthalmology. 2011;118:e5–14.
Wenick AS, Bressler NM. Diabetic macular edema: current and emerging therapies. Middle East Afr J Ophthalmol. 2012;19:4–12.
Baker CW, Glassman AR, Beaulieu WT, Antoszyk AN, Browning DJ, Chalam KV, et al. Effect of initial management with Aflibercept vs Laser Photocoagulation vs Observation on Vision loss among patients with Diabetic Macular Edema Involving the Center of the Macula and Good Visual Acuity: a Randomized Clinical Trial. JAMA. 2019;321:1880.
The Diabetic Retinopathy Clinical Research Network. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema. N Engl J Med. 2015;372:1193–203.
Maturi RK, Glassman AR, Liu D, Beck RW, Bhavsar AR, Bressler NM, et al. Effect of adding dexamethasone to continued Ranibizumab treatment in patients with Persistent Diabetic Macular Edema: a DRCR Network Phase 2 Randomized Clinical Trial. JAMA Ophthalmol. 2018;136:29.
Regillo CD, Callanan DG, Do DV, Fine HF, Holekamp NM, Kuppermann BD, et al. Use of corticosteroids in the treatment of patients with Diabetic Macular Edema who have a suboptimal response to Anti-VEGF: recommendations of an Expert Panel. Ophthalmic Surg Lasers Imaging Retina. 2017;48:291–301.
Gündüz K, Bakri SJ. Management of proliferative diabetic retinopathy. Compr Ophthalmol Update. 2007;8:245–56.
Tan Y, Fukutomi A, Sun MT, Durkin S, Gilhotra J, Chan WO. Anti-VEGF crunch syndrome in proliferative diabetic retinopathy: a review. Surv Ophthalmol. 2021;66:926–32.
Spinetta R, Petrillo F, Reibaldi M, Tortori A, Mazzoni M, Metrangolo C, et al. Intravitreal DEX Implant for the Treatment of Diabetic Macular Edema: a review of National Consensus. Pharmaceutics. 2023;15:2461.
Gedar Totuk OM, Kanra AY, Bromand MN, Kilic Tezanlayan G, Ari Yaylalı S, Turkmen I, et al. Effectiveness of Intravitreal Ranibizumab in Nonvitrectomized and Vitrectomized eyes with Diabetic Macular Edema: a two-year retrospective analysis. J Ophthalmol. 2020;2020:1–8.
Koyanagi Y, Yoshida S, Kobayashi Y, Kubo Y, Yamaguchi M, Nakama T, et al. Comparison of the effectiveness of Intravitreal Ranibizumab for Diabetic Macular Edema in Vitrectomized and Nonvitrectomized eyes. Ophthalmologica. 2016;236:67–73.
Chen Y-Y, Chen P-Y, Chen F-T, Chen Y-J, Wang J-K. Comparison of efficacy of intravitreal ranibizumab between non-vitrectomized and vitrectomized eyes with diabetic macular edema. Int Ophthalmol. 2018;38:293–9.
Özdemir HB, Hasanreisoğlu M, Yüksel M, Ertop M, Gürelik G, Özdek Ş. Effectiveness of Intravitreal Dexamethasone Implant Treatment for Diabetic Macular Edema in Vitrectomized eyes. Turk J Ophthalmol. 2019;49:323–7.
Zambarakji H, Papastefanou V, Dooley I. Steroids agents in the management of vitrectomized eyes with diabetic macular edema. Acta Ophthalmol. 2015;93:j1755–376820150032.
Morrison JL, Hodgson LA, Lim LL, Al-Qureshi S. Diabetic retinopathy in pregnancy: a review. Clin Exp Ophthalmol. 2016;44:321–34.
Mir TA, Finn AP. Pregnancy and diabetic retinopathy—considerations for evaluation and treatment: a review. Ann Eye Sci. 2023;8:14–4.
Naderan M, Sabzevary M, Rezaii K, Banafshehafshan A, Hantoushzadeh S. Intravitreal anti-vascular endothelial growth factor medications during pregnancy: current perspective. Int Ophthalmol. 2021;41:743–51.
Ou S-H, Chang W-C, Wu L-Y, Wang S-I, Wei JC-C, Lee P-T. Diabetic macular oedema is predictive of renal failure in patients with diabetes mellitus and chronic kidney disease. J Clin Endocrinol Metab. 2023;dgad581.
Lim AK. Diabetic nephropathy - complications and treatment. Int J Nephrol Renovasc Dis. 2014;7:361–81.
Roy R, Das MK, Pal BP, Ganesan S, Raman R, Sharma T. The effects of renal transplantation on diabetic retinopathy: clinical course and visual outcomes. Indian J Ophthalmol. 2013;61:552–6.
Hanna RM, Barsoum M, Arman F, Selamet U, Hasnain H, Kurtz I. Nephrotoxicity induced by intravitreal vascular endothelial growth factor inhibitors: emerging evidence. Kidney Int. 2019;96:572–80.
Ku W-N, Tien P-T, Lin C-J, Chiang C-C, Hsia N-Y, Lai C-T, et al. Changes of estimated glomerular filtration rate and glycated hemoglobin A1c in Diabetic Macular Edema patients treated by Ranibizumab and Aflibercept in the Tertiary Referral Hospital. Med (Kaunas). 2022;58:1081.
Shah AR, Van Horn AN, Verchinina L, Wichorek M, Su L, Markel D, et al. Blood pressure is Associated with receiving Intravitreal Anti-vascular endothelial growth factor treatment in patients with diabetes. Ophthalmol Retina. 2019;3:410–6.
Hsu C-Y, Lee C-M, Chou K-Y, Lee C-Y, Chen H-C, Chiou J-Y, et al. The Association of Diabetic Retinopathy and Cardiovascular Disease: a 13-Year Nationwide Population-based Cohort Study. Int J Environ Res Public Health. 2021;18:8106.
Ngo Ntjam N, Thulliez M, Paintaud G, Salvo F, Angoulvant D, Pisella P-J, et al. Cardiovascular adverse events with Intravitreal Anti-vascular endothelial growth factor drugs: a systematic review and Meta-analysis of Randomized clinical trials. JAMA Ophthalmol. 2021;139:1–11.
Acknowledgements
None.
Funding
No funds, grants or other supports was received.
Author information
Authors and Affiliations
Contributions
RV, RS– conceptualising the study, data acquisition, analysing the data, statistics and results, interpreting the findings, writing & reviewing the manuscript. NG, SB, NKY– validating the questionnaire generated by the AI platform. VP, RPK, JC, DB, RKR– Clinicians responding to the final clinical case scenarios. NG, AJ, AC, PG– collecting the AI responses and collating and analysing the clinician responses. RS– critically reviewing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval and consent to participate
The study was exempted from seeking further approvals from the Institutional research board and Ethics committee.
Consent for publication
As the study was questionnaire format-based study, a waiver for was obtained from the IRB and EC of the institution regarding the consent for publication.
Plant reproducibility
Not applicable.
Animal research
This article does not contain any studies with animals performed by any of the authors.
Clinical trials registration
Not applicable.
Gel and blots/image manipulation
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Choudhary, A., Gopalakrishnan, N., Joshi, A. et al. Recommendations for diabetic macular edema management by retina specialists and large language model-based artificial intelligence platforms. Int J Retin Vitr 10, 22 (2024). https://doi.org/10.1186/s40942-024-00544-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40942-024-00544-6