
Abstract
Respiratory diseases constitute a major health problem for ruminants, resulting in considerable economic losses throughout the world. Parainfluenza type 3 virus (PIV3) is one of the most important respiratory pathogens of ruminants. The pathogenicity and phylogenetic analyses of PIV3 virus have been reported in sheep and goats. However, there are no recent studies of the vaccination of sheep or goats against PIV3. Here, we developed a purified inactivated ovine parainfluenza virus type 3 (OPIV3) vaccine candidate. In addition, we immunized sheep with the inactivated OPIV3 vaccine and evaluated the immune response and pathological outcomes associated with OPIV3 TX01 infection. The vaccinated sheep demonstrated no obvious symptoms of respiratory tract infection, and there were no gross lesions or pathological changes in the lungs. The average body weight gain significantly differed between the vaccinated group and the control group (P < 0.01). The serum neutralization antibody levels rapidly increased in sheep post-vaccination and post-challenge with OPIV3. Furthermore, viral shedding in nasal swabs and viral loads in the lungs were reduced. The results of this study suggest that vaccination with this candidate vaccine induces the production of neutralizing antibodies and provides significant protection against OPIV3 infection. These results may be helpful for further studies on prevention and control strategies for OPIV3 infections.
Similar content being viewed by others

Introduction
Parainfluenza virus type 3 (PIV3) is one of the most important viral respiratory pathogens for humans and many species of animals [1]. The virus belongs to the family Paramyxoviridae, subfamily Orthoparamyxovirinae, genus Respirovirus, which includes human parainfluenza virus type 3 (HPIV3), bovine parainfluenza virus type 3 (BPIV3), caprine parainfluenza virus type 3 (CPIV3), human parainfluenza virus type 1 (HPIV1), murine parainfluenza virus 1 (MPIV1) and other newly discovered strains. The members of this virus family are enveloped and have genomes consisting of a single segment of negative-sense RNA, which usually has a length of 15 kb [2, 3]. PIV3 infections are found in a wide variety of mammals, including humans, cattle, sheep, goats, rhinoceros, pigs, dogs, dolphins, bison, guinea pigs, moose, bighorn sheep, camels, and water buffaloes [1, 4,5,6,7].
PIV3 infection usually results in respiratory symptoms and increases morbidity and mortality rates under a variety of stress conditions or during coinfection with other bacterial pathogens [7,8,9]. Immunization is the most effective method for preventing infectious diseases. Therefore, the rapid development of effective vaccines against PIV3 is urgently needed.
HPIV3 is one of the most common viral pathogens that causes acute lower respiratory infection (ALRI) in children, particularly in infants. Currently, no vaccine exists for the virus [10]. Over the last decade, several HPIV3 live-attenuated vaccines, such as rHPIV3cp45, rB/HPIV3, and MEDI-534, have been tested in clinical trials [11]. In addition, several vaccines are being developed to prevent HPIV3 infection, including those containing viral epitopes, DNA- and RNA-based formulations, adenovirus-based vectors, and inactivated whole viruses [12,13,14,15].
BPIV3 infection causes severe bronchopneumonia and secondary bacterial infections in instances of high stress, such as during transportation, weather change and feedlot conditions [16]. The main clinical signs of BPIV3 infection are coughing, anorexia, pyrexia, nasal and ocular discharge, dyspnoea and sometimes diarrhoea [18], followed by modified live virus (MLV) vaccines [19]. BPIV3 is closely related to bovine respiratory syncytial virus (BRSV), bovine infectious rhinotracheitis virus (IBR), bovine viral abdomen diarrhoea-mucocoosis virus (BVDV), and bovine adenovirus (BADV), and mixed infections with these viruses can occur, exacerbating their effect on the immune system [20,21,22]. Thus, several studies have been performed to investigate the possibility of combining BRSV-BPIV3 vaccines with other vaccines, for example, the combination of a live BRSV-BPIV3 vaccine with an M. haemolytica vaccine or the combination of an inactivated BRSV-BPIV3-M. haemolytica vaccine with a live bovine herpesvirus vaccine [23, 24]. In particular, BPIV3 is a promising vaccine vector for the treatment of infections caused by various respiratory viruses, including HPIV3, respiratory syncytial virus (RSV), and severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) [25].
Currently, there are only two complete gene sequences of sheep-sourced parainfluenza viruses in the GenBank database, namely, TX01 (GenBank No. MT756864) and TJ2022 (GenBank No. OR472985.1), while the others are goat-sourced parainfluenza viruses. Compared to HPIV3 and BPIV3, there are fewer sheep-sourced parainfluenza virus strains, and unlike BPIV3, they have not been typed. Although the isolation of parainfluenza virus type 3 from sheep was reported in 1966 [26], epidemiological surveys have shown that PIV3 remains widely prevalent in sheep and goat flocks [7, 27, 28]. Similar to BPIV3, PIV3 infection usually results in respiratory symptoms in goats and sheep. The noted clinical signs include coughing, nasal discharge, dyspnoea and anorexia. Gross and histopathological lesions are mainly found in the lungs and trachea [29, 30]. However, there are no commercial PIV3 vaccines available for sheep and goats or prevention and control measures available. In this study, an OPIV3 challenge model was established in lambs. An inactivated ISA 206 adjuvant OPIV3 vaccine candidate was also developed. Then, the immunogenicity and protective efficacy of the PIV3 vaccine were evaluated in sheep challenged with OPIV3.
Two-month-old sheep subjected to PIV3 inactivation showed a significantly lower temperature response, gross pathology and PIV3 replication in the lungs than did the control group. These results indicate that sheep immunization with an inactivated vaccine candidate for OPIV3 confers protection against PIV3, supporting this strategy for respiratory diseases.
Materials and methods
Cell lines and virus culture
The viral stock was propagated in Madin–Darby bovine kidney (MDBK) cells cultured with Dulbecco’s modified Eagle’s medium (DMEM) (GIBCO, USA) supplemented with 1% penicillin/streptomycin and 2% foetal bovine serum (FBS) and incubated at 37 °C in a 5% CO2 incubator. When the cytopathic effect (CPE) exceeded 80%, the cell culture supernatant was collected, purified by low-speed centrifugation (300 × g for 10 min), and stored at −80 °C.
Viral titration
Viral titration was determined by a 50% cell culture infectious dose (TCID50) endpoint dilution assay. Briefly, MDBK cells were inoculated in a 96-well culture plate and cultured until they reached 70–80% confluence. Then, the supernatant was removed, and the cells were washed twice with phosphate-buffered saline (PBS). Serial tenfold dilutions of the viruses were added to the samples, which were subsequently plated in a 96-well culture plate. After 5 days of culture at 37 °C, the cells were checked under a microscope for the presence of CPE.
TEM observation
The virus was stained with 2% phosphotungstate acid for 1–2 min at room temperature and examined via transmission electron microscopy (TEM, JEM-1400 FLASH, Japan Electronics).
Preparation of the inactivated OPIV3 vaccine
The OPIV3 viruses cultured for the inactivated vaccine were generated based on previous methods.
To prepare the virus-inactivated solution, 0.2 mol/L BEA was mixed with 0.4 mol/L NaOH at a volume ratio of 2:1 in the appropriate container at 37 °C for at least 1 h to generate the BEI solution, after which the BEI solution was filtered through a 0.22 μm membrane (Millipore). To hydrolyse residual BEI, 2% sodium thiosulfate was added to the filtered BEI solution at a final concentration of 0.03 mol/L in a warm bath at 37 °C for 1 h with gentle stirring for 10 min. The conditions for OPIV3 viral inactivation were determined with a set volume and concentration of the BEI solution in this study. To validate effective virus inactivation, 0.1 mL of inactivated virus was inoculated from each of the virus/BEI mixtures into MDBK cell culture flasks at 37 °C for 5 days. Then, the flasks were freeze-thawed three times, and 0.1 mL of purified supernatant was transferred to another MDBK cell monolayer in a 25 cm2 flask, which was incubated at 37 °C for another 5 days. The passage process was repeated three times. No CPE was observed after three passages, while positive controls showed 100% CPE.
For the OPIV3 vaccine formulation, the ISA 206 adjuvant (SEPPIC, France) was used. The ISA 206 adjuvant was autoclaved at 121 °C for at least 40 min. Before emulsification, the liquid temperature was controlled within the range of 28–32 °C. The inactivated antigen was mixed with the ISA 206 adjuvant at a ratio of 50% by weight. For a stable W/O/W vaccine emulsion, a one-step process was performed using a low shear rate and controlled temperature at 31 °C (± 1 °C) for 25 min until the antigen was fully mixed with the adjuvant. The duplex oil emulsion was kept at 4 °C until use.
Sheep immunization, infection, and sample collection
Fifteen 2-month-old sheep (Du Han hybrid sheep) were obtained from a farm in Inner Mongolia, China. All animals were negative for OPIV3, Mycoplasma ovipneumoniae (MO), Mannheimia haemolytica (M.H.), and brucellosis and presented no signs of depression, cough or other health disorders. The animals were randomly divided into three groups of five sheep each, including a vaccinated group, a control group and a nonchallenged group.
The vaccinated group was administered 2 mL of inactivated vaccine per sheep via intramuscular (IM) injection. After 21 days of vaccination, the sheep were boosted via the same dose and delivery route as above. After 42 days, the vaccinated group and control group were challenged with 4 mL of OPIV3 at 1 × 107.5 TCID50/mL via tracheal injection. The sheep in the nonchallenged group remained unvaccinated and unchallenged and served as the negative control group. The rectal temperature and body weights were monitored in the animal experiment. Blood samples were collected from the sheep before immunization and every 7 days after vaccination and booster immunization. The blood was centrifuged, and the serum was collected and stored at −20 °C for antibody detection. Clinical signs, including depression, cough, asthma, and other respiratory symptoms, were recorded from Day 0 to Day 14, and “+” indicates that one of the above clinical symptoms occurred. In addition, the number of “+” represents the severity,+mild;+ +, moderate;+++ , severe. The data were scored on a scale of 0–3 (0 = absent; 1 = mild; 2 = moderate; 3 = severe). On the 14th day after infection, all experimental animals were humanely euthanized. Nasal swab specimens and lungs were collected. All of the respective animal protocols were reviewed and approved by the Institutional Animal Ethics Committee of Inner Mongolia University (Approval No. IMU-2021-sheep-044).
Gross pathology and histopathology
On Day 14, gross dissection was performed. The gross lesions in the lungs, tracheas, lymph nodes and other tissues of the sheep were observed and examined via necropsy. The extent of gross lesions was evaluated and is expressed as normal, mild, moderate or severe. Liver, spleen, lung, heart, kidney, intestine, and mesenteric lymph node tissue samples were collected and fixed in buffer with 10% formalin for histopathological analysis.
Immunohistochemistry (IHC)
Formalin-fixed lungs were subjected to immunohistochemistry (IHC) to evaluate the OPIV3 load. The sections were incubated with 500-fold dilutions of monoclonal antibodies against the N protein of OPIV3 (developed in our laboratory) at 4 °C overnight, followed by incubation with 100-fold diluted goat anti-mouse IgG-HRP (Abcam 205719) at 37 °C for 50 min. Then, freshly prepared DAB (Servicebio G1211, Wuhan, China) was added to the sections for colour development at room temperature for approximately 10 min. Finally, the sections were stained with Mayer’s haematoxylin (Servicebio G1004, Wuhan, China) for 1 min, dehydrated and mounted with neutral gum. The percentage of immunostaining and the staining intensity (0, negative; 1+ , weak; 2+ , moderate; and 3+ , strong) were recorded (ImageScope, Leica). The H-score was calculated using the following formula:
H-SCORE = ∑(PI × I) = (percentage of cells with weak intensity × 1) + (percentage of cells with moderate intensity × 2) + percentage of cells with strong intensity × 3).
Real-time quantitative RT-PCR (qRT-PCR)
Total RNA was extracted from 100 mg of lung homogenate with TRIzol reagent (Takara, China) according to the manufacturer’s instructions. cDNA was synthesized using a Takara 6210A PrimeScript™II 1st Strand cDNA Synthesis Kit. qPCR was performed using TB Green Premix Ex Taq II (Takara, China) according to the manufacturer’s instructions. OPIV3-specific primers (forward primer 5′-AGGTAGGCAATCCACCAAAGC-3′, reverse primer 5′-CCCGATTGGTAAAGAACCTGAT-3′) were used for amplification. The samples were heated to 95 °C for 30 s, followed by 45 cycles of 10 s at 95 °C and 30 s at 60 °C. The negative and positive controls contained ddH2O, and the standard plasmid was included in the experiments. The viral genome copy number was calculated according to the results from the tenfold serial dilutions of the positive plasmid. All of the reactions were performed in triplicate.
Virus neutralization assay
Serum samples collected from immunized animals were inactivated at 56 °C for 0.5 h and serially diluted with cell culture medium in two steps. The diluted sera were mixed with a virus suspension of 100 TCID50 in 96-well plates at a ratio of 1:1, followed by 2 h of incubation at 37 °C in a 5% CO2 incubator. The serum-virus mixture was subsequently added to a 96-well culture plate supplemented with 1 × 104 MDBK cells, after which the plates were incubated for 5 days at 37 °C in a 5% CO2 incubator. The CPE of each well was recorded under a microscope, and the neutralizing titre was calculated by diluting the sample to 50%.
Statistical analysis
Statistical analyses were performed using Graph Pad Prism 6.02 software.
Results
Characterization of the OPIV3 vaccine candidate
To obtain a viral stock that efficiently replicates in MDBK cells for OPIV3 vaccine production, the OPIV3 TX01 strain was passaged in MDBK cells to generate the P21 stock virus. MDBK cells infected with the OPIV3 TX01 strain exhibited CPE at 72 h post-infection (Figure 1A). Transmission electron microscopy was used to observe OPIV3. The micrograph of OPIV3 showed intact, oval-shaped particles with diameters of 150 to 250 nm (blue arrow). A long fragment of free nucleocapsid chains originated from the disintegration of the viral particles in the supernatant of a CPE-positive MDBK cell culture infected with the OPIV3 TX01 strain (red arrow) (Figure 1B). The OPIV3 TX01 strain replicated efficiently and reached a peak titre at 107.5 TCID50/mL after 72 h at an MOI of 1.0 (Figure 1C).

Characterization of the OPIV3 vaccine candidate. A Confirmation of OPIV3 infection in MDBK cells. OPIV3-induced CPE was observed, and the cell monolayer was completely destroyed after OPIV3 infection (scale bar = 50 nm). B TEM image of OPIV3 (scale bar = 100 nm). A micrograph of OPIV3 showed intact, oval-shaped particles with diameters ranging from 150 to 250 nm (shown by the blue arrow). A long fragment of free nucleocapsid chains originated from the disintegration of viral particles in the supernatant of a CPE-positive MDBK cell culture infected with the OPIV3 TX01 strain (shown by the red arrow). C Growth kinetics of MDBK cells infected with OPIV3 at 0.01, 0.1 and 1.0 MOI.
OPIV3 vaccine preparation
The OPIV3 virus was cultured in 175 cm2 flasks and inactivated with 0.004 mol/L BEI for 40 h at 37 °C under gentle rocking for viral inactivation. The inactivated virus/BEI solution was neutralized by the addition of 2% sodium thiosulfate. The purified viruses were formulated with ISA 206 adjuvant as the OPIV3 vaccine. The working flowchart of OPIV3 vaccine preparation is shown in Figure 2.

Flowchart of OPIV3 vaccine preparation.
Vaccination protects sheep against challenge with the OPIV3 TX01 F6 strain
A flowchart of the vaccine immunogenicity analysis is shown in Figure 3. After vaccination with the inactivated OPIV3 vaccine candidate, all of the animals except one showed an increase in body temperature of approximately 40.0 °C for a single day from 0 to 5 days post-vaccination. Adverse effects were not observed in any of the vaccinated animals.

Animal experimental design. Sheep were intramuscularly immunized with inactivated OPIV3 TX01 at Days 0 and 21 and challenged with 4 mL of OPIV3 (107.5 TCID50/mL) after Day 42.
Following a challenge with the OPIV3 TX01 F6 strain (4 mL/sheep at 1 × 107.5 TCID50/mL), the total daily clinical symptoms were recorded, and the results showed that symptoms appeared 2–14 days after exposure to the virus in the control group. These symptoms were relatively obvious and could last for several days (Table 1). The sheep in the control group developed clinical signs of depression, cough, asthma, nasal discharge and anorexia post-challenge. It should also be noted that there were individual differences in clinical symptoms. These results are consistent with previous reports [30]. The vaccinated sheep were protected with fewer clinical signs than were the unvaccinated controls. After challenge, the body temperature of all sheep vaccinated with the inactivated OPIV3 vaccine prototype remained within the normal range until the end of the study. In contrast, the animals in the control group showed an increase in body temperature, reaching values higher than 40.0 °C for at least 1 day. During the 0 to 14 days of viral infection, 4 sheep had body temperatures greater than 40.2 °C twice (Figure 4A).

Clinical scores and average weight gain of the sheep. A Rectal temperature was monitored daily for 14 days after infection. B Clinical scores of vaccinated and control sheep post-challenge. C Comparison of the average weight gain of sheep. The average body weight gain significantly differed between the vaccinated group and the control group (P < 0.01).
The clinical signs typical of PIV3 infection were examined, and the overall clinical reaction score was calculated. However, none of the four vaccinated animals experienced cough, asthma, or nasal discharge after the challenge. One of the sheep appeared depressed at 2 days post-challenge (dpc). A graphical representation of the daily clinical score for each group is shown in Figure 4B. In addition, the average body weight gain was significantly different between the vaccinated and control groups (P < 0.01) (Figure 4C).
The sheep in the control group exhibited mild to moderate diffuse purple consolidation in the pulmonary lobules and interstitial lung disease. The lesions were mainly concentrated in the right upper lobe. The sheep lungs in the vaccinated group exhibited normal gross pathology (Figure 5). No pathological changes in the heart, liver, spleen or kidney were observed in the other groups (data not shown).

Gross pathological lesions in sheep lungs. Multifocal red areas (red arrows) were observed in the lungs of unvaccinated sheep but not in the lungs of vaccinated sheep or those of the nonchallenged group. The lesions were mainly concentrated in the right lung lobule. Lung consolidation was mild to moderate.
Histopathological analysis revealed that the alveolar walls were obviously thickened, the blood vessels were dilated and congested, and there was fibrous histiocytosis and severe immune cell infiltration. No lesions were observed in the control group (Figure 6A). There were no obvious histological abnormalities in other organs or tissues (data not shown).

Histopathological examinations, viral loading and viral shedding. A Histopathological examination of sheep lungs at 14 dpc. The lungs of the sheep in the vaccinated group were necropsied at 14 dpc (magnification, × 200). Lung sections from control sheep showed severely thickened alveolar septa, expansions of the alveolar interstitium, congestion, macrophage infiltration, and compensatory emphysema. The results revealed the appearance of viral pneumonia with interstitial lymphocytic infiltrates (magnification, × 200). B Formalin-fixed lung sections were subjected to OPIV3 load evaluation by IHC. C The viral load was evaluated by RT-qPCR. D Viral shedding was evaluated by RT-qPCR.
N protein expression in the lungs of OPIV3-infected animals was determined by immunohistochemistry in association with viral load and clinicopathological features. The mean N protein level in the control and vaccinated groups was greater than that in the nonchallenged group (15.278, 6.102 vs. 0.124; P < 0.001). The data are shown as one-way ANOVA data for the vaccinated group vs. the nonchallenged group (6.102 vs. 0.124, P < 0.001) and for the control group vs. the vaccinated group (15.278 vs. 6.102, P < 0.001). Overall, the results showed different staining intensities for the OPIV3 N protein in each group because of differences in viral load. There was obviously lower expression of OPIV3-N in the lungs of the vaccinated group than in the lungs of the control group. (Figure 6B).
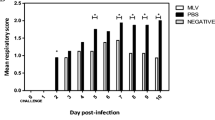
For further analysis of viral load and shedding, RT‒qPCR was used to evaluate the protection afforded by the OPIV3 vaccine candidates. The viral loads in the lungs of the vaccinated group were 860.6 ± 669.4 copies/µL (n = 5), whereas those in the control group were 2520 ± 2202 copies/µL (n = 5). The number of viral copies/µL in the lungs of the vaccinated group was lower than that in the lungs of the control group. The lungs of three of the sheep in the vaccinated group were negative for OPIV3 according to RT‒qPCR (CT ≥ 33). The peak viral loads were observed in the control group and vaccinated group, in which there were 11.327 × 103 copies/µL and 3.527 × 103 copies/µL, respectively. Individual differences are shown in Figure 6C. Moreover, the liver, heart, kidney and spleen of the challenge sheep were negative for OPIV3 (data not shown). The sheep were positive for OPIV3 nasal shedding post-challenge. The peak nasal shedding occurred on Day 4 post-challenge in the vaccinated group and on Day 6 post-challenge in the control group. Compared with those in the vaccine groups, the viral genome loads in the nasal swabs of the control group were greater on Days 1, 2, 6, 8, 12, and 14 (Figure 6D). The data are shown as the mean ± SEM.
Virus neutralization antibody response
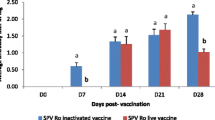
The induction of virus-neutralizing (VN) antibodies after vaccination can be a key protective immune response. Thus, we evaluated the levels of VN antibodies. In the vaccinated groups, VN antibodies were detected at 7 dpi. After 14 days of vaccination, the VN antibody titre in sheep was 1.777 ± 0.217 log10 (n = 5), whereas that in the control group was 0.364 ± 0.067 log10 (n = 5). The VN antibody titre continuously increased post-vaccination (dpv) and with a booster post-challenge in vaccinated sheep. After 21 days and 42 days of vaccination, the neutralizing antibody titres in sheep were 2.256 ± 0.295 log10 (n = 5) and 2.802 ± 0.165 log10 (n = 5), respectively. In contrast, the neutralizing antibody titres in the control group increased only after the challenge (Figure 7). The data are shown as the mean ± S.D.

Virus neutralization antibody response. Groups of sheep (n = 5) were vaccinated or not vaccinated at 0 and 21 days and challenged with OPIV3 at 45 dpv. Scatter plot showing the neutralizing antibody titres in the vaccinated group (blue circle) and control group (red triangle). The symbols represent individual animals, and the short lines represent the mean VN titres for each group. The data are shown as the mean ± S.D.
Discussion
Vaccination is among the most effective ways to prevent respiratory diseases caused by parainfluenza virus type 3 diseases [31, 32]. Compared to live vaccines, inactivated vaccines have attracted much attention due to their safer profile and easier transport and storage [33]. Inactivated viruses have been traditionally used for vaccine development, and such vaccines are safe and effective for the prevention of viral diseases such as coronavirus disease 2019 (COVID-19), influenza, foot and mouth disease, and polio [34,35,36].
In our previous research, the PIV3 strain was isolated from sheep suffering severe respiratory disease in China. We have previously described the phylogenetic analysis and pathogenicity of PIV3 in sheep [30]. By analysing the important parameters relevant to the evaluation of treatment efficacy (body temperature/clinical signs/gross pathological/viral shedding and viral loading/VN antibody titres), significant differences in clinical signs and weight changes were found between the vaccinated sheep and the controls after viral challenge. Compared with BPIV3 and HPIV3 vaccine studies, there are fewer PIV3 vaccine studies in sheep and goats, and these studies mainly date from the 1970s and 1980s [37,38,39,40]. Our results show that the OPIV3 vaccine tested in the current study induced higher levels of antibodies than those previously reported, and the percentage of gross lung lesions decreased significantly [37, 39]. These differences may be due to differences in the candidate vaccine strains and/or the different adjuvants used [42]. The complete gene sequences of the TX01 strain were uploaded to GenBank in 2021 [30]. ISA 206 (Seppic, France) adjuvanted vaccines stimulate protective immune responses in pigs, cattle, and sheep within a short period, with little or no toxicity or local reactivity [41]. ISA 206, the mineral-based oil described earlier, readily forms a water-in-oil-in-water emulsion [42].
Although the breeds and ages of the sheep used in the experiment differed from those used in the previous study, the vaccine strains and the immunization and challenge doses were also different, and the inactivated parainfluenza vaccine reduced the severity of respiratory diseases caused by parainfluenza, which is consistent with previous studies.
The main clinical signs produced by the PIV3 challenge in our studies are consistent with clinical symptoms observed in other PI3V challenge experiments [30, 43]. It is important to point out the reasons for the differences in daily weight gain of sheep may be due to season, environment, breed, and age. The OPIV3 TX01 wild-type strain was isolated from the lungs of both groups after gross dissection (data not shown). On the one hand, the pathogenic capacity of OPIV3 in the lungs was shown; on the other hand, the challenge dose of OPIV3 requires further study as the natural infection volume is likely to be lower than the challenge dose, and the infection mode also differs from the challenge mode. In addition, the breed of sheep and individual differences should be considered. Studies on vaccine immune dose, minimum dose, and treatment duration will be performed in the future to establish the protective antigen payload in the vaccine and provide insights into the evaluation of vaccine immunogenicity.
Previously, researchers have shown that vaccination against the viral component in virus-enhanced bacterial infections of the respiratory tract prevents a predisposition to bacterial superinfection [44].
The lambs vaccinated against PIV3 virus were successfully protected against the clinical illness associated with the virus and were also protected in part against the effects of bacterial superinfection. In addition, both inactivated vaccines and attenuated intranasal PIV3 vaccines can reduce the severity of pneumonia lesions and lamb mortality associated with secondary Pasteurella haemolytica infection [31, 38, 44]. Consequently, once PIV3 vaccination is widely used, the possibility of secondary bacterial infection will be reduced. Our future studies will include in-depth research on the prevention and control strategies of PIV3-induced respiratory diseases.
In conclusion, this study provides encouraging data regarding the safety and efficacy of the PIV3 vaccine for sheep and offers new ideas for the prevention and control of respiratory diseases.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request. All the data generated or analysed during this study are included in this published article.
References
Maidana SS, Lomonaco PM, Combessies G, Craig MI, Diodati J, Rodriguez D, Parreño V, Zabal O, Konrad JL, Crudelli G, Mauroy A, Thiry E, Romera SA (2012) Isolation and characterization of bovine parainfluenza virus type 3 from water buffaloes (Bubalus bubalis) in Argentina. BMC Vet Res 8:83
International Committee of Taxonomy of Viruses (2024) Current ICTV taxonomy release.
Walker PJ, Siddell SG, Lefkowitz EJ, Mushegian AR, Dempsey DM, Dutilh BE, Harrach B, Harrison RL, Hendrickson RC, Junglen S, Knowles NJ, Kropinski AM, Krupovic M, Kuhn JH, Nibert M, Rubino L, Sabanadzovic S, Simmonds P, Varsani A, Zerbini FM, Davison AJ (2019) changes to virus taxonomy and the international code of virus classification and nomenclature ratified by the international committee on taxonomy of viruses (2019). Arch Virol 164:2417–2429
Eisa M, Karrar A, Rahim AA (1979) The occurrence of antibodies to parainfluenza3 virus in sera of some domestic animals of the Sudan. Br Vet J 135:192–197
Ren JL, Zhu YM, Zhou YH, Lv C, Yan H, Ma L, Shi HF, Xue F (2015) Identification of three antigen epitopes on the nucleocapsid protein of the genotype C of bovine parainfluenza virus type 3. Vet Microbiol 178:61–69
Qiao D, Janke BH, Elankumaran S (2010) Complete genome sequence and pathogenicity of two swine parainfluenzavirus 3 isolates from pigs in the United States. J Virol 84:686–694
Mao L, Yang L, Li W, Liang P, Zhang S, Li J, Sun M, Zhang W, Wang L, Zhong C, Liu M, Jiang J, Cai X, Luo X (2019) Epidemiological investigation and phylogenetic analysis of caprine parainfluenza virus type 3 in sheep of China. Transbound Emerg Dis 66:1411–1416
Hao F, Wang Z, Mao L, Yang L, Zhang W, Li J, Wang X, Li W, Jiang J (2019) The novel caprine parainfluenza virus type 3 showed pathogenicity in Guinea pigs. Microb Pathog 134:103569
Jones G, Field A, Gilmour J, Rae A, Nettleton P, McLauchlan M (1982) Effects of experimental chronic pneumonia on bodyweight, feed intake and carcase composition of lambs. Vet Rec 110:168–173
Anderson AJ, Snelling TL, Moore HC, Blyth CC (2017) Advances in vaccines to prevent viral respiratory illnesses in children. Paediatr Drugs 19:523–531
WHO (2017) World Health Organization international clinical trials registry platform
Greenberg DP, Walker RE, Lee MS, Reisinger KS, Ward JI, Yogev R, Blatter MM, Yeh SH, Karron RA, Sangli C, Eubank L, Coelingh KL, Cordova JM, August MJ, Mehta HB, Chen W, Mendelman PM (2005) A bovine parainfluenza virus type 3 vaccine is safe and immunogenic in early infancy. J Infect Dis 191:1116–1122
Haller AA, Miller T, Mitiku M, Coelingh K (2000) Expression of the surface glycoproteins of human parainfluenza virus type 3 by bovine parainfluenza virus type 3, a novel attenuated virus vaccine vector. J Virol 74:11626–11635
Schmidt AC, Schaap-Nutt A, Bartlett EJ, Schomacker H, Boonyaratanakornkit J, Karron RA, Collins PL (2011) Progress in the development of human parainfluenza virus vaccines. Expert Rev Respir Med 5:515–526
Karron RA, Casey R, Thumar B, Surman S, Murphy BR, Collins PL, Schmidt AC (2011) The cDNA-derived investigational human parainfluenza virus type 3 vaccine rcp45 is well tolerated, infectious, and immunogenic in infants and young children. Pediatr Infect Dis J 30:e186–e191
Haanes EJ, Guimond P, Wardley R (1997) The bovine parainfluenza virus type-3 (BPIV-3) hemagglutinin/neuraminidase glycoprotein expressed in baculovirus protects calves against experimental BPIV-3 challenge. Vaccine 15:730–738
Zhu YM, Shi HF, Gao YR, **n JQ, Liu NH, **ang WH, Ren XG, Feng JK, Zhao LP, Xue F (2011) Isolation and genetic characterization of bovine parainfluenza virus type 3 from cattle in China. Vet Microbiol 149:446–451
King N, Gale C (1963) Studies on myxovirus parainfluenza-3 vaccine for prevention of ship** fever in cattle. J Am Vet Med Assoc 142:881–883
Gutekunst DE, Paton IM, Volenec FJ (1969) Parainfluenza-3 vaccine in cattle: comparative efficacy of intranasal and intramuscular routes. J Am Vet Med Assoc 155:1879–1885
Kirchhoff J, Uhlenbruck S, Keil GM, Schwegmann-Wessels C, Ganter M, Herrler G (2014) Infection of differentiated airway epithelial cells from caprine lungs by viruses of the bovine respiratory disease complex. Vet Microbiol 170:58–64
Liu X, Liang B, Liu X, Amaro-Carambot E, Surman S, Kwong PD, Graham BS, Collins PL, Munir S (2020) Human parainfluenza virus type 3 expressing the respiratory syncytial virus pre-fusion F protein modified for virion packaging yields protective intranasal vaccine candidates. PLoS One 15:e0228572
Fulton RW (2009) Bovine respiratory disease research (1983–2009). Anim Health Res Rev 10:131–139
Kerkhofs P, Tignon M, Petry H, Mawhinney I, Sustronck B (2004) Immune responses to bovine respiratory syncytial virus (BRSV) following use of an inactivated BRSV-PI3-Mannheimia haemolytica vaccine and a modified live BRSV–BVDV vaccine. Vet J 167:208–210
Perkins-Oines S, Dias N, Krafsur G, Abdelsalam K, Perry G, Ensley D, Jones C, Chase CC (2023) The effect of neonatal vaccination for bovine respiratory disease in the face of a dual challenge with bovine viral diarrhea virus and Mannheimia hemolytica. Vaccine 41:3080–3091
Bailly JE, McAuliffe JM, Durbin AP, Elkins WR, Collins PL, Murphy BR (2000) A recombinant human parainfluenza virus type 3 (PIV3) in which the nucleocapsid N protein has been replaced by that of bovine PIV3 is attenuated in primates. J Virol 74:3188–3195
Hore DE (1966) Isolation of ovine strains of parainfluenza virus serologically related to type 3. Vet Rec 79:466–467
Riedemann S, Montecinos M, Tadich N, Reinhardt G (1991) Serological survey for antibodies to parainfluenza-3 virus in sheep in Chile. Vet Rec 128:572
Contreras-Luna MJ, Ramírez-Martínez LA, Sarmiento Silva RE, Cruz Lazo C, Pérez Torres A, Sánchez-Betancourt JI (2017) Evidence of respiratory syncytial virus and parainfluenza-3 virus in Mexican sheep. Virusdisease 28:102–110
Li W, Mao L, Cheng S, Wang Q, Huang J, Deng J, Wang Z, Zhang W, Yang L, Hao F, Ding Y, Sun Y, Wei J, Jiang P, Jiang J (2014) A novel parainfluenza virus type 3 (PIV3) identified from goat herds with respiratory diseases in eastern China. Vet Microbiol 174:100–106
Ma Y, Wang Y, Zan X, Wu Y, Wang J, Li G, Chai C, Fu C, Wang S, Yin H, Wang W (2021) Phylogenetic and pathogenicity analysis of a novel lineage of caprine parainfluenza virus type 3. Microb Pathog 154:104854
Wells P, Sharp J, Rushton B, Gilmour N, Thompson D (1978) The effect of vaccination with a parainfluenza type 3 virus on pneumonia resulting from infection with parainfluenza type 3 virus and Pasteurella haemolytica. J Comp Pathol 88:253–259
Wang YQ, Liu Y, Wang YX, Wu YJ, Jia PY, Shan JJ, Wu J, Ma GH, Su ZG (2016) The potential adjuvanticity of quaternized chitosan hydrogel based microparticles for porcine reproductive and respiratory syndrome virus inactivated vaccine. Int Immunopharmacol 39:84–91
Renukaradhya GJ, Meng XJ, Calvert JG, Roof M, Lager KM (2015) Inactivated and subunit vaccines against porcine reproductive and respiratory syndrome: current status and future direction. Vaccine 33:3065–3072
Cox SJ, Barnett PV (2009) Experimental evaluation of foot-and-mouth disease vaccines for emergency use in ruminants and pigs: a review. Vet Res 40:13
Gao Q, Bao L, Mao H, Wang L, Xu K, Yang M, Li Y, Zhu L, Wang N, Lv Z, Gao H, Ge X, Kan B, Hu Y, Liu J, Cai F, Jiang D, Yin Y, Qin C, Li J, Gong X, Lou X, Shi W, Wu D, Zhang H, Zhu L, Deng W, Li Y, Lu J, Li C, Wang X, Yin W, Zhang Y, Qin C (2020) Development of an inactivated vaccine candidate for SARS-CoV-2. Science 369:77–81
Patil PK, Bayry J, Ramakrishna C, Hugar B, Misra LD, Prabhudas K, Natarajan C (2002) Immune responses of sheep to quadrivalent double emulsion foot-and-mouth disease vaccines: rate of development of immunity and variations among other ruminants. J Clin Microbiol 40:4367–4371
Smith W, Wells P, Burrells C, Dawson AM (1975) Immunoglobulins, antibodies and inhibitors of parainfluenza 3 virus in respiratory secretions of sheep. Arch Virol 49:329–337
Davies D, McCarthy AR, Penwarden RA (1980) The effect of vaccination of lambs with live parainfluenza virus type 3 on pneumonia produced by parainfluenza virus type 3 and Pasteurella haemolytica. N Z Vet J 28:201–202
Smith W (1975) The nasal secretion and serum antibody response of lambs following vaccination and aerosol challenge with parainfluenza 3 virus. Res Vet Sci 19:56–62
Davies D (1980) Isolation of parainfluenza virus type 3 from pneumonic lambs. N Z Vet J 28:148
Stauffer F, El-Bacha T, Da Poian AT (2006) Advances in the development of inactivated virus vaccines. Recent Pat Antiinfect Drug Discov 1:291–296
Barnett P, Pullen L, Williams L, Doel T (1996) International bank for foot-and-mouth disease vaccine: assessment of Montanide ISA 25 and ISA 206, two commercially available oil adjuvants. Vaccine 14:1187–1198
Garg R, Latimer L, Gomis S, Gerdts V, Potter A (2019) Maternal vaccination with a novel chimeric glycoprotein formulated with a polymer-based adjuvant provides protection from human parainfluenza virus type 3 in newborn lambs. Antiviral Res 162:54–60
Sharp J, Gilmour N, Thompson D, Rushton B (1978) Experimental infection of specific pathogen-free lambs with parainfluenza virus type 3 and Pasteurella haemolytica. J Comp Pathol 88:237–243
Acknowledgements
This study was supported by grant 2021ZD0013 from the Inner Mongolia Science and Technology Agency and grant XTCX2023-03 from the Science and Technology Bureau of Hohhot.
Funding
This work was supported by the Inner Mongolia Autonomous Region Major Science and Technology Project (2021ZD0013) and the Collaborative Innovation Project of Institutions of Higher Learning in Hohhot (XTCX2023-03).
Author information
Authors and Affiliations
Contributions
WW designed and initiated the study. YM participated in the study design, conducted most of the experiments and drafted the manuscript. JW, Youzhi W, Yan W, CG, KM, QS, and HW performed the animal experiments and collected the samples. XZ, YZ, TW, RN, JW and YH participated in the studies and analysed the data. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors confirm that the ethical policies of the journal, as noted on the journal’s author guidelines page, have been adhered to. This study was conducted in strict accordance with the Animal Management Regulations of the People’s Republic of China. All animal experiments were approved by the Institutional Animal Ethics Committee of Inner Mongolia University (Approval No. IMU-2021-sheep-044). The study was carried out in compliance with AVMA Guidelines for the Euthanasia of Animals.
Competing interests
The authors declare that they have no competing interests.
Additional information
Handling editor: Vincent Béringue.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ma, Y., Wang, J., Wu, Y. et al. Evaluation of the immunogenicity and protective efficacy of an inactivated vaccine candidate for sheep infected with ovine parainfluenza virus type 3. Vet Res 55, 82 (2024). https://doi.org/10.1186/s13567-024-01339-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13567-024-01339-1