
Abstract
Background
Digoxin is an important treatment option for reducing the ventricular rate in patients with atrial fibrillation (AF) and heart failure (HF). Digoxin has a narrow therapeutic window and large interindividual variability. A low target blood concentration, especially ≤0.9 ng/mL, is recommended for patients with HF who are taking digoxin. This study aimed to develop a population pharmacokinetic model and to identify clinical factors that affect digoxin exposure and an optimal digoxin dosing regimen in Japanese patients with AF and HF.
Methods
A population pharmacokinetic analysis was performed by using a nonlinear mixed effects model based on 3465 concentration points from 391 patients (>18 years) who were receiving oral digoxin. Using trough serum digoxin concentrations and clinical data, a population pharmacokinetic model was developed for determining covariates of clearance. A 1-compartment model was used to examine the interindividual variability of the oral clearance (CL/F) of digoxin. An appropriate dosage of digoxin was identified using Monte Carlo simulation.
Results
The final model demonstrated that creatinine clearance (CLCR) and the use of amiodarone were factors that contributed to the CL/F of digoxin. Monte Carlo simulation results showed that with a daily maintenance dose of 0.25 mg, the intoxication risk window of a trough serum concentration of ≥0.9 ng/mL could be reached in more than half of patients regardless of renal function category or concurrent use of amiodarone. The appropriate maintenance dosage was 0.125 mg daily for most Japanese patients with AF and HF. However, with a daily dose of 0.125 mg, a trough serum concentration of ≥0.9 ng/mL could be reached in more than half of patients with renal impairments (CLCR 30 mL/min) or concurrent use of amiodarone. A daily maintenance dose of 0.0625 mg was acceptable for these patients.
Conclusions
CLCR and the use of amiodaron were found to contribute to digoxin clearance using a population pharmacokinetic methodology. For Japanese patients with AF and HF, 0.125 mg is an appropriate daily digoxin maintenance dose, but a dose reduction is required for patients with CLCR <30 mL/min or concurrent amiodarone use.
Similar content being viewed by others


Background
Digoxin is an important treatment option for reducing the ventricular rate in patients with atrial fibrillation (AF) and heart failure (HF) although it is recommended as a second-line treatment [1, 2]. Digoxin has sympathoinhibitory and vagomimetic effects, which delay atrioventricular nodal conduction, leading to a reduction in the ventricular rate, as well as a positive inotropic effect [3]. The effect of digoxin on rate control with no deterioration of haemodynamic status may be appropriate for AF that is associated with systolic HF. However, adverse outcomes of digoxin limit its benefit in practice [4, 5].
Digoxin has a narrow therapeutic window [6]. High blood digoxin concentrations are a risk factor for digitalis intoxication [7,8,9,10], and the incidence of digitalis intoxication can be decreased when the digoxin dosage is adjusted based on blood digoxin concentrations [11, 12]. Moreover, a high blood digoxin concentration (≥1.2 ng/mL) is reported to be associated with a risk of mortality in patients with HF and even in patients with AF [13, 14]. Therefore, a low target blood concentration is now recommended for patients who are taking digoxin, especially ≤0.9 ng/mL, which is preferable for systolic HF [15].
Digoxin shows interindividual variability in pharmacokinetics, with a large volume distribution, mainly skeletal muscle distribution, and renal elimination through glomerular filtration and tubular secretion [16]. Various factors, including renal function and concurrent use of P-glycoprotein inhibitors, such as amiodarone and verapamil, have been reported to impact digoxin renal clearance [6, 17]. Because Japanese individuals show smaller body weights and decreased creatinine generation compared to individuals in the US and Europe [18], dosage adjustment is required based on a pharmacokinetic model of Japanese parameters. There have been no reports on dosage adjustment of digoxin in Japanese patients with AF and HF for whom digoxin is indicated. Population pharmacokinetics is a method of expressing pharmacokinetic properties in a target population from clinical data, including blood drug concentration, which involves estimation using nonlinear mixed-effects models that were developed by Sheiner and Beal [19, 20]. The present study aimed to develop a population pharmacokinetic model and to identify clinical factors that affect digoxin exposure and an optimal maintenance digoxin dosing regimen in patients with AF and HF.
Methods
Subjects
We conducted a cohort study of 391 consecutive patients with AF and HF aged 18 years and older who were taking oral digoxin at Tokyo Women’s Medical University Hospital between January 2008 and December 2016. To identify patients who were prescribed digoxin and in whom digoxin serum concentrations were measured, we first searched the automated outpatient accounting databases. Then, we confirmed that the identified patients had been diagnosed with AF and HF by checking medical records. HF was defined according to the American College of Cardiology/American Heart Association criteria [21]; the patients in our study were designated as stage C (current or prior symptoms of HF) or stage D (refractory HF). We excluded patients who were receiving methyldigoxin or patients whose trough concentration of digoxin was not measured. Details of the study design and data collection have been previously reported [10]. The protocol was approved by the institutional review boards of Tokyo Women’s Medical University and Jikei University.
Data collection
The collected data from electronic medical records included demographic data (sex, age, height, body weight, and body mass index), left ventricular ejection fraction, New York Heart Association (NYHA) functional class, underlying heart disease, clinical laboratory data (serum creatinine), and data on digoxin (dosage and trough serum concentration) and concurrent potent P-glycoprotein inhibitor medications (amiodarone, diltiazem, and verapamil). Data collection covered the period between the initiation of oral digoxin therapy and the last measurement of the digoxin trough serum concentration or January 31, 2018. Renal function was assessed using the creatinine clearance (CLCR) and the estimated glomerular filtration rate (eGFR). CLCR was calculated with the Cockcroft-Gault equation [22]. The eGFR was calculated with the Japanese version of the Modification of Diet in Renal Disease formula [18]. The serum digoxin concentration was assayed using the COBAS TDM system (Roche Diagnostics K.K., Tokyo, Japan) by the kinetic interaction of microparticles in a solution until November 2016. The detection limit of this assay was 0.3 ng/mL. The standard curves for digoxin were linear from 0.3 to 5.0 ng/mL. After that, the serum digoxin concentration was measured using the Nanopia TDM system (SEKISUI MEDICAL CO., LTD, Tokyo, Japan) by latex coagulating nephelometry. This assay had a detection limit of 0.05 ng/mL. The standard curves for digoxin were linear from 0.2 to 5.0 ng/mL. Digoxin concentrations that were measured at least 6 h after the last administration were used to develop a population pharmacokinetic model of the trough serum concentration [15]. All trough concentrations were regarded as steady-state concentrations because the trough concentrations were measured 5 days after the start of digoxin administration.
Population pharmacokinetic model development
The population pharmacokinetic model was developed with a nonlinear mixed effects model using Phoenix NLME™ software (version 8.1, Certara USA, Inc., Princeton, NJ, USA). The base model was a one-compartment model with first-order absorption. Serum concentrations below measurable limits were not used to develop the population pharmacokinetic model. Because we could not obtain serum digoxin concentrations except for trough concentrations, the absorption rate constant was fixed to 1.0 h− 1 to reflect the assumption that digoxin was absorbed fast irrespective of P-glycoprotein function [23]. In addition, the apparent volume of distribution (Vd) was fixed to 6.0 L/kg according to a previous study [24]. Because we could not estimate the absolute bioavailability, the oral clearance (CL/F) was estimated. The intraindividual variability was compared using an additive error model and a multiplicative error model, which were defined as follows:
where Cobs and Cpred denote the observed and predicted serum digoxin concentrations, respectively, and ε denotes the measurement error, which includes the intraindividual variability, analytical error, and dosing error. We assessed using the objective function value. The difference of 3.84 in the objective function value between these models was statistically significant (p < 0.05).
The interindividual variability of the oral clearance of digoxin was described using an exponential random effects model, which was defined as follows:
where CL/F denotes the parameter for digoxin oral clearance, tv CL/F is the typical value of oral clearance and η represents the interindividual variability of CL/F. We used a stepwise forward selection method to assess the impacts of covariates on the CL/F of digoxin. The potential covariates were demographic data (sex, age, and body mass index), renal function (CLCR and eGFR), and concurrent medications (amiodarone, diltiazem, and verapamil). Continuous covariates were normalized by their typical values. If CLCR was estimated to be above 120 mL/min, it was replaced with 120 mL/min to avoid the overestimation of renal clearance. Sex and concurrent medications were regarded as categorical covariates. Potential covariates were incorporated one by one into the base model and assessed using the value of the objective function that is mentioned above. Initially, potential covariates that produced the minimum value of the objective function were screened and added to the base model. After the selection of a potential covariate, we explored whether the addition of this potential covariate improved the model performance in the same manner. If we detected multicollinearity of covariates, we chose a covariate according to both the minimum value of the objective function and the clinical relevance.
Population pharmacokinetic model evaluation
We evaluated the fit and robustness of the final model using goodness-of-fit plots and bootstrap methods. The final model fit was evaluated by scatter plots of observed vs. predicted concentrations, observed vs. individual predicted concentrations, conditional weighted residuals vs. predicted concentrations, and conditional weighted residuals vs. time after the first dose. Using a bootstrap method, 1000 samples were generated by random resampling of the original dataset. The final model parameters of the 1000 generated samples were compared to those from the original dataset.
Simulations
Monte Carlo simulation was performed every 1000 iterations using the final model to identify an optimal dosing regimen at various daily doses (0.25 mg, 0.125 mg, and 0.0625 mg). This simulation was performed using a lognormal distribution based on the interindividual variation that was obtained by population pharmacokinetic analysis. Predicted serum digoxin concentrations were compared according to CLCR (90 mL/min, 60 mL/min, and 30 mL/min) and with or without concurrent use of amiodarone. Serum digoxin concentrations of ≥0.9 ng/mL and ≥1.2 ng/mL were defined as trough concentrations above the target range because these cut points of clinical interest were used in previous studies of patients with HF [13, 25]. We calculated the probabilities of trough serum digoxin concentrations being ≥0.9 ng/mL and ≥1.2 ng/mL.
Statistical analysis
Continuous data are presented as the mean ± standard deviation (SD) for those with a normal distribution or as the median and interquartile range for those with a nonnormal distribution unless otherwise specified. Categorical data are presented as numerical values (%). Data analyses were performed using JMP Pro statistical software (version 14, SAS Institute Inc., Cary, NC, USA).
Results
Study population
The clinical features of the study population are listed in Table 1. The mean age was 67 ± 14 years, and the median CLCR was 56.5 [40.7–75.6] mL/min. Among the 391 patients, 312 (80%) had permanent/persistent AF, and 100 (26%) were of NYHA functional class III or IV. Regarding underlying heart disease, nonischaemic aetiologies, including cardiomyopathies and valvular disease were common in our patients. Approximately 70% of patients received a daily dose of 0.125 mg digoxin. The median treatment duration was 350 [60–1340] days. Amiodarone was the most common concurrent P-glycoprotein inhibitor.
Regarding clinical outcomes, the relationships between the events and values of digoxin concentration immediately after or before (within 3 months) the occurrence of the events are presented in Table 2. Regarding the cause of death, the incidence of cardiac death did not increase with increased serum concentrations of digoxin. The incidence of noncardiac death increased in patients with serum digoxin concentration of ≥0.90 ng/mL. Regarding the type of digoxin intoxication that occurred, cardiac disturbance was observed in all of the concentration groups, whereas gastrointestinal symptoms were observed only in patients with serum digoxin concentrations of ≥0.90 ng/mL.
Population pharmacokinetic model development
A total of 3465 digoxin trough serum concentrations from 391 patients were used in the following analysis. At the first measurement of the trough digoxin concentration, the median serum concentration was 0.77 [0.52–1.02] ng/mL. The median number of measurements for each patient was 5 [2,3,4,5,6,7,8,9,10,11,12].
A one-compartment model and first-order absorption with a multiplicative error model were found to best describe the trough serum digoxin concentrations. The stepwise forward selection method identified the following potential covariates of CL/F: body mass index, CLCR, eGFR, use of amiodarone, and use of diltiazem. Among them, CLCR produced the minimum objective function value and was included in the base model. After adding CLCR to the base model, concurrent use of amiodarone yielded the maximum reduction of the objective function value, which was significant. There remained no clear relationships in the final model between the random effect for CL/F and other covariates, such as sex, age, height, and body mass index (Supplemental Fig.). Thus, CLCR and concurrent use of amiodarone were established as covariates of CL/F and included in the final model of digoxin (Table 3).
The estimated mean oral clearance (relative standard error, %) was 6.2 L/h (2.8%). The final model for CL/F was defined as follows:
where 0.41 is the exponential coefficient for CLCR and 0.24 is the fractional change (decrease) for concurrent use of amiodarone.
Population pharmacokinetic model evaluation
Scatter plots of observed vs. predicted concentrations (Fig. 1A), observed vs. individual predicted concentrations (Fig. 1B), conditional weighted residuals vs. predicted concentrations (Fig. 1C), and conditional weighted residuals vs. time after the first dose (Fig. 1D) did not show any systematic bias.

Goodness-of-fit scatter plots for the final population pharmacokinetic model. A. Observed concentrations (DV) vs. predicted concentrations (PRED); the solid line represents the reference line. B. Observed concentrations (DV) vs. individual predicted concentrations (IPRED); the solid line represents the reference line. C. Conditional weighted residuals (CWRES) vs. predicted concentrations (PRED); the solid and dotted horizontal lines represent the reference line and ± 2 standard deviations, respectively. The red curve is a loess curve fit to the absolute values of the residuals. The bottom red curve is the reflection of the top red curve about the x-axis. The blue line is the loess curve fit to the raw residuals. D. Conditional weighted residuals (CWRES) vs. time after the first dose (TIME); the solid and dotted lines represent the reference line and ± 2 standard deviations, respectively. The red curve is a loess curve fit to the absolute values of the residuals. The bottom red curve is the reflection of the top red curve about the x-axis. The blue line is the loess curve fit to the raw residuals
The success rate of the bootstrap method was 100%, and the mean bootstrap parameters were close to the estimated values that were obtained from the original dataset (Table 3).
Simulation
The Monte Carlo simulations are summarized in Table 4 and Fig. 2. A daily maintenance dose of 0.25 mg could reach the intoxication risk window of a trough serum concentration of ≥1.2 ng/mL in nearly half of patients and ≥0.9 ng/mL in more than half of patients, regardless of renal function category or concurrent use of amiodarone. A daily maintenance dose of 0.125 mg could not be tolerated in patients with renal impairments (CLCR 30 mL/min) or concurrent use of amiodarone because more than half of patients reached a trough serum concentration of ≥0.9 ng/mL. A daily maintenance dose of 0.0625 mg was appropriate as a maintenance dose for patients with renal impairments or concurrent use of amiodarone.

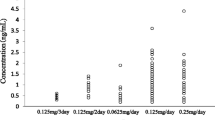
Summary of the Monte Carlo simulation. A. Violin plots for the predicted trough serum concentration according to the digoxin dosage and creatinine clearance in the absence of amiodarone. B. Violin plots for the predicted trough serum concentration according to the digoxin dosage and creatinine clearance in the presence of amiodarone. The dashed and dotted lines represent the median and interquartile range, respectively. The violin plots indicate the distributions of the predicted digoxin trough serum concentration according to the dosage
Discussion
We developed a population pharmacokinetic model of digoxin in Japanese patients with AF and HF using real-world data. This population pharmacokinetic analysis identified that CLCR and concurrent use of amiodarone influenced digoxin clearance and the appropriate maintenance dosage was 0.125 mg daily for almost all Japanese patients with AF and HF. However, 0.0625 mg daily appeared to be a suitable dosage for patients with renal impairments (CLCR 30 mL/min) or concurrent use of amiodarone.
Digoxin has a large Vd and ethnic differences in Vd that are corrected by kilograms of body weight have not been reported. We used the previously reported value of digoxin Vd [24] in this model because it does not influence the trough serum concentration at the steady state. Digoxin is excreted primarily by the kidney (≥70%), and renal excretion of digoxin is correlated with the glomerular filtration rate [6]. Previous studies have shown that CLCR is associated with the clearance of digoxin [26,27,28]. Because the Cockcroft-Gault formula is based on serum creatinine, body weight, age, and sex [22], these factors also influence the clearance of digoxin [29]. In this study, CLCR was established as the most useful covariate for the clearance of digoxin among several covariates. CLCR is not adjusted for body surface area and may more comprehensively reflect the individual situation.
Our results also showed that the use of amiodarone was a significant covariate of the clearance of digoxin. Digoxin is a substrate of P-glycoprotein, which contributes to its absorption and elimination [17]. Several medications are known to interact with digoxin via P-glycoprotein and affect the pharmacokinetics of digoxin [30]. In particular, amiodarone has a relatively high inhibition capacity against P-glycoprotein [30]. It has been reported that high-dose amiodarone administration (600 to 1600 mg daily) doubles digoxin plasma concentrations [31]. In this study, the effect of dose-dependent inhibition of amiodarone on digoxin pharmacokinetics was not clarified.
Our Monte Carlo simulation results indicated that 0.25 mg daily of digoxin was an unacceptable dosage because an estimated serum concentration of ≥1.2 ng/mL was predicted to occur in more than half of patients with AF and HF. Miura et al. reported that digoxin intoxication was observed even in Japanese patients with AF and/or HF whose serum concentrations were between 1.4 and 2.0 ng/mL [32]. We previously demonstrated that a serum concentration of ≥1.2 ng/mL was significantly associated with an increased risk of digoxin intoxication in patients with AF and HF [10]. The present analysis showed that 0.125 mg daily of digoxin is a favourable maintenance dosing regimen for a large proportion of Japanese patients with AF and HF. In patients with CLCR <30 mL/min or concurrent use of amiodarone, however, 0.125 mg daily is an undesirable dosing regimen. Dosage reduction to 0.0625 mg daily is recommended for these patients to avoid a poor prognosis and digoxin intoxication. Komatsu et al. suggested that an extremely low dosage of digoxin, namely, 0.0625 mg daily, was also suitable for Japanese patients with CLCR <35 mL/min or concurrent use of amiodarone but that 0.1875–0.25 mg daily was recommended for patients with CLCR >60 mL/min when the target serum digoxin concentration range was 0.5–0.8 ng/mL [33]. This discrepancy might be due to differences in the clinical characteristics of patients. The presence of HF is reported to influence the clearance of digoxin [29]. Renal clearance of digoxin decreases in patients with HF compared to patients without HF despite no difference in digoxin dosage, creatinine clearance, diuresis, or sodium excretion in the urine [34]. Therefore, the blood concentration of digoxin is higher in patients with HF than in patients without HF. Approximately half of Japanese patients with HF have renal impairment, and 10% receive amiodarone for complicated arrhythmias [35].
In patients with HF, renal clearance of a drug decreases because low cardiac output reduces renal blood flow and the glomerular filtration rate, in addition to causing renal parenchyma and renal tubule disorders (renal failure). Therefore, the clearance of digoxin is reduced, and the blood concentration is increased [34]. This study recommends dosages for patients with HF and also takes into account the effects of amiodarone, which is frequently used in patients with arrhythmias and HF, based on clinical data from patients with AF and HF and a reference target serum digoxin concentration range for patients with HF. In clinical practice, some patients required higher blood digoxin concentrations to maintain haemodynamics and adequate heart rate control. However, gastrointestinal complications increased with increased serum digoxin concentration among our patients. It is important to start with the recommended maintenance dosage and to adjust the dosage based on a thorough examination of the individual’s symptoms, effects, and side effects. We believe that our results will help ensure the safety of digoxin treatment for Japanese patients with AF and HF.
Study limitations
This study has several limitations that should be considered in the interpretation of the results. First, because this study had a single-centre retrospective observational design, we could not avoid the possibility of bias. Due to the sample size, this study was limited to assessing the impact in a special population (e.g., individuals with obesity and undergoing renal replacement therapy). Adherence to pharmacotherapy could not be evaluated. Second, the method of measuring the samples that were analysed in this study changed in December 2016. Because the accuracies of the measurements did not differ significantly between the methods before and after the change and no clinical problems occurred due to change in the measurement method, the measurement values were used in this study regardless of their measurement method. Third, this study did not fully investigate all drugs that may pharmacokinetically interact with digoxin. Due to the small sample size of this study, we limited the considered drugs to P-glycoprotein inhibitors, such as amiodarone, verapamil and diltiazem, that are expected to be used in combination in patients with AF and HF. Fourth, this study included only patients who were treated at a single centre. There was also treatment bias. The clinical characteristics of our patients might not reflect those of general HF patients because our institution is a university hospital in the metropolitan Tokyo area. Therefore, the findings could not be generalized to all Japanese patients with HF. It is unclear whether the use of the recommended dosages would improve outcomes including, e.g., in term of digitalis intoxication and death, in general Japanese patients with AF and HF. To evaluate this, validation in another patient population from this study will be required.
Conclusions
Our constructed population pharmacokinetic model indicates the clinical significance of CLCR and the use of amiodaron for digoxin oral clearance. A low maintenance dosage of digoxin, namely, 0.125 mg daily, is appropriate for Japanese patients with AF and HF, and the dosage should be reduced to 0.0625 mg daily for patients with CLCR <30 mL/min or concurrent use of amiodarone.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AF:
-
Atrial fibrillation
- CLCR :
-
Creatinine clearance
- CL/F:
-
Oral clearance
- eGFR:
-
Estimated glomerular filtration rate
- HF:
-
Heart failure
- Vd:
-
Apparent volume of distribution
References
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200. https://doi.org/10.1093/eurheartj/ehw128.
Tsutsui H, Isobe M, Ito H, Ito H, Okumura K, Ono M, et al. JCS 2017/JHFS 2017 guideline on diagnosis and treatment of acute and chronic heart failure - digest version. Circ J. 2019;83(10):2084–184. https://doi.org/10.1253/circj.CJ-19-0342.
Gheorghiade M, Adams KF Jr, Colucci WS. Digoxin in the management of cardiovascular disorders. Circulation. 2019;109(24):2959–64. https://doi.org/10.1161/01.CIR.0000132482.95686.87.
Turakhia MP, Santangeli P, Winkelmayer WC, Xu X, Ullal AJ, Than CT, et al. Increased mortality associated with digoxin in contemporary patients with atrial fibrillation: findings from the TREAT-AF study. J Am Coll Cardiol. 2014;64(7):660–8. https://doi.org/10.1016/j.jacc.2014.03.060.
Ouyang AJ, Lv YN, Zhong HL, Wen JH, Wei XH, Peng HW, et al. Meta-analysis of digoxin use and risk of mortality in patients with atrial fibrillation. Am J Cardiol. 2015;115(7):901–6. https://doi.org/10.1016/j.amjcard.2015.01.013.
Hauptman PJ, Kelly RA. Digitalis. Circulation. 1999;99(9):1265–70. https://doi.org/10.1161/01.cir.99.9.1265.
Eichhorn EJ, Gheorghiade M. Digoxin. Prog Cardiovasc Dis. 2002;44(4):251–66. https://doi.org/10.1053/pcad.2002.31591.
Beller GA, Smith TW, Abelmann WH, Haber E, Hood WB Jr. Digitalis intoxication: a prospective clinical study with serum level correlations. N Engl J Med. 1971;284(18):989–97. https://doi.org/10.1056/NEJM197105062841801.
Ordog GJ, Benaron S, Bhasin V, Wasserberger J, Balasubramanium S. Serum digoxin levels and mortality in 5,100 patients. Ann Emerg Med. 1987;16(1):32–9. https://doi.org/10.1016/s0196-0644(87)80281-0.
Hirai T, Naganuma M, Shiga T, Echizen H, Itoh T, Hagiwara N. Serum digoxin concentrations and outcomes in patients with heart failure and atrial fibrillation: a single-center observational study. Jpn J Clin Pharmacol Ther. 2020;51(2):57–64. https://doi.org/10.3999/jscpt.51.57.
Duhme DW, Greenblatt GJ, Koch-Weser J. Reduction of digoxin toxicity associated with measurements of serum levels: a report from the Boston collaborative drug surveillance program. Ann Intern Med. 1974;80(4):516–9. https://doi.org/10.7326/0003-4819-80-4-516.
Aronson JK, Hardmann M. ABC of monitoring drug therapy. Digoxin BMJ. 1992;305(6862):1149–52. https://doi.org/10.1136/bmj.305.6862.1149.
Rathore SS, Curtis JP, Wang Y, Bristow MR, Krumholz HM. Association of serum digoxin concentration and outcomes in patients with heart failure. JAMA. 2003;289(7):871–8. https://doi.org/10.1001/jama.289.7.871.
Lopes RD, Rordorf R, De Ferrari GM, Leonardi S, Thomas L, Wojdyla DM, et al. Digoxin and mortality in patients with atrial fibrillation. J Am Coll Cardiol. 2018;71(10):1063–74. https://doi.org/10.1016/j.jacc.2017.12.060.
Aonuma K, Shiga T, Atarashi H, Doki K, Echizen H, Hagiwara N, et al. Guidelines for therapeutic drug monitoring of cardiovascular drugs clinical use of blood drug concentration monitoring (JCS 2015) - digest version. Circ J. 2017;81(4):581–612. https://doi.org/10.1253/circj.CJ-66-0138.
Iisalo E. Clinical pharmacokinetics of digoxin. Clin Pharmacokinet. 1977;2(1):1–16. https://doi.org/10.2165/00003088-197702010-00001.
Wessler JD, Grip LT, Mendell J, Giugliano RP. The P-glycoprotein transport system and cardiovascular drugs. J Am Coll Cardiol. 2013;61(25):2495–502. https://doi.org/10.1016/j.jacc.2013.02.058.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982–92. https://doi.org/10.1053/j.ajkd.2008.12.034.
Sheiner LB, Rosenberg B, Melmon KL. Modelling of individual pharmacokinetics for computer-aided drug dosage. Comput Biomed Res. 1972;5(5):411–59. https://doi.org/10.1016/0010-4809(72)90051-1.
Sheiner LB, Beal SL. Evaluation of methods for estimating population pharmacokinetics parameters. I. Michaelis-Menten model: routine clinical pharmacokinetic data. J Pharmacokinet Biopharm. 1980;8(6):553–71. https://doi.org/10.1007/BF01060053.
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation. 2013;128(16):e240–327. https://doi.org/10.1161/CIR.0b013e31829e8776.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. https://doi.org/10.1159/000180580.
Gerloff T, Schaefer M, Johne A, Oselin K, Meisel C, Cascorbi I, et al. MDR1 genotypes do not influence the absorption of a single oral dose of 1 mg digoxin in healthy white males. Br J Clin Pharmacol. 2002;54(6):610–6. https://doi.org/10.1046/j.1365-2125.2002.01691.x.
Aronson JK. Clinical pharmacokinetics of digoxin 1980. Clin Pharmacokinet. 1980;5(2):137–49. https://doi.org/10.2165/00003088-198005020-00002.
Adams KF Jr, Gheorghiade M, Uretsky BF, Patterson JH, Schwartz TA, Young JB. Clinical benefits of low serum digoxin concentrations in heart failure. J Am Coll Cardiol. 2002;39(6):946–53. https://doi.org/10.1016/s0735-1097(02)01708-4.
Jelliffe RW, Brooker G. A nomogram for digoxin therapy. Am J Med. 1974;57(1):63–8. https://doi.org/10.1016/0002-9343(74)90769-4.
Konishi H, Shimizu S, Chiba M, Minouchi T, Koida M, Yamaji A. Predictive performance of serum digoxin concentration in patients with congestive heart failure by a hyperbolic model based on creatinine clearance. J Clin Pharm Ther. 2002;27(4):257–65. https://doi.org/10.1046/j.1365-2710.2002.00418.x.
Zhao L, Yang P, Li P, Wang X, Qin W, Zhang X. Efficiency of individual dosage of digoxin with calculated concentration. Clin Interv Aging. 2014;9:1205–10. https://doi.org/10.2147/CIA.S63596.
Yukawa M, Yukawa E, Suematsu F, Takiguchi T, Ikeda H, Aki H, et al. Determination of digoxin clearance in Japanese elderly patients for optimization of drug therapy: a population pharmacokinetics analysis using nonlinear mixed-effects modelling. Drugs Aging. 2011;28(10):831–41. https://doi.org/10.2165/11594230-000000000-00000.
Fenner KS, Troutman MD, Kempshall S, Cook JA, Ware JA, Smith DA, et al. Drug-drug interactions mediated through P-glycoprotein: clinical relevance and in vitro-in vivo correlation using digoxin as a probe drug. Clin Pharmacol Ther. 2009;85(2):173–81. https://doi.org/10.1038/clpt.2008.195.
Robinson K, Johnston A, Walker S, Mulrow JP, McKenna WJ, Holt DW. The digoxin-amiodarone interaction. Cardiovasc Drugs Ther. 1989;3(1):25–8. https://doi.org/10.1007/BF01881526.
Miura T, Kojima R, Sugiura Y, Mizutani M, Takatsu F, Suzuki Y. Effect of aging on the incidence of digoxin toxicity. Ann Pharmacother. 2000;34:427–32. https://doi.org/10.1345/aph.19103.
Komatsu T, Morita M, Miyaji F, Inomata T, Ako J, Atsuda K. Population pharmacokinetics and optimization of the dosing regimen of digoxin in adult patients. J Pharm Health Care Sci. 2015;1:25. https://doi.org/10.1186/s40780-015-0023-6.
Naafs MA, van der Hoek C, van Duin S, Koorevaar G, Schopman W, Silberbusch J. Decreased renal clearance of digoxin in chronic congestive heart failure. Eur J Clin Pharmacol. 1985;28(3):249–52. https://doi.org/10.1007/BF00543318.
Shiga T, Suzuki A, Haruta S, Mori F, Ota Y, Yagi M, et al. Clinical characteristics of hospitalized heart failure patients with preserved, mid-range, and reduced ejection fractions in Japan. ESC Heart Fail. 2019;6(3):475–86. https://doi.org/10.1002/ehf2.12418.
Acknowledgements
We thank Ms. Emi Sawada for her assistance.
Funding
This research received no grants from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
T.H. and T.S. conceived and designed the study. T.H., M.N. and T.S. collected and organized the patient data from the patient files. T.H. and H.K. analysed the data. T.H. and T.S. contributed to the interpretation of the data. T.H. and T.S. were major contributors to the writing of the manuscript. N.H. supervised the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was approved by the Institutional Review Boards of Tokyo Women’s Medical University (2020–0117) and Jikei University (32–209 (102909)), and the requirement to obtain written and verbal informed consent was waived due to the nature of the retrospective study. The study received ethical approval for the use of an opt-out approach to consent. The Institutional Review Boards of both sites permitted a transfer of study data from Tokyo Women’s Medical University to Jikei University for collaborative research. This study was conducted in compliance with Ethical Guidelines for Medical and Biological Research Involving Human Subjects issued by the Japanese Ministry of Health, Labour and Welfare and the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors have no potential conflicts of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Fig.
Relationships between the random effect for CL (eta CL) and the potential covariates (sex, age, height and body mass index) in the final model.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hirai, T., Kasai, H., Naganuma, M. et al. Population pharmacokinetic analysis and dosage recommendations for digoxin in Japanese patients with atrial fibrillation and heart failure using real-world data. BMC Pharmacol Toxicol 23, 14 (2022). https://doi.org/10.1186/s40360-022-00552-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40360-022-00552-y