
Abstract
Background
Vitamin D deficiency in critically ill patients is associated with poor outcomes, and vitamin D supplementation is recommended for patients with chronic kidney disease. Whether acute kidney injury (AKI) is associated with altered Vitamin D metabolism is unknown. We aimed to compare the longitudinal profiles of serum 25(OH)D and 1,25(OH)2D concentrations in critically ill patients with and without moderate to severe AKI and explore the impact of renal recovery and parathyroid hormone (PTH).
Methods
In this prospective, observational study in two centres in the UK, critically ill patients with and without AKI underwent serial measurement of serum 25(OH)D and 1,25(OH)2D and plasma PTH concentrations for 5 days. Linear mixed model analysis and sensitivity analyses were performed.
Results
Serial data of 137 patients were analysed. Seventy-one patients had AKI stage II/III of whom 23 recovered kidney function during the 5-day study period; 66 patients did not have AKI at enrolment of whom 14 developed new AKI. On day of enrolment, patients’ serum 25(OH)D concentrations were low (median 18 nmol/L) but there was no significant difference between patients with and without AKI. Median serum 1,25(OH)2D levels were significantly lower in patients with AKI II/III (41 pmol/L [IQR 26, 58]) compared to similarly unwell patients without AKI (54 pmol/L [IQR 33, 69]) during the 5-day period. Recovery of kidney function in patients with AKI was associated with a rise in 1,25(OH)2D concentrations. Plasma PTH results were impacted by serum calcium and magnesium levels but not associated with 1,25(OH)2D levels.
Conclusions
Critically ill patients with moderate-to-severe AKI have significantly lower serum 1,25(OH)2D concentrations than similarly sick patients without AKI but there was no difference in serum 25(OH)D concentrations. Recovery of AKI was associated with a rise in serum 1,25(OH)2D concentrations. More research is needed to investigate the health benefits and safety of supplementation with active vitamin D in critically ill patients with moderate-to-severe AKI.
Trial registration Clinicaltrials.gov (NCT02869919), registered on 16 May 2016.
Similar content being viewed by others

Background
Vitamin D deficiency affects about 40% of Europeans. [1] It is associated with adverse health outcomes, including increased mortality, muscle weakness and osteoporosis, increased susceptibility to sepsis, longer duration of mechanical ventilation and increased risk of acute kidney injury (AKI). [2]
In health, more than 95% of systemic vitamin D3 (Vit D3), also known as colecalciferol, is synthesized in the skin under ultraviolet B (UVB) irradiation and then converted to 25-hydroxyvitamin D (25(OH)D) by 25-hydroxylase in the liver, followed by hydroxylation to 1,25(OH)2D (also known as calcitriol) predominantly in proximal tubular cells. [3] The production of 1,25(OH)2D is tightly controlled, being stimulated by parathyroid hormone (PTH), and inhibited by calcium, phosphate and fibroblast growth factor-23 (FGF-23). [3] 1,25(OH)2D, the main bioactive metabolite of vitamin D, exerts the greatest physiological effect.
In chronic kidney disease (CKD), 1,25(OH)2D levels start to decline when glomerular filtration rate (GFR) falls to < 60 ml/min. To promote bone and cardiovascular health in patients, routine vitamin D supplementation (using alfacalcidol) is recommended for patients with CKD. [4] Acute kidney injury is a syndrome with dynamic trajectories. [5] Whether there is also a role for routine Vitamin D supplementation in patients with AKI is unknown. [6] A systematic review of data of 130 critically ill patients showed no difference in serum 25(OH)D levels between patients with and without AKI but significantly lower serum 1,25(OH)2D levels in AKI patients. [7] A population-based cohort study from Taiwan showed that patients with AKI who had dialysis and survived 90 days after hospital discharge had a significantly higher long-term risk of bone fractures compared to hospitalized patients without AKI, regardless of subsequent progression to end-stage kidney disease (ESKD). [8] The authors speculated that changes in vitamin D metabolism might have contributed but did not measure vitamin D levels.
Finally, several randomized controlled trials (RCTs) have investigated the role of vitamin D supplementation in critically ill patients, with and without AKI. A meta-analysis of 14 trials involving 2324 patients concluded that the supplementation of vitamin D had no effect on overall mortality. [9] Importantly, in 12 of 14 trials, Vitamin D3 (colecalciferol) was used for supplementation. Whether other active Vitamin D or other vitamin D metabolites would have been more effective is unclear. A more recent meta-analysis of 16 RCTs including 2449 patients also showed that different types of Vitamin D had been used in clinical trials. [10] Further, in eight studies, vitamin D was administered via the enteral route, whereas in seven studies, Vitamin D was administered intravenously or intramuscularly. The VITDALIZE is still actively recruiting. [11] In this international placebo-controlled double-blind RCT, 2400 adult patients with severe vitamin D deficiency are randomized to receiving a loading dose of 540,000 IU cholecalciferol, followed by 4000 IU daily for 90 days versus placebo.
The main objectives of this study were (i) to undertake serial measurements of 25(OH)D and 1,25(OH)2D concentrations in critically ill patients with and without moderate to severe AKI; (ii) to investigate whether there are differences in vitamin D metabolite concentrations between AKI patients who recover renal function and those without recovery; and (iii) to investigate the role of factors that usually impact vitamin D regulation, including gender, annual season, ionized calcium (iCa), Magnesium (Mg) and PTH [12].
Methods
Setting
This prospective observational study was conducted in two tertiary care hospitals in the National Health Service in the UK. Patients were recruited between July 2016 and January 2018. Data collection and laboratory analyses were completed in the following 18 months. Statistical analyses were delayed due to the COVID pandemic but completed in 2022.
Definitions
AKI was defined according to the serum creatinine and urine output criteria of the Kidney Disease Improving Global Outcomes (KDIGO) classification. [13, 14] Baseline kidney function was determined using the lowest serum creatinine result recorded in the patients’ medical notes in the 12 months before hospitalization. If no result was recorded in the medical notes, the primary care clinician and/or local hospital was contacted for additional information. If no baseline creatinine value was available, and there was no documented diagnosis or clinical suspicion of CKD, it was assumed that the patient’s baseline estimated glomerular filtration rate (eGFR) was > 45 mL/min/1.73 m2, and the serum creatinine was back calculated using the Modification of Diet in Renal Disease formula. [14]
Depending on the trajectories of kidney function during the 5-day follow-up period, we distinguished between patients with ‘persistent AKI II/III’, ‘no AKI throughout’, ‘development of new AKI’ and ‘AKI with recovery of kidney function’ during the 5-day period. [15] Kidney recovery was defined as a reduction in AKI stage or return to baseline kidney function, as per 16 th Acute Disease Quality Initiative expert consensus meeting. [15]
Participants
Consecutive adult patients in the intensive care unit (ICU) were screened daily for eligibility. [12] Patients were included in the AKI group if they were critically ill adults and had KDIGO defined AKI stage II or III for 36 h or less. Criteria for inclusion in the critically ill non-AKI group were: (i) no AKI, and (ii) concomitant cardiovascular and/or respiratory failure necessitating invasive or non-invasive respiratory support and/or treatment with catecholamines, with a requirement anticipated to last for longer than 24 h. Criteria for exclusion from either group were: (i) AKI stage I; (ii) AKI stage II or III for more than 36 h; (iii) known CKD stage 3b–5 (i.e. baseline eGFR < 45 mL/min/1.73m2); (iv) previous renal transplant; (v) known vitamin D deficiency (a documented diagnosis or laboratory Vitamin D value of < 50 nmol/L); (vi) known vitamin D supplementation in the last 3 months (either as a single agent or in a combination product); (vii) known hyperparathyroidism; (viii) need for total parenteral nutrition (TPN); (ix) life expectancy less than 48 h; (x) haemoglobin concentration < 70 g/L, or (xi) pregnancy. These exclusion criteria were agreed in order to eliminate any factors that may confound serum vitamin D metabolite concentrations. If patients were included but developed exclusion criteria during the 5-day follow-up period (i.e. initiation of TPN or vitamin D administration for clinical reasons), they were excluded from the analysis and replaced with another patient.
Study procedures
Blood samples for serial measurement of serum 25(OH)D and 1,25(OH)2D and plasma PTH were taken in the morning between 08.00 and 12.00 noon on the day of enrolment (within 36 h of the diagnosis of AKI stage II or III) and on day 5. Additional blood samples were taken on day 2 for measurement of serum 1,25(OH)2D concentration, owing to its shorter elimination half-life (~ 4 h). All samples were centrifuged at 3500 rpm for 10 min, then separated into aliquots and stored at − 80 °C until batch analysis after completion of patient recruitment.
Data collection
The following data were collected from the medical records: baseline demographics, type of organ failure, type of organ support, severity of illness [Acute Physiology and Chronic Health Evaluation (APACHE) II and Sequential Organ Failure Assessment (SOFA) score and SOFA minus renal score (SOFA-Renal)], routine biochemistry results and C-reactive protein (CRP), and ICU and hospital mortality.
Laboratory analysis
Serum concentrations of 25(OH)D and 1,25(OH)2D were measured using a liquid chromatography–mass spectrometry method, with a coefficient of variation (CV) of 7.3% for 25(OH)D. The lower limit of detection was 7 nmol/L. 1,25(OH)2D was measured using a standard ChemiLumunescent ImmunoAssay (Diasorin Liaison®). The intra-assay CVs were 1.9–2.3% across a range of concentrations from 39 to 200 pmol/L. The lower limit of detection was 12 pmol/L. Plasma PTH was measured by Roche automated analyser (Roche diagnostics Limited, West Sussex, UK). The reference range was 10–65 ng/L. Assay CVs for PTH were < 5% at PTH concentrations of 41 and 105 ng/L.
Sample size
The aim of this study was to investigate Vitamin D physiology in patients with and without AKI during a 5-day period. Based on data from Lai et al. [16], a sample size of 126 patients with complete data was considered to be necessary to detect a difference of 25 pmol/L in serum 1,25(OH)2D concentration between the AKI and non-AKU cohort, with a power of 80% and at a two-tailed significance level of 5% (assuming a standard deviation of 50 in each group).
To study trajectories in Vitamin D concentrations, it was important to have blood results available on day 5 for all enrolled patients. After 50 patients had been recruited, we performed an interim review of the case report forms and noted that only 28 patients (58%) were alive and still in the ICU and had blood samples taken on day 5. Based on these results, we concluded that we needed to recruit at least 230 patients in order to be able to analyse 126 patients with day 5 samples. To compensate for potential missing or incomplete data, we aimed to recruit at least 136 patients.
Statistical analysis
For the baseline characteristics, continuous variables were summarized using medians, and interquartile ranges (IQRs) and categorical variables were summarized using counts and percentages. Sequential Vitamin D metabolite concentrations were compared within the AKI and no AKI groups using the Mann–Whitney U Test. Multiple comparisons were accounted for by adjusting p-values with the Benjamini–Hochberg procedure.
For the inferential analysis, we used a linear mixed model which accounted for lack of independence of data within patients by modelling both fixed and random effects. We defined time as the number of days since enrolment. Model parameters were estimated using restricted maximum likelihood. In each model, we adjusted for kidney function, time, age, gender, ethnicity, season, and baseline CRP, ionized calcium concentrations, and ‘SOFA—Renal’ score. One model includes an interaction between kidney function (no AKI, persistent AKI II/III, new AKI, recovery of kidney function following AKI II/III) and time. We considered three different random effect structures, random intercept, random intercept with an uncorrelated slope, and random intercept with a correlated slope. We explored whether allowing the residual variances of each time point and/or kidney function improved the model. Satterthwaite’s method was used to estimate the p-values and confidence intervals (CIs) of the fixed effects. The model with the smallest Bayesian information criterion was chosen as the final model. We defined statistical significance at p < 0.05. All analyses were performed using R v4.1.3 and mixed models were fit and tested using the lme4 and lmerTest packages, respectively. As a sensitivity analysis, we took the natural logarithm of the outcome before fitting the model to see how stable the model coefficients were.
Trial registration
The study was registered with clinicaltrials.gov (NCT02869919) on 16 May 2016.
Results
Baseline characteristics
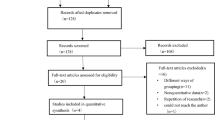
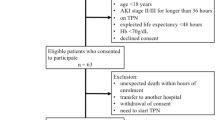
Patient recruitment ceased after enrolment of 137 patients with complete data for analysis (Fig. 1, Table 1). Seventy-four patients had AKI stage II/III of whom 59 were treated with renal replacement therapy (RRT); 23 patients recovered kidney function during the 5-day follow-up period. Sixty-three patients did not have AKI at enrolment of whom 11 developed new AKI during the 5-day study period. (Fig. 1) Patients with AKI II/III at enrolment had significantly higher APACHE II and ‘SOFA–Renal’ scores at ICU admission compared to patients without AKI at enrolment but there was no statistically significant difference in age and gender. (Table 2) ICU, hospital and 30-day mortality were significantly higher in the AKI II/III cohort.

Flowchart AKI Acute kidney injury, AKD Acute kidney disease, ICU Intensive care unit, RRT Renal replacement therapy, SCr at baseline Serum creatinine returned to baseline. * patient developed new AKI after day 0 but died on day 5
25(OH) vitamin D results
Six patients had missing 25(OH)D data and were not included in the mixed model. Among the remaining 131 patients, serum 25(OH)D concentrations were low (median 18 nmol/L) on the day of enrolment across the whole patient cohort when compared with reference ranges for the general population. (Additional file 1: Table S1). In patients with AKI II/III at enrolment, serum 25(OH)D concentrations were approximately 5 nmol/l lower than in patients without AKI throughout the study, whether they recovered renal function or not. (Additional file 1: Table S2) In the three kidney function categories ‘normal kidney function throughout’, ‘AKI II/III throughout’, and ‘recovered from AKI II/III’, serum 25(OH)D levels increased between day 0 and day 5, but the changes were statistically not significant (Fig. 2a, Additional file 1: Tables S1 and Additional file 1: Figure S1).

Changes in serum 25(OH)D, serum 1,25(OH)2D and plasma PTH concentrations of each patient by kidney function. a Serum 25(OH)D concentrations (n = 131). AKI Acute kidney injury b Serum 1, 25(OH)2D concentrations (n = 131). AKI Acute kidney injury. c Plasma PTH concentrations (n = 133). AKI Acute kidney injury, PTH Parathyroid hormone. Mean (solid) and median (dashed) results are highlighted at each time point. Faint lines represent individual patients.
Patients admitted in winter had significantly lower serum 25(OH)D concentrations than those admitted in summer. The mean difference was 12.0 nmol/l (95% CI 5.6 to 18.4; p < 0.001). (Additional file 1: Table S2) Among patients who developed new AKI and patients with AKI II/III who recovered kidney function during the 5-day period, females had a higher 25(OH)D result on the day of enrolment than males. (Additional file 1: Figure S2).
Sensitivity analysis
The coefficients in the log-linear model had the same directions of association as the linear model. Male gender and winter season were independently associated with lower 25(OH)D results (Additional file 1: Table S3).
1,25(OH)2D results
Six patients (4%) had missing 1,25(OH)2D results and were not included in the mixed model. Serum 1,25(OH)2D concentrations rose between day 0 and day 5 in patients without AKI and in AKI patients who recovered kidney function during the 5-day follow-up period. (Fig. 2b and Additional file 1: Table S4) In contrast, in patients who did not have AKI at enrolment but developed new AKI, and in patients who had AKI II/III throughout the 5-day period, serum 1,25(OH)2D concentrations decreased during the follow-up period. Compared to the cohort with normal kidney function throughout, patients who developed new AKI and patients with AKI II/III throughout the 5-day period had significantly lower 1,25(OH)2D results at each time point. (Additional file 1: Tables S5 and S6) Similarly, AKI patients with renal recovery had significantly lower 1,25(OH)2D results at each time point compared to patients with normal kidney function throughout the 5-day period.
There was no difference in these trajectories within each category between male and female patients. (Additional file 1: figure S3) Patients admitted in winter had lower 1,25(OH)2D results than those admitted in summer with a mean difference of 9.8 pmol/l (95% CI − 0.8 to 20.4) which was statistically not significant (p = 0.069). (Additional file 1: Table S5).
Sensitivity analysis
Patients with normal kidney function throughout and patients with AKI II/III who recovered kidney function during the 5-day period had higher 1,25(OH)2D levels than patients with persistent or new AKI. (Additional file 1: Table S6) Considering the variables outside the kidney function and time interaction, the log-linear model coefficients had the same directions of association as the linear model. (Additional file 1: Table S5 and S7) Age, gender, ethnicity, season, baseline CRP and baseline SOFA-renal score were not independently associated with 1,25(OH)2D concentrations.
PTH
On day of enrolment, patients without AKI had lower plasma PTH concentrations compared to patients with AKI. (Fig. 2c and Additional file 1: Table S8) In all kidney function categories, the PTH results on day 5 were lower than on day 0 but the decline was most marked in patients with AKI who recovered kidney function during the 5-day period. (Additional file 1: Table S8 and Figure S3).
PTH concentrations were related to serum ionized calcium and magnesium concentrations. A serum ionized calcium concentration of 0.1 mmol/L above a patient’s average value was significantly (p < 0.001) associated with a PTH value 13.8 pg/ml lower (95% CI 7.4 to 20.1) than their average. (Additional file 1: Table S9) A magnesium value 0.1 mmol/l above a patient’s average was significantly (p = 0.040) associated with a PTH value 2.1 pg/ml higher (95% CI 0.1 to 4.2) than the patient’s average.
Discussion
The key findings of this prospective two-centre observational study are: 1) Critically ill adult patients with AKI II/III had significantly lower serum 1,25(OH)2D concentrations compared to similarly unwell patients without AKI; 2) Serum 25(OH)D concentrations were low with no significant difference between critically ill patients with and without AKI; iii) In patients with AKI II/III, recovery of kidney function was associated with an increase in 1,25(OH)2D levels in contrast to patients with AKI II/III who did not recover kidney function; and iv) PTH concentrations were impacted by serum calcium and magnesium levels but did not correlate with changes in serum 1,25(OH)2D concentrations.
Vitamin D has pleiotropic effects on immunity, endothelial and mucosal functions, and glucose and calcium metabolism. 1,25(OH)2D is the main bioactive metabolite of vitamin D with the greatest physiological effect. Its half-life is much shorter (of the order of 4 h) than that of vitamin D3 (24 h) or 25(OH)D (3 weeks). Although deficiency is associated with poor outcomes [2, 17,18,19], the thresholds for sufficiency / deficiency often relate to bone health, without consideration of other physiological effects. Recommendations when to supplement Vitamin D differ in many countries. [18] The European Society for Clinical Nutrition and Metabolism considers a serum/plasma 25(OH)D concentration below 50 nmol/L (or 20 ng/ml) to define vitamin D deficiency [1]. A cut-off < 25 nmol/L (or 10 ng/mL) increases the risk for osteomalacia and nutritional rickets dramatically and is considered to determine severe vitamin D deficiency.
The optimal vitamin D concentration during critical illness is unknown. Besides critical illness itself, immobilization, fluid overload, plasma exchange and cardiopulmonary bypass have been reported to impact serum vitamin D concentrations. [2] Thus, the question remains whether low vitamin D values in critically ill patients reflect deficiency, greater severity of illness, the result of therapeutic interventions or are simply considered risk factors for poor outcomes. [18, 20] The role of routine Vitamin D supplementation in all critically ill patients remains under investigation but has not been explored specifically in critically ill patients with AKI. [9, 11, 18, 21]
Importantly, the relationship between AKI and vitamin D appears bi-directional. Loss of functioning nephrons impacts the 1-hydroxylase negatively and affects the ability to generate 1,25(OH)2D. [22, 23] On the other hand, experimental models have shown that vitamin D depletion contributes to AKI development due to several mechanisms, including upregulation of the renin–angiotensin–aldosterone system, increased expression of renal vascular renin and dysregulation of the immune system. [23,24,25] Vitamin D deficiency may also exacerbate AKI by worsening the renal vascular condition, preventing healing of renal ischaemia–reperfusion injury (IRI) and accelerating AKI-to-CKD progression. [25,26,27,28]
The role of supplementation with active vitamin D (calcitriol) in AKI has been investigated in experimental studies in rats, using different analogues in varying doses with heterogeneous results. Ersan et al. reported that pre-treatment with paricalcitol resulted in amelioration of IRI-induced AKI via a matrix metalloproteinase-dependent inflammatory mechanism. [29] Others showed that paricalcitol ameliorated liposaccharide (LPS)-associated AKI and cisplatin-induced AKI. [30, 31] Hamzawy et al. demonstrated that pre-treatment with oxacalcitriol ameliorated IRI-induced AKI through anti-inflammatory mechanisms. [32] In another experimental study, the administration of 1,25(OH)2D did not ameliorate gentamicin-induced AKI. [33] Arfian et al. investigated the effect of intraperitoneal administration of colecalciferol on IRI-induced AKI and found that AKI was mitigated through reduction in inflammation. [34] Outside AKI, two different oral doses of vitamin D (500 IU/kg and 1000 IU/kg) were used in an experimental model of paracetamol-induced liver failure. [35] The lower dose of 500 IU/kg was found to have a greater protective effect.
Our findings complement and advance the existing literature on Vitamin D metabolism in critically ill patients. Similar to previous reports, we found no difference in serum 25(OH)D concentrations between the AKI and non-AKI cohort. [7, 16] Instead, we demonstrated significant differences in 1,25(OH)2D concentrations between patients with and without severe AKI. By consensus, serum/plasma concentration of 25(OH)D is recognized as a valid biomarker for vitamin D status. [1] Our data suggest that 1,25(OH)2D deficiency exists and may be under-recognized, especially in critically ill patients with moderate to severe AKI. Importantly, colecalciferol has been used for supplementation in several clinical intervention studies but may be inappropriate and ineffective in patients with AKI. [36,37,38]
Our data shows that on day of enrolment, patients without AKI had lower plasma PTH concentrations compared to patients with AKI. In those who recovered kidney function by day 5, PTH levels declined again. These data are consistent with other human studies in the literature confirming acute elevations of PTH with AKI that subsequently returned to normal when AKI resolved. with resolution of AKI.. [39, 40] It is postulated that low concentrations of serum 1,25(OH)2D and secondary hypocalcaemia may contribute to secondary hyperparathyroidism in AKI.
It is well-known that after the induction of sustained hypocalcaemia, preformed PTH is secreted into the blood within 1 min and restoration of normocalcaemia results in a decrease in PTH levels with an apparent half-life of approximately 3 min. [41, 42]
Despite the strengths of our study, we acknowledge some limitations. First, we aimed to exclude patients taking vitamin D supplements from participating but acknowledge that it is possible that patients taking over-the-counter or prescribed vitamin D supplements may have been inadvertently included despite our best effort. The low levels of 25(OH)D observed and low variability within the data at day 0 suggest that this was not widespread. Second, we recruited patients in two tertiary care centres in the United Kingdom and acknowledge that our results may not be generalizable to patients in other geographical areas. Third, we included patients with AKI of any aetiology were included, promoting the generalizability of the findings. Nonetheless, we acknowledge that certain AKI sub-phenotypes may have a higher risk of 1,25(OH)2D deficiency than others. Consideration of AKI aetiology may be useful in further defining a population with the lowest vitamin D levels and to enrich future intervention studies. Fourth, we have some missing results because blood sampling was not done due to competing clinical requirements, or blood samples were underfilled and unsuitable for analysis. The statistical analyses were adjusted accordingly. Fifth, we did not measure FGF-23 and vitamin D binding protein consistently and reliably in all patients, as originally planned. We are aware that elevated serum FGF-23 correlate with increased mortality in critically ill patients independent of vitamin D status. Also, FGF-23 measurements may be outside the detectable, validated range for commercially available tests. [43] Sixth, we had planned to take samples on day of ICU discharge in all ICU survivors. However, this proved to be challenging. Our interim analysis after 50 patients showed that these samples had not been taken in more than 50% of patients due to a variety of reasons including emergency transfer to another hospitals or discharge from ICU outside usual working hours, patient refusal to have blood test taken, or simple human oversight. Further, it became apparent that length of stay in ICU after enrolment and day of ICU discharge were very variable between patients. For these reasons, we elected not to analyse the results to avoid misinterpretation. Seventh, we defined renal recovery as a reduction in AKI stage or return to baseline kidney function but know that serum creatinine is not a reliable biomarker of renal recovery. Further, we only monitored renal function for 5 days and acknowledge that renal recovery may take longer to develop. Finally, the majority of patients with AKI II/III received RRT during the 5-day study period and the sample size did not allow formal comparison between the RRT and non-RRT cohorts, as originally planned. However, in a previous study, we showed that vitamin D is not removed during RRT and that serum vitamin D concentrations did not significantly differ between patients with AKI III treated with or without RRT. [44]
Conclusions
Among critically ill adult patients, serial serum concentrations of 1,25(OH)2D were significantly lower in patients with moderate-to-severe AKI compared to critically ill patients without AKI. There was no statistically significant difference in serum 25(OH)D concentrations. More research is needed to define vitamin D deficiency in critically ill patients with AKI. Our results support a case to investigate the health benefits and safety of supplementation with active vitamin D analogues in this cohort.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AKI:
-
Acute kidney injury
- AKD:
-
Acute kidney disease
- AOR:
-
Adjusted odds ratio
- APACHE:
-
Acute physiology and chronic health evaluation
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- CRP:
-
C-reactive protein
- CV:
-
Coefficient of variation
- ECMO:
-
Extracorporeal membrane oxygenation
- eGFR:
-
Estimated glomerular filtration rate
- ESKD:
-
End stage kidney disease
- FGF-23:
-
Fibroblast growth factor-23
- GFR:
-
Glomerular filtration rate
- GI:
-
Gastrointestinal
- ICU:
-
Intensive care unit
- IQR:
-
Interquartile range
- IRI:
-
Ischaemia-reperfusion injury
- KDIGO:
-
Kidney Disease Improving Global Outcomes
- LPS:
-
Liposaccharide
- PTH:
-
Parathyroid hormone
- RRT:
-
Renal replacement therapy
- SOFA:
-
Sequential Organ Failure Assessment
- TPN:
-
Total parenteral nutrition
- UVB:
-
Ultraviolet B
References
Berger MM, Shenkin A, Schweinlin A, Amrein K, Augsburger M, Biesalski HK, Bischoff SC, Casaer MP, Gundogan K, Lepp HL, et al. ESPEN micronutrient guideline. Clin Nutr. 2022;41(6):1357–424.
Amrein K, Christopher KB, McNally JD. Understanding vitamin D deficiency in intensive care patients. Intensive Care Med. 2015;41(11):1961–4.
Bikle DD: Vitamin D: production, metabolism and mechanisms of action. In: Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J eds. Endotext. South Dartmouth
Duranton F, Rodriguez-Ortiz ME, Duny Y, Rodriguez M, Daurès JP, Argilés A. Vitamin D treatment and mortality in chronic kidney disease: a systematic review and meta-analysis. Am J Nephrol. 2013;37(3):239–48.
Ostermann M, Basu RK, Mehta RL. Acute kidney injury. Intensive Care Med. 2023;49(2):219–22.
Ostermann M, Macedo E, Oudemans-van Straaten H. How to feed a patient with acute kidney injury. Intensive Care Med. 2019;45(7):1006–8.
Zhang H, Jiang Y, Shi N, Lu YQ. Serum vitamin D levels and acute kidney injury: a systemic review and meta-analysis. Sci Rep. 2022;12(1):20365.
Wang WJ, Chao CT, Huang YC, Wang CY, Chang CH, Huang TM, Lai CF, Huang HY, Shiao CC, Chu TS, et al. The impact of acute kidney injury with temporary dialysis on the risk of fracture. J Bone Miner Res. 2014;29(3):676–84.
Shen H, Mei Y, Zhang K, Xu X. The effect of vitamin D supplementation on clinical outcomes for critically Ill patients: a systemic review and meta-analysis of randomized clinical trials. Front Nutr. 2021;8:664940.
Menger J, Lee ZY, Notz Q, Wallqvist J, Hasan MS, Elke G, Dworschak M, Meybohm P, Heyland DK, Stoppe C. Administration of vitamin D and its metabolites in critically ill adult patients: an updated systematic review with meta-analysis of randomized controlled trials. Crit Care. 2022;26(1):268.
Amrein K, Parekh D, Westphal S, Preiser JC, Berghold A, Riedl R, Eller P, Schellongowski P, Thickett D, Meybohm P. Effect of high-dose vitamin D3 on 28-day mortality in adult critically ill patients with severe vitamin D deficiency: a study protocol of a multicentre, placebo-controlled double-blind phase III RCT (the VITDALIZE study). BMJ Open. 2019;9(11):e031083.
Cameron LK, Lei K, Smith S, Doyle NL, Doyle JF, Flynn K, Purchase N, Smith J, Chan K, Kamara F, et al. Vitamin D levels in critically ill patients with acute kidney injury: a protocol for a prospective cohort study (VID-AKI). BMJ Open. 2017;7(7):e016486.
Ostermann M, Wu V, Sokolov D, Lumlertgul N. Definitions of acute renal dysfunction: an evolving clinical and biomarker paradigm. Curr Opin Crit Care. 2021;27(6):553–9.
Kellum JA, Lameire N. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (part 1). Crit Care. 2013;17(1):204.
Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, Bittleman D, Cruz D, Endre Z, Fitzgerald RL, et al. Acute kidney disease and renal recovery: consensus report of the acute disease quality initiative (ADQI) 16 workgroup. Nat Rev Nephrol. 2017;13(4):241–57.
Lai L, Qian J, Yang Y, **e Q, You H, Zhou Y, Ma S, Hao C, Gu Y, Ding F. Is the serum vitamin D level at the time of hospital-acquired acute kidney injury diagnosis associated with prognosis? PLoS ONE. 2013;8(5):e64964.
Christakos S, Dhawan P, Verstuyf A, Verlinden L, Carmeliet G. Vitamin D: metabolism, molecular mechanism of action, and pleiotropic effects. Physiol Rev. 2016;96(1):365–408.
Amrein K, Scherkl M, Hoffmann M, Neuwersch-Sommeregger S, Köstenberger M, Tmava Berisha A, Martucci G, Pilz S, Malle O. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74(11):1498–513.
Hurst EA, Mellanby RJ, Handel I, Griffith DM, Rossi AG, Walsh TS, Shankar-Hari M, Dunning J, Homer NZ, Denham SG, et al. Vitamin D insufficiency in COVID-19 and influenza A, and critical illness survivors: a cross-sectional study. BMJ Open. 2021;11(10):e055435.
Lee P, Nair P, Eisman JA, Center JR. Vitamin D deficiency in the intensive care unit: an invisible accomplice to morbidity and mortality? Intensive Care Med. 2009;35(12):2028–32.
Amrein K, Oudemans-van Straaten HM, Berger MM. Vitamin therapy in critically ill patients: focus on thiamine, vitamin C, and vitamin D. Intensive Care Med. 2018;44(11):1940–4.
Omdahl JL, Morris HA, May BK. Hydroxylase enzymes of the vitamin D pathway: expression, function, and regulation. Annu Rev Nutr. 2002;22:139–66.
Graidis S, Papavramidis TS, Papaioannou M. Vitamin D and acute kidney injury: a two-way causality relation and a predictive, prognostic, and therapeutic role of vitamin D. Front Nutr. 2020;7:630951.
Zhang Y, Kong J, Deb DK, Chang A, Li YC. Vitamin D receptor attenuates renal fibrosis by suppressing the renin-angiotensin system. J Am Soc Nephrol. 2010;21(6):966–73.
Braun AB, Christopher KB. Vitamin D in acute kidney injury. Inflamm Allergy Drug Targets. 2013;12(4):262–72.
de Bragança AC, Volpini RA, Mehrotra P, Andrade L, Basile DP. Vitamin D deficiency contributes to vascular damage in sustained ischemic acute kidney injury. Physiol Rep. 2016;4(13):e12829.
de Bragança AC, Volpini RA, Canale D, Gonçalves JG, Shimizu MH, Sanches TR, Seguro AC, Andrade L. Vitamin D deficiency aggravates ischemic acute kidney injury in rats. Physiol Rep. 2015;3(3):e12331.
Gonçalves JG, de Bragança AC, Canale D, Shimizu MH, Sanches TR, Moysés RM, Andrade L, Seguro AC, Volpini RA. Vitamin D deficiency aggravates chronic kidney disease progression after ischemic acute kidney injury. PLoS ONE. 2014;9(9):e107228.
Ersan S, Celik A, Tanrisev M, Kose I, Cavdar Z, Unlu M, Kocak A, Ural C, Yilmaz B, Kose T. Pretreatment with paricalcitol attenuates level and expression of matrix metalloproteinases in a rat model of renal ischemia-reperfusion injury. Clin Nephrol. 2017;88(11):231–8.
Xu S, Chen YH, Tan ZX, **e DD, Zhang C, **a MZ, Wang H, Zhao H, Xu DX, Yu DX. Vitamin D3 pretreatment alleviates renal oxidative stress in lipopolysaccharide-induced acute kidney injury. J Steroid Biochem Mol Biol. 2015;152:133–41.
Park JW, Cho JW, Joo SY, Kim CS, Choi JS, Bae EH, Ma SK, Kim SH, Lee J, Kim SW. Paricalcitol prevents cisplatin-induced renal injury by suppressing apoptosis and proliferation. Eur J Pharmacol. 2012;683(1–3):301–9.
Hamzawy M, Gouda SAA, Rashed L, Morcos MA, Shoukry H, Sharawy N. 22-oxacalcitriol prevents acute kidney injury via inhibition of apoptosis and enhancement of autophagy. Clin Exp Nephrol. 2019;23(1):43–55.
Hur E, Garip A, Camyar A, Ilgun S, Ozisik M, Tuna S, Olukman M, Narli Ozdemir Z, Yildirim Sozmen E, Sen S, et al. The effects of vitamin d on gentamicin-induced acute kidney injury in experimental rat model. Int J Endocrinol. 2013;2013:313528.
Arfian N, Budiharjo S, Wibisono DP, Setyaningsih WAW, Romi MM, Saputri R, Rofiah EK, Rahmanti T, Agustin M, Sari DCR. Vitamin D ameliorates kidney ischemia reperfusion injury via reduction of inflammation and myofibroblast expansion. Kobe J Med Sci. 2020;65(4):E138-e143.
Abo El-Magd NF, Eraky SM. The molecular mechanism underlining the preventive effect of vitamin D against hepatic and renal acute toxicity through the NrF2/ BACH1/ HO-1 pathway. Life Sci. 2020;244:117331.
Quraishi SA, De Pascale G, Needleman JS, Nakazawa H, Kaneki M, Bajwa EK, Camargo CA Jr, Bhan I. Effect of cholecalciferol supplementation on vitamin D status and cathelicidin levels in sepsis: a randomized placebo-controlled trial. Crit Care Med. 2015;43(9):1928–37.
Amrein K, Schnedl C, Holl A, Riedl R, Christopher KB, Pachler C, Urbanic Purkart T, Waltensdorfer A, Münch A, Warnkross H, et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: the VITdAL-ICU randomized clinical trial. JAMA. 2014;312(15):1520–30.
Nair P, Venkatesh B, Lee P, Kerr S, Hoechter DJ, Dimeski G, Grice J, Myburgh J, Center JR. A randomized study of a single dose of intramuscular cholecalciferol in critically Ill adults. Crit Care Med. 2015;43(11):2313–20.
Pietrek J, Kokot F, Kuska J. Serum 25-hydroxyvitamin D and parathyroid hormone in patients with acute renal failure. Kidney Int. 1978;13(2):178–85.
Neyra JA, Moe OW. Bone dysregulation in acute kidney injury. Nephron. 2023;147(12):747–53.
Kumar R, Thompson JR. The regulation of parathyroid hormone secretion and synthesis. J Am Soc Nephrol. 2011;22(2):216–24.
Raimundo M, Crichton S, Lei K, Sanderson B, Smith J, Brooks J, Ng J, Lemmich Smith J, McKenzie C, Beale R, et al. Maintaining normal levels of ionized calcium during citrate-based renal replacement therapy is associated with stable parathyroid hormone levels. Nephron Clin Pract. 2013;124(1–2):124–31.
Thein OS, Ali NA, Mahida RY, Dancer RCA, Ostermann M, Amrein K, Martucci G, Scott A, Thickett DR, Parekh D. Raised FGF23 correlates to increased mortality in critical illness, independent of vitamin D. Biology. 2023;12(2):309.
Ostermann M, Summers J, Lei K, Card D, Harrington DJ, Sherwood R, Turner C, Dalton N, Peacock J, Bear DE. Micronutrients in critically ill patients with severe acute kidney injury—a prospective study. Sci Rep. 2020;10(1):1505.
Acknowledgements
The authors would like to thank the research nurses in the critical care departments of the participating institutions for supporting the study.
Funding
This work was supported by independent research funding from Fresenius Medical Care. The sponsor was not involved in the design of the protocol and had no involvement in the conduct of the study. The results will remain intellectual property of the research team. LKC’s involvement was supported by the Biomedical Research Centre at Guy’s and St Thomas’ NHS Foundation Trust.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Sampling and data collection were performed by LC, RL and AB. The laboratory analyses were performed by KV and GH. DJH assisted with the laboratory analyses. The statistical analyses were done by LLC and WY. The first draft of the manuscript was written by MO. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by a National Research Ethics Committee in the UK (London Camberwell St Giles) (IRAS 196968) and carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). Written informed consent was obtained from participants or provided by a personal or professional consultee if the patient did not have capacity to consent for themselves. In a case where a consultee had given permission for the patient to take part, the patient was invited to give informed consent to continue participation or to withdraw from further participation as soon as they regained capacity.
Consent for publication
Written consent for publication was obtained from participants or provided by a personal or professional consultee if the patient did not have capacity to consent for themselves. In a case where a consultee gave permission for the patient to take part, the patient was informed and invited to give informed consent for publication as soon as they regained capacity.
Competing interests
The authors declare no conflict of interest related to this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Figure S1:
Changes in 25(OH)D measurements by kidney function and gender. Table S1a: Serum 25(OH)D concentrations by kidney function and time point. Table S1b: Coefficient estimates for the final 25(OH)D model.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cameron, L.K., Ledwaba-Chapman, L., Voong, K. et al. Vitamin D metabolism in critically ill patients with acute kidney injury: a prospective observational study. Crit Care 28, 108 (2024). https://doi.org/10.1186/s13054-024-04869-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-024-04869-4