
Abstract
Background
There is currently no standard treatment for locoregional recurrence of esophageal squamous cell carcinoma (ESCC) previously treated with radiotherapy. This study aimed to assess the efficacy and safety of re-irradiation for ESCC patients with locoregional recurrence.
Methods
The PubMed, EmBase, and Cochrane library databases were systematically searched for eligible studies published before January 2021. The pooled effect estimates were calculated using the random effects model. Subgroup analyses were conducted to assess the treatment effectiveness of re-irradiation based on specific characteristics.
Results
Nine retrospective studies including 573 ESCC patients with locoregional recurrence were selected. The pooled incidences of the 1-year, 2-year, 3-year, and 5-year survival for patients after re-irradiation were 59% (95% confidence interval [CI]: 35–83; P < 0.001), 25% (95% CI: 16–33; P < 0.001), 25% (95% CI: 4–45; P = 0.017), and 15% (95% CI: 2–27; P = 0.024), respectively. The rates of complete response and local re-recurrence after re-irradiation were 54% (95% CI: 21–88; P = 0.001) and 62% (95% CI: 55–70; P < 0.001), respectively. The median overall survival and local failure-free survival for patients after re-irradiation were 13.94 months (95% CI: 4.18–46.51; P < 0.001) and 11.01 months (95% CI: 5.99–20.22; P < 0.001), respectively. Grade ≥ 3 adverse events of esophageal perforation, tracheoesophageal fistula, and radiation pneumonitis were significantly more common after re-irradiation.
Conclusions
This study found that re-irradiation for ESCC patients with locoregional recurrence after previous radiotherapy was feasible. However, patients should be carefully observed in order to treat associated adverse events, including esophageal perforation, tracheoesophageal fistula, and radiation pneumonitis.
Similar content being viewed by others


Introduction
Esophageal cancer is the eighth most common cancer worldwide, with more than 450,000 new cases annually, and the sixth leading cause of cancer-related deaths [1]. Esophageal squamous cell carcinoma (ESCC) is the predominant histological type of esophageal cancer [2]. Although patients with early ESCC undergo esophagectomy, most ESCC patients are diagnosed with locally advanced disease. Therefore, surgery alone is usually insufficient, and radiotherapy or chemotherapy are administered [3, 4]. However, the prognosis of ESCC remains poor, and local recurrence or metastasis play a critical role in treatment failure and mortality [5].
Previous studies have shown that local recurrence is the major cause of ESCC recurrence after definitive chemoradiotherapy, which accounts for nearly 40–60% of ESCC cases [6, 7]. Re-irradiation is a common salvage treatment strategy and is widely administered for recurrent ESCC after radical radiotherapy or chemoradiotherapy. Chen et al. found that re-irradiation was able to relieve symptoms and prolong survival [8]. However, the efficacy of re-irradiation for locoregional recurrent ESCC previously treated with radiotherapy is variable, and whether the efficacy of re-irradiation is affected by patient characteristics remains controversial. We therefore performed a systematic review and meta-analysis to assess the efficacy and safety of re-irradiation for ESCC patients with locoregional recurrence who were previously treated with radiotherapy.
Methods
Search strategy and selection criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis guideline was used to guide this systematic review and meta-analysis [9]. Studies investigating the treatment effects of re-irradiation for patients with locoregional recurrent ESCC previously treated with radiotherapy were eligible. Only studies published in English were included. The PubMed, EmBase, and Cochrane library databases were searched for eligible studies published through January 2021, and the following search terms were used: esophageal squamous cell carcinoma, recurrence or recurrent, and radiotherapy or irradiation. We also manually reviewed the reference lists of retrieved studies to identify any additional studies that met the inclusion criteria.
The inclusion criteria were as follows: (1) Study design: retrospective, prospective, or randomized controlled trials; (2) Patients: patients with recurrent ESCC previously treated with definitive radiotherapy; (3) Intervention: re-irradiation; and (4) Outcomes: survival rate at 1, 2, 3, or 5 years, complete response, local re-recurrence, overall survival, local failure-free survival, and grade ≥ 3 adverse events. Study selection was performed by two reviewers, and conflicts between reviewers was settled by group discussion until a consensus was reached.
Data collection and quality assessment
Two reviewers independently extracted the following information: first author’s name, publication year, country, study design, sample size, mean age, male proportion, tumor stage, interval from prior therapy to irradiation, total radiation dose, and reported outcomes. The quality of each individual study was assessed using the Newcastle–Ottawa Scale, and the starring system for each study ranged from 0 to 9 [10]. Studies with 6 stars were considered to be of moderate quality, and studies with 4 or 5 stars were regarded as low quality. Inconsistent results between reviewers for extracted data and quality assessment were settled by an additional reviewer after referring to the original article.
Statistical analysis
The pooled incidence of survival at 1, 2, 3, and 5 years, complete response, local re-recurrence, and grade ≥ 3 adverse events were calculated based on the number of events and total patients, whereas pooled overall survival and local failure-free survival were calculated based on mean survival and 95% confidence intervals (CIs). The pooled effect estimates were calculated using the random effects model, and underlying variations across included studies were considered [11, 12]. Heterogeneity among the included studies for each outcome was assessed using I2 and the Q statistic, and significant heterogeneity was defined as I2 > 50.0% or P < 0.10 [13, 14]. The robustness of the pooled conclusion was assessed using sensitivity analysis by sequentially removing a single study [15]. Subgroup analyses for survival at 1, 2, 3, and 5 years were also performed according to sample size, mean age, male proportion, tumor stage, interval from prior therapy to radiotherapy, and study quality, and the differences between subgroups were assessed using the interaction P test [16]. Funnel plot, Egger test, and Begg’s tests were used to assess potential publication bias [17, 18]. The P values for pooled conclusions are two-sided, and the inspection level was 0.05. All statistical analyses in this study were performed using STATA software (version 10.0; Stata Corporation, College Station, TX, USA).
Results
Literature search
A total of 781 articles were identified from initial searches of the PubMed, EmBase, and Cochrane library databases, and 422 studies were retained after duplicate titles were removed. A further 390 studies were excluded because they covered irrelevant topics. The remaining 32 studies were retrieved for full-text evaluation, and 23 studies were excluded for the following reasons: not recurrent ESCC (n = 15), patients were previously without radiotherapy (n = 5), and other interventions (n = 3). Reviewing the reference lists yielded one additional potential study, but this study was also retrieved by our electronic search. Finally, nine studies were selected for the final meta-analysis (Fig. 1) [19,20,21,22,23,24,25,26,27].

The PRISMA flowchart for study selection process
Study characteristics
The characteristics of the included studies and patients are summarized in Table 1. All of the studies were retrospective, and a total of 573 ESCC patients with locoregional recurrence were included. Four studies were conducted in Japan, four studies were conducted in China, and one study was conducted in Korea. The mean age for patients ranged from 60.8 years to 72.5 years, and the male proportion ranged from 49.1 to 100.0%. Four studies were of moderate quality, and the remaining five studies were of low quality.
Survival rate at 1, 2, 3, and 5 years
Six, five, four, and five studies reported the effects of re-irradiation on survival at 1, 2, 3, and 5 years, respectively (Fig. 2). The pooled incidences of 1-year, 2-year, 3-year, and 5-year survival for patients after re-irradiation were 59% (95% confidence interval [CI]: 35–83; P < 0.001), 25% (95% CI: 16–33; P < 0.001), 25% (95% CI: 4–45; P = 0.017), and 15% (95% CI: 2–27; P = 0.024), respectively. There was significant heterogeneity for the survival rates at 1 year (I2 = 97.4%; P < 0.001), 2 years (I2 = 58.5%; P = 0.034), 3 years (I2 = 95.6%; P < 0.001), and 5 years (I2 = 95.0%; P < 0.001). Sensitivity analyses found the ranges for survival at 1, 2, 3, and 5 years were 52.3–67.7%, 20.2–27.4%, 15.0–28.2%, and 6.7–18.1%, respectively (Additional file 1). There was potential significant publication bias for the 1-year survival rate (Egger test P: 0.017; Begg’s test P: 0.548), but there was no significant publication bias for the 2-year (Egger test P: 0.625; Begg’s test P: 0.452), 3-year (Egger test P: 0.595; Begg’s test P: 0.806), or 5-year (Egger test P: 0.477; Begg’s test P: 0.221) survival rates (Additional file 1).

The pooled incidences of survival at 1, 2, 3, and 5 years after re-irradiation
Complete response and local re-recurrence
Three and four studies reported the effects of re-irradiation on complete response and local re-recurrence, respectively (Fig. 3). The pooled incidences of complete response and local re-recurrence after re-irradiation were 54% (95% CI: 21–88; P = 0.001) and 62% (95% CI: 55–70; P < 0.001), respectively. There was significant heterogeneity for complete response (I2 = 60.7%; P = 0.079), but no evidence of heterogeneity was observed for local re-recurrence (I2 = 0.0%; P = 0.496).

The pooled incidences of complete response and re-recurrence after re-irradiation
Overall survival and local failure-free survival
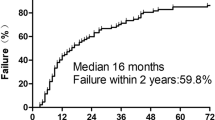
Three and three studies reported the effects of re-irradiation on overall survival and local failure-free survival, respectively (Fig. 4). The pooled overall survival and local failure-free survival after re-irradiation were 13.94 months (95% CI: 4.18–46.51; P < 0.001) and 11.01 months (95% CI: 5.99–20.22; P < 0.001), respectively. There was significant heterogeneity for overall survival (I2 = 79.4%; P = 0.008) but not for local failure-free survival (I2 = 25.4%; P = 0.262).

The pooled overall survival and local failure-free survival after re-irradiation
Grade ≥ 3 adverse events
Esophageal perforation (pooled incidence: 21%; 95% CI: 11–31; P < 0.001), tracheoesophageal fistula (pooled incidence: 30%; 95% CI: 2–58; P = 0.038), and radiation pneumonitis (pooled incidence: 4%; 95% CI: 2–6; P < 0.001) were significantly more common after re-irradiation (Fig. 5). However, re-irradiation was not associated with increased incidences of thrombocytopenia, anemia, or neutropenia. There was no significant heterogeneity for grade ≥ 3 adverse events.

The pooled grade ≥ 3 adverse events after re-irradiation
Subgroup analysis
The results of subgroup analyses for survival at 1, 2, 3, and 5 years are shown in Table 2. The 1-year survival rate after re-irradiation was higher in studies with a sample size ≥ 50, mean age ≥ 65 years, male proportion < 90%, ≥ 50% patients with tumor stage III and IV, mean interval from prior therapy to radiotherapy ≥ 24 months, and moderate quality. The 2-year survival rate after re-irradiation was higher in studies with a mean age ≥ 65 years and mean interval from prior therapy to radiotherapy ≥ 24 months. The 3-year survival rate after re-irradiation was higher in studies with a sample size ≥ 50, mean age ≥ 65 years, ≥ 50% patients with tumor stage III and IV, mean interval from prior therapy to radiotherapy ≥ 24 months, and moderate quality. The 5-year survival rate after re-irradiation was higher in studies with a sample size ≥ 50, mean age ≥ 65 years, ≥ 50% patients with tumor stage III and IV, mean interval from prior therapy to radiotherapy ≥ 24 months, and moderate quality.
Discussion
In this meta-analysis, we included nine studies assessing the effectiveness of re-irradiation in 573 ESCC patients with locoregional recurrence, and the effect estimates varied across the included studies. Although patients should be monitored for grade ≥ 3 esophageal perforation, tracheoesophageal fistula, and radiation pneumonitis in clinical practice, re-irradiation was effective for locoregional recurrent ESCC previously treated with radiotherapy. Moreover, the treatment effects of re-irradiation on survival rate were affected by sample size, mean age, male proportion, tumor stage, interval from prior therapy to radiotherapy, and study quality.
To our knowledge, this is the first meta-analysis focused on the treatment effects of re-irradiation for locoregional recurrent ESCC previously treated with radiotherapy. Several features of this study should be mentioned. First, it mainly included studies with lower quality, which restricted the representativeness of the cohort, and lower comparability, which could affect the reliability of the pooled results. Second, the heterogeneity in the survival rate at various timepoints was substantial, which could be explained by differences in tumor stage at initial diagnosis, initial treatment strategy, and radiation dose. Therefore, the results of this study should be generalized cautiously, and potential prognostic factors should be explored in further studies.
Our results on the pooled incidences of survival and recurrence after re-irradiation showed that re-irradiation is feasible. Although most studies suggested that re-irradiation could improve the survival rate at various timepoints, several studies reported a lower survival rate than expected [22, 24]. Kim et al. found an overall survival longer than 12 months in only one patient, and the mean overall survival was 6.73 months [22]. However, three patients experienced grade 5 tracheoesophageal fistula. Moreover, in the study by Katano et al., only one patient survived longer than 2 years [24]. Furthermore, two included studies found that the incidence of complete response, which was lower than expected and the pooled conclusion was variable [21, 24].
With regard to the safety of re-irradiation, our results showed that grade ≥ 3 esophageal perforation, tracheoesophageal fistula, and radiation pneumonitis were more common after re-irradiation. However, whether these adverse events were related to re-irradiation is unclear. The dose of irradiation for ESCC patients with locoregional recurrence after initial radiotherapy is important and needs further investigation [28].
Subgroup analyses showed that the survival rate after re-irradiation was affected by sample size, mean age, male proportion, tumor stage, interval from prior therapy to radiotherapy, and study quality. Interestingly, re-irradiation provided better survival outcomes for patients with high risk. There could be several reasons for these results. (1) The sample size was related to the power and weight from the overall analysis, which affected the robustness of the pooled conclusion. (2) Patient age is significantly related to disease severity and treatment tolerability. (3) The effect of radiosensitivity for ESCC patients might differ in men and women. Moreover, androgen could facilitate the growth of human ESCC cells, and the activation of androgen receptors could induce the progression of ESCC [29,30,31]. Therefore, the association of androgen levels with the prognosis of ESCC after radiotherapy needs to be further explored. (4) The baseline tumor stage before chemoradiotherapy or radiotherapy is a significant prognostic factor for ESCC [32]. (5) The interval from prior therapy to radiotherapy is significantly related to the response and progression of disease at initial treatment. (6) The quality of studies is significantly related to the reliability of the conclusions, and the representativeness of the result is stronger in studies with higher quality.
Several shortcomings of this study should be acknowledged. First, all of the included studies were retrospective, and the results could be affected by uncontrolled selection and confounder biases. Second, the analysis was based on a small number of studies, and the pooled conclusions were variable. Third, this study was based on published articles, and unpublished data were not available. Therefore, publication bias is inevitable. Finally, the analysis was based on pooled data, and whether the treatment effects of re-irradiation differ based on patients’ characteristics needs to be further evaluated.
Conclusions
In summary, this study found that re-irradiation was effective for locoregional recurrent ESCC. However, patients should be carefully monitored for grade ≥ 3 esophageal perforation, tracheoesophageal fistula, and radiation pneumonitis. Further, re-irradiation had a greater effect on survival outcomes in high-risk patients than in low-risk patients. Further prospective controlled clinical trials should be conducted to compare the efficacy and safety of re-irradiation versus non-re-irradiation for locoregional recurrent ESCC previously treated with radiotherapy.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CIs:
-
Confidence intervals
- ESCC:
-
Esophageal squamous cell carcinoma
References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–86.
Pennathur A, Gibson MK, Jobe BA, et al. Oesophageal carcinoma. Lancet. 2013;381:400–12.
Wu YF, Chu SC, Chang BS, et al. Hematologic markers as prognostic factors in nonmetastatic esophageal cancer patients under concurrent chemoradiotherapy. Biomed Res Int. 2019;2019:1263050.
Hong ZN, Weng K, Peng K, et al. Neoadjuvant immunotherapy combined chemotherapy followed by surgery versus surgery alone for locally advanced esophageal squamous cell carcinoma: a propensity score-matched study. Front Oncol. 2021;11:797426.
Ye Y, Xu Y, Fu Q, et al. Enteral nutrition support does not improve PNI in radiotherapy patients with locally advanced esophageal cancer. Nutr Cancer. 2019;71:223–9.
Welsh J, Settle SH, Amini A, et al. Failure patterns in patients with esophageal cancer treated with definitive chemoradiation. Cancer. 2012;118:2632–40.
Ghaly G, Kamel M, Nasar A, et al. Locally advanced esophageal cancer: what becomes of 5-year survivors? J Thorac Cardiovasc Surg. 2016;151:726–31.
Chen Y, Lu Y, Wang Y, et al. Comparison of salvage chemoradiation versus salvage surgery for recurrent esophageal squamous cell carcinoma after definitive radiochemotherapy or radiotherapy alone. Dis Esophagus. 2014;27:134–40.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Stang A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–5.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Ades AE, Lu G, Higgins JP. The interpretation of random-effects metaanalysis in decision models. Med Decis Mak. 2005;25:646–54.
Deeks JJ, Higgins JPT, Altman DG. Analyzing data and undertaking meta-analyses. In: Higgins J, Green S, editors. Cochrane handbook for systematic reviews of interventions 5.0.1; chapter 9. Oxford: The Cochrane Collaboration; 2008.
Higgins JPT, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Tobias A. Assessing the influence of a single study in meta-analysis. Stata Tech Bull. 1999;47:15–7.
Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ. 2003;326:219.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–101.
Shioyama Y, Nakamura K, Ohga S, et al. Radiation therapy for recurrent esophageal cancer after surgery: clinical results and prognostic factors. Jpn J Clin Oncol. 2007;37:918–23.
Nonoshita T, Sasaki T, Hirata H, et al. High-dose-rate brachytherapy for previously irradiated patients with recurrent esophageal cancer. Radiat Med. 2007;25:373–7.
Maruyama K, Motoyama S, Anbai A, et al. Therapeutic strategy for the treatment of postoperative recurrence of esophageal squamous cell carcinoma: clinical efficacy of radiotherapy. Dis Esophagus. 2011;24:166–71.
Kim YS, Lee CG, Kim KH, et al. Re-irradiation of recurrent esophageal cancer after primary definitive radiotherapy. Radiat Oncol J. 2012;30:182–8.
Zhou ZG, Zhen CJ, Bai WW, et al. Salvage radiotherapy in patients with local recurrent esophageal cancer after radical radiochemotherapy. Radiat Oncol. 2015;10:54.
Katano A, Yamashita H, Nakagawa K. Re-irradiation of locoregional esophageal cancer recurrence following definitive chemoradiotherapy: a report of 6 cases. Mol Clin Oncol. 2017;7:681–6.
Hong L, Huang YX, Zhuang QY, et al. Survival benefit of re-irradiation in esophageal cancer patients with locoregional recurrence: a propensity score-matched analysis. Radiat Oncol. 2018;13:171.
Xu X, Wang Z, Jiang S, et al. Evaluating the optimal re-irradiation dose for locally recurrent esophageal squamous cell carcinoma after definitive radiotherapy. Radiat Oncol. 2019;14:191.
Zhao K, Si Y, Sun L, et al. Efficacy and toxicity of re-irradiation for esophageal cancer patients with locoregional recurrence: a retrospective analysis. Radiat Oncol. 2020;15:243.
Zhang J, Peng F, Li N, et al. Salvage concurrent radio-chemotherapy for post-operative local recurrence of squamous-cell esophageal cancer. Radiat Oncol. 2012;7:93–100.
Matsuoka H, Sugimachi K, Ueo H, et al. Sex hormone response of a newly established squamous cell line derived from clinical esophageal carcinoma. Cancer Res. 1987;47:4134–40.
Dong H, Xu J, Li W, et al. Reciprocal androgen receptor/interleukin-6 crosstalk drives oesophageal carcinoma progression and contributes to patient prognosis. J Pathol. 2017;241:448–62.
Luo HS, Xu HY, Du ZS, et al. Impact of sex on the prognosis of patients with esophageal squamous cell cancer underwent definitive radiotherapy: a propensity score-matched analysis. Radiat Oncol. 2019;14:74.
Kondo S, Tajika M, Tanaka T, et al. Prognostic factors for salvage endoscopic resection for esophageal squamous cell carcinoma after chemoradiotherapy or radiotherapy alone. Endosc Int Open. 2016;4:E841–8.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
LK acquisition of data, analysis and interpretation of data, drafting the article, final approval; LT acquisition of data, analysis and interpretation of data, drafting the article, final approval; CH interpretation of data, revising the article, final approval; CH interpretation of data, revising the article, final approval; CH conception and design of the study, critical revision, final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Sensitivity analysis for the 1-year survival rate (52.3–67.7%). CI: confidence interval; Fig. S2. Funnel plot for the 1-year survival rate; Fig. S3. Sensitivity analysis for the 2-year survival rate (20.2–27.4%); Fig. S4. Funnel plot for the 2-year survival rate; Fig. S5. Sensitivity analysis for the 3-year survival rate (15.0–28.2%); Fig. S6. Funnel plot for the 3-year survival rate; Fig. S7. Sensitivity analysis for the 5-year survival rate (6.7–18.1%); Fig. S8. Funnel plot for the 5-year survival rate.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lan, K., Chen, J. Efficacy and safety of re-irradiation for locoregional esophageal squamous cell carcinoma recurrence after radiotherapy: a systematic review and meta-analysis. Radiat Oncol 17, 61 (2022). https://doi.org/10.1186/s13014-022-02019-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-022-02019-0