
Abstract
Background
This study aims to investigate the relationship between vitamin B1 intake and cognitive function in older adults.
Methods
This cross-sectional observational study utilized data from the National Health and Nutrition Examination Survey (NHANES) 2011–2014. A total of 2422 participants were included in the analysis, with dietary vitamin B1 intake being determined by averaging two 24-h dietary recalls. Cognitive function was assessed using three cognitive function tests: the Digit Symbol Substitution Test (DSST) for processing speed, the Animal Fluency Test (AFT) for executive function, a Consortium to Establish a Registry for Alzheimer's disease (CERAD) subtest for memory. Test-specific and global cognition z score was created. Multivariate linear regression models were used to explore the association between vitamin B1 and cognitive function.
Results
2422 participants, aged 60 years and older, were included from NHANES across two survey cycles (2011–2014). Higher vitamin B1 intake was associated with higher DSST, AFT scores (P < 0.001) as well as the global cognition z score (P = 0.008).
In the fully adjusted model, as compared to the lowest quartile (Q1), the highest quartile (Q4) of vitamin B1 intake was related to higher DSST score (β = 2.23, 95% CI 0.79 ~ 3.67) and global cognition z sore (β = 0.09, 95% CI 0.02 ~ 0.16). The association between dietary vitamin B1 intake and cognitive function scores in US adults is linear. There was no detected significant statistical interaction between these variables.
Conclusions
Increased dietary intake of vitamin B1 was associated with better cognitive function in individuals aged over 60.
Similar content being viewed by others


Introduction
The prevalence of cognitive impairment is increasing due to the aging of the global population [1]. From mild cognitive impairment (MCI) to Alzheimer's disease (AD), all forms of dementia are characterized by cognitive impairment and are becoming a major global public health concern [2]. Projections indicate that the number of people with dementia will increase from 57.4 million cases globally in 2019 to 152.8 million cases in 2050 [3]. In the United States, the number of adults over 65 with clinical AD will increase from 6.07 million in 2020 to 13.85 million in 2060 [4]. Therefore, exploring protectable factors related to cognitive performance is essential for preventing the onset of cognitive impairment [5]. Identifying risks and protective factors is an effective way of early prevention strategies. Physical activity and a healthy diet are modifiable factors associated that can reduce the risk of cognitive impairment [6,7,8]. Additionally, a nutritious diet with adequate intake of vitamins B, D, and E can have a protective effect on cognitive performance [12]. Thus, thiamine deficiency can occur at any stage of life [13]. Vitamin B1 deficiency also has been linked to various neurodegenerative disorders, including Alzheimer's disease, Parkinson's disease, and Huntington's disease [14, 15]. Nevertheless, the impact of dietary vitamin B1 intake on cognitive impairment in older adults remains uncertain. Consequently, our objective is to examine the association between dietary vitamin B1 intake and cognitive function in individuals aged 60 years and older, utilizing publicly accessible data from the National Health and Nutrition Examination Survey (NHANES) between 2011 and 2014.
Materials and methods
Data sources and study population
The cross-sectional study utilized NHANES data from 2011 to 2014, performed by the National Center for Health Statistics (NCHS). The NHANES program employs a stratified, multistage probability cluster sampling design to conduct annual surveys, ensuring the sampled population accurately represents the entire U.S. population. Through health interviews, sociodemographic information including age, gender, household income, and education level is collected, along with health-related lifestyle variables such as alcohol consumption, smoking habits, and physical activity. All procedures were approved by the NCHS Research Ethics Committee, and participants provided written informed consent. (http://www.cdc.gov/nchs/nhanes.htm).
For this analysis, we excluded subjects with incomplete cognitive information and participants with incomplete vitamin B1 intake questionnaires [11, 16, 17]. The final sample consisted of 2422 individuals aged 60 years and above. In this study, we followed the STROBE guidelines for reporting observational studies [18].
Dietary vitamin B1 intake
The NHANES study employed a 24-h food recall questionnaire that was made available to all participants, enabling the collection of comprehensive data regarding the type and quantity of food consumed within the previous 24 h. All NHANES participants were eligible to participate in two 24-h dietary recall interviews, with the data collected being utilized to ascertain the daily intake of vitamin B1 for each individual. The initial dietary recall interview was conducted face-to-face at the Mobile Examination Center (MEC), while the second interview took place via telephone within a period of 3–10 days [19]. Dietary vitamin B1 intake was assessed by averaging data from two 24-h dietary recalls. Participants were grouped based on their vitamin B1 intake.
Cognitive function
In the NHANES study, participants underwent various cognitive function tests to evaluate their memory and executive skills. The immediate and delayed verbal list learning (CERAD-IRT and CERAD-DRT) test, conducted by the Alzheimer's Disease Word Learning Registry Consortium, assesses the capacity to acquire novel linguistic [20]. The participants were required to read aloud a list of 10 unrelated terms, followed by an immediate recall of as many words as possible. Their scores from the first three tests were added. Moreover, a delayed recall test was conducted approximately 8–10 min after the commencement of the word learning trial, with a score range of 0–10.The Animal Fluency Test (AFT) measures verbal and executive abilities by asking participants to name as many animals as possible in one minute [21]. For each animal named, one point is awarded [22]. The Digit Symbol Substitution Test (DSST) is a time-constrained assessment that quantifies processing speed and executive function through the task of transcribing symbols corresponding to digits, utilizing a provided legend [23]. Participants had 2 min to match symbols to numbers in 133 boxes using keys at the top. Scores were based on correct matches, ranging from 0 to 133.
The global cognition z score calculated by averaging the four standardized scores, including DSST, AFT, CERAD-IRT, and CERAD-DRT. Standardized scores were calculated from the sample mean and standard deviation of each cognitive test score. For all the tests, higher scores indicate better cognitive performance [22, 24].
Covariates
Multiple potential covariates were evaluated based on existing literature, including gender, age, body mass index, race, marital status, education, poverty income ratio, smoking status, alcohol status, hypertension, diabetes mellitus, history of cardiovascular disease, and stroke [11, 25, 26]. The classification of race/ethnicity included non-Hispanic white, non-Hispanic black, Mexican American, and other races. Marital status was categorized as married, cohabiting, or living alone. Educational attainment was classified into three categories: less than 9 years, 9–12 years, and more than 12 years. The poverty income ratio (PIR) was utilized to classify family income into three distinct groups: low (PIR ≤ 1.3), medium (PIR > 1.3–3.5), and high (PIR > 3.5). Smoking status was classified as follows: never smokers (smoked fewer than 100 cigarettes), current smokers, and former smokers (quit smoking after consuming more than 100 cigarettes). Similarly, alcohol status was categorized as never drinking (consumed less than 12 alcoholic drinks in a lifetime), current drinking, and former drinking (consumed at least 12 drinks in a lifetime).
Statistical analysis
The characteristics of the study participants at baseline were compared using the Chi-square test and one-way analysis of variance. Continuous variables were presented as mean and standard deviation (SD) or median and interquartile range (IQR), while categorical variables were expressed as population proportions and percentages. In order to account for multiple comparisons, pairwise comparisons with Bonferroni correction were conducted.
Vitamin B1 intake was categorized by quartiles, with Q1 being the reference group. The multivariate linear regression explored vitamin B1 intake as both a continuous and categorical variable. β and 95% confidence interval (CI) were calculated to assess the relationship between vitamin B1 intake and cognitive function. Model 1 represented the crude model without any adjustment for variables. Model 2 was adjusted for age, gender, race/ethnicity, poverty income ratio, marital status, and education level. Model 3 was adjusted as for Model 2, additionally adjusted for body mass index, smoking status, alcohol status, hypertension, diabetes mellitus, cardiovascular disease history, and stroke. Linear trend tests were performed by treating categorical variables as continuous variables. We also conducted curve fitting of the dose–response relationship between vitamin B1 intake and cognitive test scores using the restricted cubic spline approach.
Subgroup analyses were conducted using hierarchical binary linear regression models, wherein continuous variables were converted into categorical variables according to clinical cutoffs or quantiles. Interaction tests were performed, followed by effect adjustment tests on subgroup measures, and likelihood ratio tests were subsequently conducted.
All analyses were performed with the statistical software packages R 4.1.1 and Free Statistics software versions 1.7.1. A two-sided p < 0.05 was considered statistically significant.
Results
Characteristics of participants at the baseline
During the 2011–2014 cycle, NHANES involved the participation of 19,931 individuals.
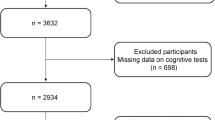
We excluded individuals under the age of 60 (n = 16,299), those with missing dietary data on vitamin B1 (n = 564), those with missing cognitive data (n = 355), and those with missing covariates (n = 291). As a result, a final sample of 2,422 participants was included in the study. Figure 1 illustrates the selection process in detail.

Flowchart detailing the selection process for patients included in this retrospective analysis
The baseline characteristics of the study participants based on their dietary vitamin B1 intake were summarized in Table 1. Quartile analysis of vitamin B1 was conducted to categorize the participants into four groups: Q1 (≤ 0.97 mg/day), Q2 (0.98 mg/day–1.33 mg/day), Q3 (1.34 mg/day–1.82 mg/day), and Q4 (> 1.82 mg/day). The mean age of the participants was 69.3 ± 6.7 years, with 1232 (50.9%) females and 1214 (50.1%) Non-Hispanic Whites. Moreover, in comparison to individuals with low vitamin B1 intake, those with higher vitamin B1 intake exhibited a greater likelihood of being Non-Hispanic White and male, as well as possessing higher family income, and lower rates of smoking. Additionally, these individuals demonstrated higher scores on the DSST, AFT, and global z score, with respective averages of 48.3 ± 15.7, 17.6 ± 5.7, and 0.10 (−0.44, 0.57) in the highest vitamin B1 intake.
Relationship between dietary vitamin B1 intake and cognitive function
Table 2 presents the findings of multivariable linear regression analysis on the association between vitamin B1 consumption and cognitive function. Our research indicated that vitamin B1 intake was positively associated with cognitive scores. In the crude model, participants in the highest quartile (Q4) groups exhibited higher cognition scores(DSST:β = 4.40, 95% CI 2.50 ~ 6.31; AFT:β = 1.48, 95% CI 0.86 ~ 2.10; Z score:β = 0.16, 95% CI 0.07 ~ 0.25) compared to the Q1 group. Moreover, as vitamin B1 intake increased, cognitive scores gradually increased (p for trend < 0.001). These associations remained statistically significant across all multivariate linear regression models, even after controlling for various covariates such as age, gender, race/ethnicity, poverty income ratio, marital status, education level, body mass index, smoking status, alcohol status, hypertension, and diabetes mellitus, cardiovascular disease history, and stroke. In the model 3, compared with Q1, participants in Q4 groups were found with higher DSST score (β = 2.23, 95% CI 0.79 ~ 3.67) and global z score (β = 0.09, 95% CI 0.02 ~ 0.16). The Q2 and Q3 groups also exhibited significantly higher DSST scores (p for trend 0.003), AFT scores (p for trend 0.048), and global z scores (p for trend 0.004) than the Q1 group. The relationship between covariates and cognitive function is shown in Additional file 1: Table S1.
Dose–response relationships
After fully adjusting, vitamin B1 and cognitive function scores showed a dose–response relationship. In restricted cubic spline models, vitamin B1 was positively associated with each of the cognitive scores in a linear manner (Fig. 2).

Association between dietary vitamin B1 intake and cognitive performance in DSST, AFT, CERAD-IRT, CERAD-DRT and z score. Solid and dashed lines represent the predicted value and 95% confidence intervals. Adjusted for age, gender, race/ethnicity, poverty income ratio, marital status, education level, body mass index, smoking status, alcohol status, hypertension, diabetes mellitus, cardiovascular disease history and stroke. Only 99% of the data is shown
Subgroup analysis
In addition, the study examined possible moderators of the association between cognitive performance and dietary vitamin B1 intake of cognitive scores, including gender (male vs. female), age (60–70 vs. > 80), BMI (< 25 vs. 25–30 vs. > 30 kg/m2), hypertension (yes vs. no), diabetes mellitus (yes vs. no), cardiovascular disease history (yes vs. no) and stroke (yes vs. no). The results of the subgroup analysis for the association between dietary vitamin B1 intake and cognitive function are shown in Additional file 2: Table S2. High intake of vitamin B1 was associated with higher global z score, if the participants were without diabetes (β = 0.09, 95% CI 0.01 ~ 0.17; p for interaction = 0.014), and coronary heart disease (β = 0.09, 95% CI 0.02 ~ 0.17; p for interaction = 0.007). Compared with Q1, participants in Q4 groups were found to have a higher globe z score (β = 0.08, 95%CI −0.02 ~ 0.18; p for trend = 0.045) and DSST score (β = 2.4, 95% CI 0.42 ~ 4.38; p for trend = 0.011) in the subgroup of hypertension. No significant interactions were found between dietary vitamin B1 intake and participant characteristics or other disease states (Fig. 3).

Stratified analyses of the association between cognitive performance and dietary vitamin B1 intake according to baseline characteristics in z score test. The P value for interaction represents the likelihood of interaction between the variable and vitamin B1. CI confidence interval
Discussion
This study examined data obtained from a cross-sectional study conducted from 2011 to 2014, specifically targeting the older adult population. Vitamin B1 intake was associated with better cognitive scores in this study using multivariate-adjusted linear regression analysis, which remained significant after adjusting for all potential confounders. Moreover, we observed a dose-dependent association between dietary vitamin B1 consumption and low cognitive performance in US adults (global z score, P for nonlinearity = 0.457).
Several studies have also investigated the relationship between B vitamins and cognition [25, 27, 28]. A meta-analysis has indicated that B vitamin supplementation was associated with decelerating cognitive decline, particularly in populations who have received early and long-term intervention. Additionally, increased dietary folate intake has been associated with a reduced risk of dementia in people without cognitive impairment [12]. Deficiencies of vitamin B1 can result in heart failure and serious neurologic disorders such as paralysis, ataxia, confusion, and delirium [13, 33, 34]. According to Pourhassan et al., the mean level of thiamine in the blood of patients with delirium was significantly lower than that of controls (p = 0.002) [35]. The research conducted by La Rue et al. also revealed a positive association between the consumption of thiamine in one's diet and abstract reasoning abilities [32]. Our study similarly found the protective effect of vitamin B1 on cognitive function. As dietary vitamin B1 intake increased, cognitive scores (including DSST, AFT, and Z score) increased accordingly (p < 0.001).
Although the mechanism of association between vitamin B1 intake and cognitive decline is unclear, we believe our findings are biologically plausible. Previous studies have demonstrated that thiamine deficiency elicits anorexia through the inhibition of the hypothalamic adenosine monophosphate-activated protein kinase signal pathway and disruption of neuroendocrine feedback control over food intake and energy metabolism, which may be related to malnutrition and insufficient thiamine intake in AD patients [36, 37]. Ramamoorthy et al. pointed out the role of neuroinflammation in the dysfunction of thiamin transporters (mediated via transcriptional mechanisms) and suggested optimizing thiamin levels in the brain of AD patients [37]. Vitamin B1 deficiency leads to reduced activity of acetylcholine synthase choline acetyltransferase, and neurogenesis, inducing excessive glutamate release and selective death of the subthalamic midline nucleus, which is involved in brain inflammation and oxidative stress [14].
In this study, we used a multidimensional, comprehensive approach to assess cognitive function, including the CERAD-DRT, CERAD-IRT, DSST, AFT, and z score [38]. Furthermore, confounding variables were adjusted by previous studies and conducting thorough analyses. Additionally, a dose–response analysis was conducted to investigate the potential relationship between vitamin B1 intake and cognitive function. In spite of that, there were several limitations in our study. Firstly, due to the cross-sectional nature of this study, we could not determine the temporal association between vitamin B1 and cognitive function. Additional randomized controlled studies are needed to confirm the findings. Secondly, despite comprehensive adjustments for potential covariates, the presence of reverse causality and residual confounding cannot be entirely ruled out. Certain covariates may possess new indicators that were not considered in this study. Thirdly, as the dietary data for vitamin B1 were collected from self-reported 24-h diet reviews, there might be some measurement and recall errors. Finally, additional research is required to determine whether the current findings can be extrapolated to other populations based on this study of U.S. adults.
Conclusions
In conclusion, among a representative national sample of US adults, vitamin B1 intake was associated with cognitive performance. Our findings may provide support for further largescale prospective studies to elucidate the exact causality of this relationship.
Availability of data and materials
Publicly available datasets are available online for this study. The repository/repositories name and accession numbers are available online at http://www.cdc.gov/ nchs/nhanes.htm (accessed on 1 March 2022). Dietary data can be obtained from 2011–2012 Dietary Data—Continuous NHANES (cdc.gov) and 2013–2014 Dietary Data—Continuous NHANES (cdc.gov).
Abbreviations
- NHANES:
-
National Health and Nutrition Examination Survey
- NCHS:
-
National Center for Health Statistics
- MEC:
-
Mobile Examination Center
- DSST:
-
Digit Symbol Substitution Test
- AFT:
-
Animal Fluency Test
- CERAD:
-
Consortium to Establish a Registry for Alzheimer's disease
- CERAD-IRT:
-
Immediate verbal list learning
- CERAD-DRT:
-
Delayed verbal list learning
- MCI:
-
Mild cognitive impairment
- AD:
-
Alzheimer's disease
- PIR:
-
Poverty income ratio
- Q:
-
Quartile
- SD:
-
Standard deviation
- IQR:
-
Median and interquartile range
- CI:
-
Confidence intervals
References
Chapman S, Rentería MA, Dworkin JD, Garriga SM, Barker MS, Avila-Rieger J, et al. Association of subjective cognitive decline with progression to dementia in a cognitively unimpaired multiracial community sample. Neurology. 2023;100:e1020–7.
Ghahremani M, Nathan S, Smith EE, McGirr A, Goodyear B, Ismail Z. Functional connectivity and mild behavioral impairment in dementia-free elderly. Alzheimers Dement (N Y). 2023;9:e12371.
GBD. 2019 Dementia forecasting collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7:e105-25.
Rajan KB, Weuve J, Barnes LL, McAninch EA, Wilson RS, Evans DA. Population estimate of people with clinical Alzheimer’s disease and mild cognitive impairment in the United States (2020–2060). Alzheimers Dement. 2021;17:1966–75.
Zhang X-X, Tian Y, Wang Z-T, Ma Y-H, Tan L, Yu J-T. The epidemiology of Alzheimer’s disease modifiable risk factors and prevention. J Prev Alzheimers Dis. 2021;8:313–21.
Grasset L, Proust-Lima C, Mangin J-F, Habert M-O, Dubois B, Paquet C, et al. Explaining the association between social and lifestyle factors and cognitive functions: a pathway analysis in the Memento cohort. Alzheimers Res Ther. 2022;14:68.
Ye KX, Sun L, Wang L, Khoo ALY, Lim KX, Lu G, et al. The role of lifestyle factors in cognitive health and dementia in oldest-old: a systematic review. Neurosci Biobehav Rev. 2023;152:105286.
Stefaniak O, Dobrzyńska M, Drzymała-Czyż S, Przysławski J. Diet in the prevention of Alzheimer’s disease: current knowledge and future research requirements. Nutrients. 2022;14:4564.
Wang Z, Zhu W, **ng Y, Jia J, Tang Y. B vitamins and prevention of cognitive decline and incident dementia: a systematic review and meta-analysis. Nutr Rev. 2022;80:931–49.
Ma J-H, Huang N-H, Huang T, Mu D-L. 25-hydroxyvitamin D concentrations and risk of incident dementia, mild cognitive impairment, and delirium in 443,427 UK Biobank participants. Psychiatry Res. 2023;327:115369.
Zhang K, Li B, Gu Z, Hou Z, Liu T, Zhao J, et al. Association between dietary folate intake and cognitive impairment in older US adults: National Health and Nutrition Examination Survey. Arch Gerontol Geriat. 2023;109:104946.
Strandler HS, Strand TA. Thiamin (Vitamin B1)—a sco** review for Nordic nutrition recommendations 2023. Food Nutr Res. 2023. https://doi.org/10.29219/fnr.v67.10290.
Mrowicka M, Mrowicki J, Dragan G, Majsterek I. The importance of thiamine (vitamin B1) in humans. 2023. Biosci Rep. https://doi.org/10.1042/BSR20230374.
Gibson GE, Hirsch JA, Fonzetti P, Jordan BD, Cirio RT, Elder J. Vitamin B1 (thiamine) and dementia. Ann Ny Acad Sci. 2016;1367:21–30.
Whitfield KC, Bourassa MW, Adamolekun B, Bergeron G, Bettendorff L, Brown KH, et al. Thiamine deficiency disorders: diagnosis, prevalence, and a roadmap for global control programs. Ann N Y Acad Sci. 2018;1430:3–43.
Song L, Li H, Fu X, Cen M, Wu J. Association of the oxidative balance score and cognitive function and the mediating role of oxidative stress: evidence from the National Health and Nutrition Examination Survey (NHANES) 2011–2014. J Nutr. 2023;153:1974–83.
Sun X, Yu W, Wang M, Hu J, Li Y. Association between rest-activity rhythm and cognitive function in the elderly: The U.S. National Health and Nutrition Examination Survey, 2011–2014. Front Endocrinol. 2023;14:1135085.
Ghaferi AA, Schwartz TA, Pawlik TM. STROBE reporting guidelines for observational studies. JAMA Surg. 2021;156:577–8.
Wen H, Niu X, Zhao R, Wang Q, Sun N, Ma L, et al. Association of vitamin B1 with cardiovascular diseases, all-cause and cardiovascular mortality in US adults. Front Nutr. 2023;10:1175961.
Lu Z, Chen C, Zhang J, Wang X, Zhang D, Li S. The relationship between alternative healthy diet index and cognitive function in the older adults: the mediating effect of depressive symptoms. Nutrients. 2022;14:2856.
Long LS, Wolpaw JT, Leung JM. Sensitivity and specificity of the animal fluency test for predicting postoperative delirium. Can J Anaesth. 2015;62:603–8.
Wei J, Wang L, Kulshreshtha A, Xu H. Adherence to life’s simple 7 and cognitive function among older adults: the national health and nutrition examination survey 2011 to 2014. J Am Heart Assoc. 2022;11:e022959.
Jaeger J. Digit symbol substitution test: the case for sensitivity over specificity in neuropsychological testing. J Clin Psychopharmacol. 2018;38:513–9.
Tang H, Zhang X, Luo N, Huang J, Zhu Y. Association of dietary live microbes and non-dietary prebiotic/probiotic intake with cognitive function in older adults: evidence from NHANES. J Gerontol A Biol Sci Med Sci. 2023. https://doi.org/10.1093/gerona/glad175.
Zhou L. Association of vitamin B2 intake with cognitive performance in older adults: a cross-sectional study. J Transl Med. 2023;21:870.
Zhong Q, Sun W, Qin Y, Xu H. Association of dietary α-carotene and β-carotene intake with low cognitive performance in older adults: a cross-sectional study from the national health and nutrition examination survey. Nutrients. 2023;15:239.
Samson ME, Yeung LF, Rose CE, Qi YP, Taylor CA, Crider KS. Vitamin B-12 malabsorption and renal function are critical considerations in studies of folate and vitamin B-12 interactions in cognitive performance: NHANES 2011–2014. Am J Clin Nutr. 2022;116:74–85.
Xu H, Wang S, Gao F, Li C. Vitamin B6, B9, and B12 intakes and cognitive performance in elders: National Health and Nutrition Examination Survey, 2011–2014. Neuropsych Dis Treat. 2022;18:537–53.
Hughes CF, Ward M, Tracey F, Hoey L, Molloy AM, Pentieva K, et al. B-vitamin intake and biomarker status in relation to cognitive decline in healthy older adults in a 4-Year follow-up study. Nutrients. 2017;9:53.
Qian T, Zhao L, Pan X, Sang S, Xu Y, Wang C, et al. Association between blood biochemical factors contributing to cognitive decline and b vitamins in patients with Alzheimer’s disease. Front Nutr. 2022;9:823573.
Sheng L-T, Jiang Y-W, Pan X-F, Feng L, Yuan J-M, Pan A, et al. Association between dietary intakes of b vitamins in midlife and cognitive impairment in late-life: the Singapore Chinese Health study. J Gerontol A Biol Sci Med Sci. 2020;75:1222–7.
Sang S, Pan X, Chen Z, Zeng F, Pan S, Liu H, et al. Thiamine diphosphate reduction strongly correlates with brain glucose hypometabolism in Alzheimer’s disease, whereas amyloid deposition does not. Alzheimers Res Ther. 2018;10:26.
Chen Z-R, Huang J-B, Yang S-L, Hong F-F. Role of cholinergic signaling in Alzheimer’s disease. Molecules. 2022;27:1816.
Ceolin C, Papa MV, De Rui M, Devita M, Sergi G, Coin A. Micronutrient deficiency and its potential role in delirium onset in older adults: a systematic review. J Nutr Health Aging. 2023;27:785–90.
Pourhassan M, Angersbach B, Lueg G, Klimek CN, Wirth R. Blood thiamine level and cognitive function in older hospitalized patients. J Geriatr Psychiatry Neurol. 2019;32:90–6.
Marseglia A, Darin-Mattsson A, Skoog J, Rydén L, Hadarsson-Bodin T, Kern S, et al. Metabolic syndrome is associated with poor cognition: a population-based study of 70-year-old adults without dementia. J Gerontol A Biol Sci Med Sci. 2021;76:2275–83.
Ramamoorthy K, Yoshimura R, Al-Juburi S, Anandam KY, Kapadia R, Alachkar A, et al. Alzheimer’s disease is associated with disruption in thiamin transport physiology: a potential role for neuroinflammation. Neurobiol Dis. 2022;171:105799.
Shi Y, Wang H, Zhu Z, Ye Q, Lin F, Cai G. Association between exposure to phenols and parabens and cognitive function in older adults in the United States: a cross-sectional study. Sci Total Environ. 2023;858:160129.
Acknowledgements
Thank the Fourth Hospital of Hebei Medical University for their assistance with manuscript submission.
Author information
Authors and Affiliations
Contributions
Conceived and designed, WAJ and HMW; formal analysis, WAJ and FFY; methodology, WAJ and JPS; writing—original draft, WAJ and HMW; writing—review and editing, CL and HQJ. All authors contributed to the article and approved the submitted version the study.
Corresponding author
Ethics declarations
Consent for publication
The authors have no ethical, legal, and financial conflicts related to the article. All authors read and approved the manuscript for publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Association of covariates and cognitive function.
Additional file 2: Table S2.
Association between Dietary Vitamin B1 and Cognitive Function among Different Subgroups.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jia, W., Wang, H., Li, C. et al. Association between dietary vitamin B1 intake and cognitive function among older adults: a cross-sectional study. J Transl Med 22, 165 (2024). https://doi.org/10.1186/s12967-024-04969-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-024-04969-3