
Abstract
Background
Insulin resistance is a pivotal risk factor for cardiovascular diseases, and the triglyceride-glucose (TyG) index is a well-established surrogate of insulin resistance. This study aimed to investigate the prognostic value of the TyG index and its ability in therapy guidance in patients with three-vessel disease (TVD).
Methods
A total of 8862 patients with TVD with available baseline TyG index data were included in the study. The endpoint was major adverse cardiac events (MACE). All patients received coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), or medical therapy (MT) alone reasonably.
Results
An elevated TyG index was defined as the TyG index greater than 9.51. During a median follow-up of 7.5 years, an elevated TyG index was significantly associated with an increased risk of MACE (adjusted hazard ratio 1.161, 95% confidence interval 1.026–1.314, p = 0.018). The elevated TyG index was shown to have a more pronounced predictive value for MACE in patients with diabetes, but failed to predict MACE among those without diabetes, whether they presented with stable angina pectoris (SAP) or acute coronary syndrome (ACS). Meanwhile, the association between an elevated TyG index and MACE was also found in patients with left main involvement. Notably, CABG conferred a significant survival advantage over PCI in patients with a normal TyG index, but was not observed to be superior to PCI in patients with an elevated TyG index unless the patients had both ACS and diabetes. In addition, the benefit was shown to be similar between MT and revascularisation among patients with SAP and an elevated TyG index.
Conclusions
The TyG index is a potential indicator for risk stratification and therapeutic decision-making in patients with TVD.
Graphical Abstract

Similar content being viewed by others


Introduction
Coronary artery disease (CAD) is the most common form of heart disease and remains the leading cause of death [1]. Three-vessel disease (TVD) is an extreme form of CAD that impacts the blood supply of the left anterior descending, left circumflex, and right coronary arteries and is estimated to occur in 30% of all patients with CAD [2]. Patients with TVD have a substantial risk of adverse events [3]. Therefore, timely identification of patients at high risk is essential to improve their prognosis and guide therapy.
Insulin resistance refers to a pathological state in which insulin-sensitive organs become resistant to insulin and reflects disruption of metabolic homeostasis [4, 5]. Insulin resistance is not only the core defect in type 2 diabetes but also one of the most important factors exacerbating vascular lesions in patients with CAD [6]. However, the classical methods used for measurement of insulin resistance (i.e., euglycemic insulin clamp and intravenous glucose tolerance testing) cannot be widely applied in the clinical setting owing to their high cost and invasiveness [7].
An emerging indicator known as the triglyceride-glucose (TyG) index, which is developed from triglycerides and glucose, is a simple and reliable surrogate for insulin resistance and has been shown to perform better than the homeostasis model assessment of insulin resistance [8, 9]. Previous studies have demonstrated the predictive value of the TyG index in patients with stable CAD [10, 11], those with acute coronary syndrome [12,13,14,15], and those with myocardial infarction and nonobstructive coronary arteries [16] but not in patients with TVD. A recent study found that an elevated TyG index was associated with a higher risk of multi-vessel involvement in CAD [17], suggesting a distinct role of the TyG index in TVD.
The aim of this study was to investigate the prognostic value of the TyG index and its interaction with the treatment strategy in a large cohort of patients with TVD.
Methods
Design
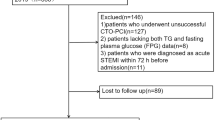
A total of 8943 consecutive patients with TVD were prospectively enrolled at Fuwai Hospital, Chinese Academy of Medical Sciences in Bei**g, China, between 2004 and 2011. TVD was defined as angiographically confirmed stenosis of ≥ 50% in all three main epicardial coronary arteries (left anterior descending, left circumflex, and right coronary) with or without involvement of the left main artery. Finally, 8862 patients with available triglyceride and fasting plasma glucose measurements were included in the study. The flowchart of this study is shown in Fig. 1.

Flowchart of this study. MACE, major adverse cardiac events; TVD, three-vessel disease; TyG index, triglyceride-glucose index
All patients underwent a detailed clinical examination and received coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), or medical therapy (MT) alone according to current practice guidelines, the judgement of the heart team, and patient preferences. Patients were followed up annually until 2016 by telephone interview, follow-up letter, or clinic visit. Investigators underwent training and a blinded questionnaire was completed to obtain high-quality data.
The study was approved by the Ethics Committee of Fuwai Hospital and performed in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all study participants.
Measurement and calculation of TyG index
Fasting blood samples were collected from the enrolled patients within 24 h after admission. Fasting plasma glucose and triglyceride concentrations were measured using standard biochemical techniques in the core laboratory at Fuwai Hospital. The TyG index was calculated as follows: ln (triglycerides [mg/dL] × fasting plasma glucose [mg/dL]/2).
Determination of the cut point for the TyG index
The cut point for the TyG index was calculated using the “surv_cutpoint” function (survminer package, Version 0.4.9 in R). The TyG value that corresponded to the most significant relation (the maximal log-rank statistic) with the primary endpoint was thought to be the optimal cut point (Additional file 1: Fig. S1).
Study endpoint
The endpoint of this study was major adverse cardiac events (MACE), which is a composite of cardiac death, myocardial infarction, stroke, and urgent revascularisation.
Statistical analysis
Continuous data are shown as the mean ± standard deviation or as the median [interquartile range (IQR)]. Categorical variables are summarised as the percentage. The Student’s t-test was used to compare continuous variables between groups, and the chi-squared test was used to compare categorical variables. The statistical analysis was performed using R Version 4.0.2 (R Core Team, Vienna, Austria). A two-sided p-value of < 0.05 was considered statistically significant.
Survival curves were conducted by Kaplan–Meier method and compared using the log-rank test. Cox proportional hazard regression models were used to evaluate the associations between the TyG index and outcomes with calculation of hazard ratio (HRs) and 95% confidence interval (CIs). The multivariable Cox models were adjusted for age, sex, body mass index, previous myocardial infarction, family history of CAD, previous stroke, hypertension, diabetes, hyperlipidaemia, chronic obstructive pulmonary disease, peripheral artery disease, chronic kidney disease, smoking, clinical presentation (acute coronary syndrome [ACS] or stable angina pectoris [SAP]), left ventricular ejection fraction, creatinine clearance, left main involvement, SYNTAX score, and treatment strategy (CABG, PCI, or MT).
Data and resource availability
The dataset analyzed in the current study are available from the corresponding author upon reasonable request.
Results
Patient characteristics at baseline
The mean age of the 8862 study participants was 61.0 ± 10.0 years, and 79.7% were men. The optimal cut point for the TyG index in patients with TVD was identified to be 9.51 (see Methods and Additional file 1: Fig. S1). Levels above this cutoff value were considered elevated. As shown in Table 1, an elevated TyG index was observed in 1190 (13.4%) of all patients and found to be associated with younger age, female sex, and a higher body mass index. The incidence of comorbidities, including diabetes, hypertension, hyperlipidaemia, and chronic kidney disease, was higher in patients with an elevated TyG index than in those with a normal TyG index. Furthermore, patients with an elevated TyG index were more prone to ACS and more likely to have a family history of CAD.
Associations between TyG index and outcomes
The median follow-up duration was 7.5 years [IQR 5.9, 9.1]. During follow-up, 2222 patients (25.1%) experienced MACE.
Kaplan–Meier analysis showed that an elevated TyG index was associated with a higher incidence of MACE (p = 0.002, log-rank test) (Fig. 2). Univariable and multivariable Cox analyses showed that an elevated TyG index was significantly associated with an increased risk of MACE (crude HR 1.200, 95% CI 1.067–1.350, p = 0.002; adjusted HR 1.161, 95% CI 1.026–1.314, p = 0.018) (Fig. 2 and Additional file 2: Table S1). Further analysis indicated that there was an additional predictive value of the TyG index over diabetes (Additional file 3: Table S2).

Survival curves for MACE according to TyG index in TVD patients. HR, hazard ratio; TVD, three-vessel disease; TyG index, triglyceride-glucose index
The prognostic impact of the TyG index varies in patients with different disease phenotypes (Additional file 4: Table S3). A subgroup analysis was performed according to the clinical presentations (SAP or ACS) and the presence or absence of diabetes. The results showed that an elevated TyG index increased the risk of MACE only in diabetic patients rather than non-diabetic patients, whether they presented with SAP or ACS. Additionally, the association between an elevated TyG index and MACE was also found in patients with TVD plus left main involvement.
Interaction between the TyG index and the treatment strategy
In this cohort, 2676 (30.2%), 3789 (42.8%), and 2397 (27.0%) patients received CABG, PCI, or MT alone, respectively. To assess the impact of the TyG index on the choice of treatment strategy selection for patients with TVD, we compared the benefits of three treatment strategies in different disease phenotypes with different levels of the TyG index (Table 2 and Fig. 3).

The benefit of three treatment strategies in TVD patients with different disease phenotypes and different levels of the TyG index. A > B means that A showed a significant advantage over B; A = B means that the benefit was similar between A and B. ACS, acute coronary syndrome; CABG, coronary artery bypass grafting; MACE, major adverse cardiac events; MT, medical therapy; PCI, percutaneous coronary intervention; SAP, stable angina pectoris; TVD, three-vessel disease; TyG index, triglyceride-glucose index
In the group of patients with SAP and a normal TyG index, the risk of MACE after PCI and MT was comparable, and CABG was associated with a lower risk of MACE than PCI and MT; while among patients with SAP and an elevated TyG index, the risk of MACE was similar among three treatment strategies. These findings were regardless of the presence or absence of diabetes.
In the group of patients with ACS and a normal TyG index, both revascularisation strategies were at much lower risk of MACE than MT, and CABG was further associated with a lower risk of MACE than PCI, regardless of the presence or absence of diabetes. When the TyG index was elevated in patients with ACS, the risk of MACE after CABG was similar to that after PCI in those without diabetes; while CABG was shown to be associated with a lower risk of MACE than PCI in those with diabetes.
Moreover, in the group of patients with left main involvement, the risk of MACE was significantly lower after CABG than after PCI among patients with a normal TyG index; while among patients with an elevated TyG index, the risk of MACE after CABG was similar to that after PCI.
In summary, when comparing two revascularisation strategies, patients with a normal TyG index had a greater benefit from CABG than PCI; whereas in the presence of an elevated TyG index, the risk of MACE after CABG and PCI were similar, unless the patients had both ACS and diabetes. MT showed a similar benefit as revascularisation among patients with SAP and an elevated TyG index.
Discussion
In this large cohort of patients with TVD, we showed a significant association of an elevated TyG index with an increased risk of MACE. For distinct phenotype groups, an elevated TyG index had a predictive role for MACE in patients with diabetes and not in those without diabetes, regardless of the clinical presentations (SAP or ACS); the predictive role of the TyG index was also observed in patients with TVD plus left main involvement. CABG afforded a significant advantage over PCI and MT in terms of MACE among patients with a normal TyG index. However, CABG was not observed to be superior to PCI in patients with an elevated TyG index unless the patients had both ACS and diabetes. In addition, the benefit was shown to be similar between MT and revascularisation among patients with SAP and an elevated TyG index.
Insulin resistance can promote both atherogenesis and progression of plaque, thus correlates well with an increased risk of atherothrombotic cardiovascular disease [18, 19]. As a reliable indicator of insulin resistance, the TyG index has been demonstrated by many studies to have a positive relationship with the incidence of CAD [20, 21]. An elevated TyG index indicates severe systemic disruption of lipid metabolism and glucose, which is associated with impairment of coronary endothelial and smooth muscle cells as well as escalation of the risk of CAD [22]. More importantly, the TyG index has been identified to have a prognostic role in several types of CAD, including stable CAD [10, 11], acute coronary syndrome [12,13,14,15], and myocardial infarction with nonobstructive coronary arteries [16]. However, the prognostic usefulness of the TyG index remains unclear in patients with TVD. In the present study, we found that the TyG index had fair prognostic ability in patients with this complex and severe type of CAD.
Diabetes is one of the most significant risk factors for CAD, and insulin resistance promotes development of type 2 diabetes [23]. Based on the high degree of causality between insulin resistance and diabetes, we performed a subgroup analysis according to the presence of concomitant diabetes in patients with TVD and found that an elevated TyG index was associated with an increased risk of MACE in the diabetic subgroup but not in the non-diabetic subgroup, whether the patients presented SAP or ACS. This result might be explained by the overall low insulin resistance in patients without diabetes and is consistent with previous studies showing that the TyG index has a stronger predictive value in patients with CAD and diabetes than in their non-diabetic counterparts [11, 13, 15, 16, 24]. Moreover, an elevated TyG index also conferred valid predictive value on patients with left main involvement that represents a subgroup at a high risk.
The current guidelines recommend CABG as the preferred treatment strategy for multivessel CAD owing to its advantages in management of complex lesions and less need for repeat revascularisation [25, 26] However, our results suggested that the benefit of three treatment strategies (CABG, PCI, and MT) was closely related to the levels of TyG index and disease phenotypes in patients with TVD. We found that CABG was the optimal treatment strategy among patients with a normal TyG index, regardless of the clinical presentations, the presence or absence of diabetes, and left main involvement; while the survival benefit of CABG over PCI disappeared when patients had an elevated TyG index. This may be because the risk of symptomatic graft failure after CABG is higher in patients with an elevated TyG index than in those with a normal TyG index [27], which worsens both short-term and long-term outcomes [28]. Another interpretation of this result is that perioperative and postoperative stress responses deteriorate the impairment of insulin signaling in patients with insulin resistance, who already have severe metabolic syndrome [29, 30]. It should be noted that CABG remained the optimal choice once TVD patients with an elevated TyG index had both ACS and diabetes. This was probably because PCI and MT were hard to manage the extremely severe in situ vascular injury in such patients, and only the revascularisation on relatively healthy grafts could improve the prognosis [31]. In addition, another important finding of our study was the comparable prognosis between MT and revascularization among patients with SAP and an elevated TyG index, suggesting that revascularization might not be superior to MT alone in such patients.
In conclusion, we have demonstrated that an elevated TyG index is a strong risk factor for a poor prognosis in patients with TVD, especially those with comorbid diabetes. Moreover, we found that CABG is the preferred treatment in patients with TVD and a normal TyG index because of the lower risk of MACE in comparison with PCI and MT, as recommended in the guidelines. However, the optimal treatment strategy in patients with TVD and an elevated TyG index should be re-evaluated unless they have both ACS and diabetes.
This study has some limitations. First, its participants were recruited from a single centre, which might limit the generalisability of its findings. Second, the study had an observational design, which means that the possibility of several types of bias cannot be excluded, even after strict adjustment for confounders. Therefore, our findings require confirmation in randomised controlled clinical trials in the future. Third, the validity of the TyG index on admission is limited in the acute phase of ACS, because it might not represent the real degree of insulin resistance in the stable phase and during the follow-up. Further analysis of the trajectory of the TyG index might help to address this point.
Availability of data and materials
The datasets used/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACS:
-
Acute coronary syndrome
- CABG:
-
Coronary artery bypass grafting
- CAD:
-
Coronary artery disease
- CI:
-
Confidence interval
- IQR:
-
Interquartile range
- MACE:
-
Major adverse cardiac events
- MT:
-
Medical therapy
- HR:
-
Hazard ratio
- PCI:
-
Percutaneous coronary intervention
- SAP:
-
Stable angina pectoris
- TVD:
-
Three-vessel disease
- TyG index:
-
Triglyceride-glucose index
References
Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Beaton AZ, Boehme AK, Buxton AE, et al. Heart disease and stroke statistics-2023 update: a report from the American heart association. Circulation. 2023;147(8):e93–621.
Bradley SM, Spertus JA, Kennedy KF, Nallamothu BK, Chan PS, Patel MR, Bryson CL, Malenka DJ, Rumsfeld JS. Patient selection for diagnostic coronary angiography and hospital-level percutaneous coronary intervention appropriateness: insights from the National Cardiovascular Data Registry. JAMA Intern Med. 2014;174(10):1630–9.
Min JK, Dunning A, Lin FY, Achenbach S, Al-Mallah M, Budoff MJ, Cademartiri F, Callister TQ, Chang HJ, Cheng V, et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: an International Multicenter Registry) of 23,854 patients without known coronary artery disease. J Am Coll Cardiol. 2011;58(8):849–60.
Defronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773–95.
Hill MA, Yang Y, Zhang L, Sun Z, Jia G, Parrish AR, Sowers JR. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metab Clin Exp. 2021;119:154766.
DeFronzo RA. Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis: the missing links. The Claude Bernard Lecture 2009. Diabetologia. 2010;53(7):1270–87.
Minh HV, Tien HA, Sinh CT, Thang DC, Chen CH, Tay JC, Siddique S, Wang TD, Sogunuru GP, Chia YC, et al. Assessment of preferred methods to measure insulin resistance in Asian patients with hypertension. J Clin Hypertens (Greenwich). 2021;23(3):529–37.
Vasques AC, Novaes FS, de Oliveira MS, Souza JR, Yamanaka A, Pareja JC, Tambascia MA, Saad MJ, Geloneze B. TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes Res Clin Pract. 2011;93(3):e98–100.
Lee SH, Kwon HS, Park YM, Ha HS, Jeong SH, Yang HK, Lee JH, Yim HW, Kang MI, Lee WC, et al. Predicting the development of diabetes using the product of triglycerides and glucose: the Chungju Metabolic Disease Cohort (CMC) study. PLoS ONE. 2014;9(2): e90430.
** JL, Sun D, Cao YX, Guo YL, Wu NQ, Zhu CG, Gao Y, Dong QT, Zhang HW, Liu G, et al. Triglyceride glucose and haemoglobin glycation index for predicting outcomes in diabetes patients with new-onset, stable coronary artery disease: a nested case-control study. Ann Med. 2018;50(7):576–86.
** JL, Cao YX, Wu LG, You XD, Guo YL, Wu NQ, Zhu CG, Gao Y, Dong QT, Zhang HW, et al. Triglyceride glucose index for predicting cardiovascular outcomes in patients with coronary artery disease. J Thorac Dis. 2018;10(11):6137–46.
Wang L, Cong HL, Zhang JX, Hu YC, Wei A, Zhang YY, Yang H, Ren LB, Qi W, Li WY, et al. Triglyceride-glucose index predicts adverse cardiovascular events in patients with diabetes and acute coronary syndrome. Cardiovasc Diabetol. 2020;19(1):80.
Luo E, Wang D, Yan G, Qiao Y, Liu B, Hou J, Tang C. High triglyceride-glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc Diabetol. 2019;18(1):150.
Mao Q, Zhou D, Li Y, Wang Y, Xu SC, Zhao XH. The triglyceride-glucose index predicts coronary artery disease severity and cardiovascular outcomes in patients with non-ST-segment elevation acute coronary syndrome. Dis Markers. 2019;2019:6891537.
Jiao Y, Su Y, Shen J, Hou X, Li Y, Wang J, Liu B, Qiu D, Sun Z, Chen Y, et al. Evaluation of the long-term prognostic ability of triglyceride-glucose index for elderly acute coronary syndrome patients: a cohort study. Cardiovasc Diabetol. 2022;21(1):3.
Gao S, Ma W, Huang S, Lin X, Yu M. Impact of triglyceride-glucose index on long-term cardiovascular outcomes in patients with myocardial infarction with nonobstructive coronary arteries. Nutr Metab Cardiovasc Dis. 2021;31(11):3184–92.
Wang X, Xu W, Song Q, Zhao Z, Meng X, **a C, **e Y, Yang C, ** P, Wang F. Association between the triglyceride-glucose index and severity of coronary artery disease. Cardiovasc Diabetol. 2022;21(1):168.
Adeva-Andany MM, Martínez-Rodríguez J, González-Lucán M, Fernández-Fernández C, Castro-Quintela E. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab Syndr. 2019;13(2):1449–55.
Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011;14(5):575–85.
Park GM, Cho YR, Won KB, Yang YJ, Park S, Ann SH, Kim YG, Park EJ, Kim SJ, Lee SG, et al. Triglyceride glucose index is a useful marker for predicting subclinical coronary artery disease in the absence of traditional risk factors. Lipids Health Dis. 2020;19(1):7.
Liu X, Tan Z, Huang Y, Zhao H, Liu M, Yu P, Ma J, Zhao Y, Zhu W, Wang J. Relationship between the triglyceride-glucose index and risk of cardiovascular diseases and mortality in the general population: a systematic review and meta-analysis. Cardiovasc Diabetol. 2022;21(1):124.
Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68.
DeFronzo RA, Ferrannini E, Groop L, Henry RR, Herman WH, Holst JJ, Hu FB, Kahn CR, Raz I, Shulman GI, et al. Type 2 diabetes mellitus. Nat Rev Dis Primers. 2015;1:15019.
Drwiła D, Rostoff P, Gajos G, Nessler J, Konduracka E. Prognostic value of the triglyceride-glucose index among non-diabetic patients with acute myocardial infarction at one-year follow-up. Kardiol Pol. 2021;79(10):1116–23.
Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, Bittl JA, Cohen MG, DiMaio JM, Don CW, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e4–17.
Arnold SV, Bhatt DL, Barsness GW, Beatty AL, Deedwania PC, Inzucchi SE, Kosiborod M, Leiter LA, Lipska KJ, Newman JD, et al. Clinical management of stable coronary artery disease in patients with type 2 diabetes mellitus: a scientific statement from the American heart association. Circulation. 2020;141(19):e779–806.
Chen L, Ding XH, Fan KJ, Gao MX, Yu WY, Liu HL, Yu Y. Association between triglyceride-glucose index and 2-year adverse cardiovascular and cerebrovascular events in patients with type 2 diabetes mellitus who underwent off-pump coronary artery bypass grafting. Diabetes Metab Syndr Obes. 2022;15:439–50.
Gaudino M, Antoniades C, Benedetto U, Deb S, Di Franco A, Di Giammarco G, Fremes S, Glineur D, Grau J, He GW, et al. Mechanisms, consequences, and prevention of coronary graft failure. Circulation. 2017;136(18):1749–64.
Anderson RE, Brismar K, Barr G, Ivert T. Effects of cardiopulmonary bypass on glucose homeostasis after coronary artery bypass surgery. Eur J Cardio-thoracic Surg. 2005;28(3):425–30.
Doenst T, Wijeysundera D, Karkouti K, Zechner C, Maganti M, Rao V, Borger MA. Hyperglycemia during cardiopulmonary bypass is an independent risk factor for mortality in patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2005;130(4):1144.
Scudeler TL, Godoy LC, Hoxha T, Kung A, Moreno PR, Farkouh ME. Revascularization strategies in patients with diabetes and acute coronary syndromes. Curr Cardiol Rep. 2022;24(3):201–8.
Acknowledgements
We thank Liwen Bianji (Edanz) (www.liwenbianji.cn) for editing the English text of a draft of this manuscript.
Funding
The Bei**g Municipal Science and Technology Commission (Z191100006619106), the CAMS Innovation Fund for Medical Sciences (2023-I2M-1-001), and the National High Level Hospital Clinical Research Funding (2022-GSP-GG-17).
Author information
Authors and Affiliations
Contributions
YZ, LS, XF, and JY were involved in the conception, design, and conduct of the study and the analysis and interpretation of the results. YZ drafted the manuscript. CZ, LJ, JT, XZ, DW, YZ, KS, CZ, BX, WZ, RH, RG, JW, LS, XF, and JY contributed to the data acquisition. All authors approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Fuwai Hospital and performed in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all study participants.
Consent for publication
Written informed consent for publication was obtained from all participants.
Competing interests
The authors declares that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
The optimal cut point of TyG index.
Additional file 2: Table S1.
Details of the univariable and multivariable analysis of the association between TyG index and endpoint.
Additional file 3: Table S2.
The additional predictive value of the TyG index over diabetes for MACE.
Additional file 4: Table S3.
Associations between elevated TyG index and MACE in different disease phenotype groups.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Y., Zhang, C., Jiang, L. et al. An elevated triglyceride-glucose index predicts adverse outcomes and interacts with the treatment strategy in patients with three-vessel disease. Cardiovasc Diabetol 22, 333 (2023). https://doi.org/10.1186/s12933-023-02063-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-02063-4