
Abstract
Background
Digital infrared thermal imaging (DITI), which detects infrared rays emitted from body surface to create a body heat map, has been utilized at various musculocutaneous conditions. Notably, DITI can demonstrate autonomic vasomotor activity in the nerve-innervated area, and thus may be of use in carpal tunnel syndrome (CTS). In this study, we compared DITI findings before and after carpal tunnel release (CTR) surgery in patients with unilateral CTS to investigate the corresponding neurophysiological changes.
Methods
In this retrospective cohort study, DITI parameters such as the temperature differences between the median and ulnar nerve territories and median nerve-innervated digital anisometry were measured. Subjective symptom duration, pain scale, and ultrasonographic findings were also compared before and after CTR. Patients were evaluated before and 6 weeks after CTR, respectively.
Results
A total of 27 patients aged 59.0 ± 11.2 years were finally included. After CTR, median nerve-innervated thermal anisometry was improved (2.55 ± 0.96 °C to 1.64 ± 1.34 °C; p = 0.003). The temperature differences between the median and ulnar nerve territories were not significantly changed. Subjective pain, the Simovic Weinberg Clinical Scale, and palmar bowing of the flexor retinaculum were also significantly improved (p < 0.001 for all comparisons).
Conclusions
Our results demonstrated that DITI findings could reflect an improvement in autonomic function after CTR. Therefore, DITI can be an objective method to assess pre- and post-operative neurophysiologic changes in CTS.
Similar content being viewed by others


Background
Carpal tunnel syndrome (CTS) is one of the most common peripheral nerve entrapment syndromes which is caused by compression of the median nerve within the carpal tunnel [1]. Elevated carpal tunnel pressure and traction of median nerve can cause nerve injury, obstruction of venous outflow, and ischemia [2]. A recent anatomic study also suggests that myofascial stress affecting paraneural sheath plays a role in pathogenesis of CTS [3]. Also carpal tunnel syndrome is associated with repeated wrist use, pregnancy, diabetes, and systemic diseases such as hypothyroidism [4]. Symptoms include sensory changes such as tingling, abnormal sensation, and burning of the wrist and fingers along the innervation of the median nerve, and motor symptoms such as thenar atrophy and weakness. It is more common in women than in men and is known to occur bilaterally in more than 50% of cases [5].
Most CTS patients with mild to modest symptoms receive conservative treatments. However, severe CTS patients or those with nerve lesions proved by electrodiagnosis often require surgery [6]. Carpal tunnel release (CTR) is generally considered in cases which fail to respond to conservative treatment, develop weakness and atrophy of the thenar muscles, and traumatic CTS [7]. Previous studies have reported that more than 20% of patients with CTS underwent CTR [8, 9].
Although there is no definitive standard for the diagnosis of CTS, electrodiagnostic testing is widely used in conjunction with clinical symptoms. In addition to physical examinations such as Tinel’s sign and Phalen’s maneuver, methods such as US, magnetic resonance imaging, and infrared body thermography are used [10,11,12]. Infrared body thermography (DITI) detects infrared rays emitted from the surface of the human body and displays it as a body heat map according to the temperature differences. Specifically, DITI is known to be able to evaluate the function of sympathetic vasomotor fibers regulating cutaneous blood flow, which cannot be adequately tested by electrodiagnostic tests [13] . As a relatively inexpensive and non-invasive test, it is currently used for some pain-related diseases such as entrapment neuropathy, spinal neuropathy, and complex regional pain syndrome [14].
Several studies using DITI have been published in previous studies on CTS; unfortunately, they did not show consistent results, [15,16,17] including pre- and postoperative cases [18,19,20]. In our previous study, we reported that DITI findings may differ depending on the severity and symptom duration of CTS. As DITI reflects the state of the autonomic nervous system, the possibility of using DITI in CTS is plausible [21].
In this context, we aimed to identify the thermographic, clinical, and sonographic changes before and after CTR in patients with unilateral CTS. Subsequently, we primarily investigated the significance of DITI in the evaluation and understanding of neurophysiological changes after CTR.
Methods
Patients and assessments
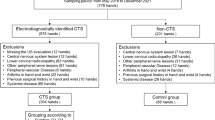
This retrospective cohort study was performed from January 2020 to July 2021 and used a database from a single hospital’s electrodiagnostic laboratory. Symptoms, signs and laboratory findings were compared before and after surgery in patients who had undergone surgical treatment for unilateral CTS. All patients showed clinical and electrodiagnostic findings consistent with CTS, and significant symptoms that were difficult to improve with conservative treatment, such as pharmacological or injection treatment. Patients with diseases that may affect DITI; including central nervous system lesions involving the affected hand, lower cervical radiculopathy, systemic peripheral neuropathy, peripheral vascular disease, arthritis of the hand, previous history of hand or wrist surgery; and systemic diseases such as tumor, thyroid diseases, fibromyalgia, and uncontrolled diabetes; were excluded. The study was approved by the local institutional review board (Approval number: PSSH0475–202201-HR-002-01).
The degree of pain was recorded through the numerical rating scale (NRS) before surgery, and Simovic Weinberg Clinical Scale [22] was used to rate the severity of symptoms. Electrodiagnostic testing was performed; based on nerve conduction studies and needle EMG findings, disease severity was classified under Steven’s classification [23] as mild, moderate, or severe.
Ultrasonography was performed using a linear probe (12–5 MHz) in the proximal carpal tunnel between the pisiform and scaphoid bones. Patients were examined in a sitting position, with the elbow flexed at 90 degrees and the forearm fully supinated. The cross-sectional area and palmar bowing of the median nerve were measured at the site, respectively.
Digital infrared thermographic parameters
The DITI test was performed according to the same protocol as previously published by these authors, and the same parameters were evaluated [21]. The IRIS-8000® (Medicore, Seoul, Korea) was used to record the thermographic image. Before electrodiagnosis, DITI was performed under the following conditions: the room temperature was maintained at 23–25 °C; the subject was dressed in loose clothing and allowed to acclimate to the environment for 15–20 min; the subject was placed 1.5 m from the thermographic camera; no lotion or ointment was applied before the test; topical patches, splints, and metal accessories were removed; vigorous exercise and physical therapy were to be avoided within 4 h of the test; no alcohol or caffeine consumption, or smoking were allowed within 12 h of the test.
We designated six regions of interest of the thermal image of the palmar surface. Skin temperature was measured at the center of the finger pulp of the first, second, third, and fifth digits based on an area of 400 data points. Additionally, measurements were obtained from the thenar and hypothenar eminences based on an area of 800 data points. The mean value of all data points in the study area was determined. By translating the approved red-green-blue data to temperature, the final result was displayed in degrees Celsius. We created the indicators below for data interpretation and quantitative analysis. The values were calculated by substituting the average body temperature obtained within each region of interest.
-
Temperature difference between the median and ulnar nerve digits (ΔM−U digits)
-
= (digit 1 + digit 2 + digit 3)/3−digit 5
-
-
Temperature difference between the thenar and hypothenar areas (Δthenar−hypothenar)
-
= thenar − hypothenar,
-
-
Temperature difference between the median and ulnar nerve territories (ΔM−U territories)
-
= ΔM−U digits + Δthenar–hypothenar,
-
-
Median nerve-innervated digits anisometry
-
= │digit 1−digit 2│ + │digit 1−digit 3│ + │digit 2−digit 3│
-
Surgical procedures
All patients underwent open CTR. The surgeon first made a 2 cm incision in the central part of the distal wrist. After dissecting the subcutaneous layer, the transverse carpal ligament was identified. Thereafter, decompression was performed by incision of the transverse carpal ligament while checking the median nerve sheath. Then, the surgeon removed adhesion tissues around the median nerve and confirmed that the nerve was sufficiently decompressed. Finally, each layer was sutured closed. Brachial plexus blockade was done prior to surgery.
Except for electromyography, NRS, SCS, ultrasonography, and DITI were evaluated according to the same protocol by the same evaluator 6 weeks after surgery.
Statistical analysis
Paired t-test was performed for each parameter before and after surgery. All statistical analyses were conducted using SPSS 22.0 (IBM, Armonk, NY, USA).
Results
Baseline characteristics
A total of 27 patients were included in this study; 7 men and 20 women with an average age of 59 ± 11.2 years. There were more participants with right hand than left hand involvement (right hand involvement: 59.3%). The average duration of symptoms was 12 ± 13.85 months. According to the electrodiagnostic severity grading, 3 patients were classified as moderate and 24 as severe; no patients were considered as mild (Table 1).
Clinical and sonographic findings
As a result of the study, the pain NRS score in the patients decreased from 6.07 ± 1.21 points before surgery to 2.07 ± 1.03 points 6 weeks after surgery (p < 0.001); and the Simovic Weinberg Clinical Scale changed from 25.44 ± 2.75 points before surgery to 6.67 ± 3.66 points (p < 0.001). Ultrasound findings of the median nerve cross-sectional area (CSA) in the proximal carpal tunnel was not significantly different from 0.20 ± 0.04 cm2 to 0.18 ± 0.08 cm2 before and after surgery, respectively (p = 0.191). However, a significant reduction in PB was observed, changing from 4.10 ± 0.71 mm to 3.24 ± 0.91 mm before and after surgery, respectively (p < 0.001) (Table 2).
Digital infrared thermographic findings
There was no statistically significant difference in both the skin temperature of each finger, except for the fourth finger (mediated by both median and ulnar nerves), and that of the thenar and hypothenar areas before and after surgery. Other processed parameters, including ΔM − U digits, Δthenar−hypothenar, and ΔM − U territories, showed no statistically significant differences before and after surgery. Only median nerve-innervated digits anisometry showed a significant decrease after surgery compared to before surgery (2.55 ± 0.96 °C to 1.64 ± 1.34 °C; p = 0.003) (Table 3).
Discussion
In this study, we demonstrated the decreased median nerve-innervated digital thermal ansiometry after CTR. This finding was in accordance with the postoperative improvement of clinical symptoms and US findings. In CTS, the increased interstitial fluid pressure in the carpal tunnel or the pressure that directly compresses the median nerve changes the microvasculature of the median nerve, resulting in ischemia and blood flow disorders [24]. Damage to unmyelinated small fibers in the early stages of CTS may increase thermal variation in areas innervated by the same nerve through mechanisms such as sympathetic dysfunction, reactive vasoconstriction, and antidromic sensory fiber activation [25]. Furthermore, a neuroanatomic study recently identified superficial fascia to be innervated by autonomic and sensory nerve fibers, which suggests the role of superficial fascia stress in CTS [26]. We have reported in a previous study that as the severity of CTS worsens, the anisometry also gradually increases [21]. Anisometry of median-nerve innervated digits might suggest that as disease progresses, damage in thin-unmyelinated fibers cause disregulaton of vasomotor activity, thereby resulting in thermal variations within the same nerve-innervated area.
Infrared thermographic changes were observed, along with pain reduction and clinical improvement after CTR in this study. It can be inferred that the statistically significant decrease in anisometry values after CTR in this study is due to the improvement of blood flow and autonomic function in the median nerve-innervated area after decompression of the carpal tunnel. On the other hand, there was no significant change in skin temperature other than anisometry after surgery. Specifically, secondary parameters, such as ΔM − U digits, Δthenar−hypothenar, and ΔM − U territories did not show significant changes after surgery. According to our previous study, these parameters, as opposed to anisometry, stand out in the early stage of the disease, but become less apparent as the severity and duration of the disease increases [21]. Those who underwent surgery were electrodiagnostically severe in most cases (88.9%), with an average prolonged symptom duration of 12.0 months. Therefore, the indicators which showed a marked difference in the early stage of the disease did not change much postoperatively. An exception to this was in the case of anisometry, which became more prominent as the disease progressed, demonstrating improvement after the operation. There have been previous studies which have identified autonomic changes before and after CTR by utilizing the advantages of DITI. Ming et al. [18] observed changes in DITI findings before, and 6 months after, CTR in 22 patients with CTS. Similar to our findings, they reported a decrease in median nerve-innervated digits anisometry. However, their results showed that median-ulnar territory difference significantly diminished, which is discordant to our study. Ming et al. do not mention disease severity, unlike our study where the patients may be a more severe and homogenous group. ΔM − U territories values from Ming et al. in CTS patients tended to be higher than that of healthy controls or than that of the participants in our study, and ΔM − U territories is a parameter that diminishes as the disease progresses [21]. Another study by Baic et al. [19] compared the temperature differences of the thenar area and eight sites of median nerve-innervated digits. While their study analysis on digits was too segmented, they also demonstrated better temperature distribution within the median territory after CTR compared to the thenar area. Meanwhile, Bargiel et al. [20] performed three DITI tests on 40 patients who underwent CTR 2 days before and 2 weeks after surgery. As a result, they reported alleviation of clinical symptoms after carpal tunnel surgery, but no improvement in thermographic findings. However, Bargiel et al. used a different methodology than our study, and only examined overall hand temperature before and after cooling by dynamic thermography. Subsequently, previous studies between CTR and DITI findings have shown inconsistent results; further studies to identify neurophysiologic changes after CTR are still lacking. This study’s results can be validated because the study parameters are based on our previous study, which reported on the possibility of using DITI in CTS; in particular, we primarily suggested that DITI reflects the state of the autonomic nervous system and shows different findings depending on the severity and symptom duration of CTS [21].
Since the median nerve contains most of the sympathetic nerves of the hand [27], it is thought that autonomic dysfunction may occur in CTS [28]. Therefore, there have been studies using various approaches to evaluate autonomic dysfunction caused by median nerve compression in CTS. Methods such as sympathetic skin response (SSR), vasomotor response by Doppler technique, and capillaroscopy are used to evaluate sympathetic activity [29, 30]. Among them, capillaroscopy and Doppler have rarely been performed in CTS. While several studies on sympathetic skin response in CTS patients have been conducted, their results were inconsistent. Although there was no difference between affected and unaffected hands in some studies [30], others have shown decreased sympathetic activity in CTS [31,32,33]. In a postoperative study, the SSR before and after CTR failed to reflect post-surgical improvement in one study [34], yet in another study, the SSR amplitude ratio was restored after surgery [35]. The use of SSR in CTS is limited as it has not been established which of several parameters such as amplitude, median/ulnar latency difference, SSR waveform, etc., has diagnostic value in CTS. Therefore, DITI is considered the only objective tool to be able to assess the function of the small nerve fibers of CTS.
Electrodiagnostic testing is widely used in clinical practice as a tool to confirm CTS. However, while neuro-electrophysiological examination shows a strong correlation with the functional aspect of the median nerve, there are cases where there is no clear correlation with the symptoms of actual patients [36]. Moreover, there is also a study which found that there is no significant correlation with the degree of improvement of clinical symptoms after surgery [34]. In the early stages of nerve injury, damage to the unmyelinated small fibers, which conduct electrical impulses of the autonomic nervous system, occurs first. However, electrical diagnostic testing is limited with regards to reflecting the damage to these small fibers [37]. In addition, ultrasonography is also a widely used modality; it can directly check the morphology of the damaged nerve with the naked eye, examine both sides simultaneously, enable dynamic study, and can be used to guide treatment administration via injection [38]. Regarding the postoperative US findings of CTS, El-Karabaty et al. [39] reported that the flattened median nerve recovered to its normal shape after carpal tunnel decompression. Naranjo et al. [40] reported that the prognosis of surgery is good when the difference in the median nerve cross-sectional area before and after surgery is small. However, US can only confirm anatomical abnormalities and does not directly reflect the functional state or level of nerve damage. In our study, the degree of PB decreased after CTR, however, this is a direct anatomical change due to CTR. The CSA, which objectively determines the extent of median nerve swelling, did not show any significant changes after surgery. Therefore, it did not accurately reflect the improved pain level and clinical symptoms after surgery.
This study has several limitations. This study is a retrospective study with single-center’s database and further validation studies are needed. Another objective test, an electrodiagnostic test, could not be performed after surgery, hence analysis thereof was not done. It unconfirmed whether there were other symptoms related to vasomotor function. Since DITI abnormalities are interpreted as being related to thin unmyelinated nerve fiber dysfunction, it is necessary to investigate whether there are other subjective complaints related to this in future studies.
Conclusions
Carpal tunnel decompression surgery improved anisometry between median nerve-innervated digits in digital infrared thermal imaging, which is thought to be due to the improvement of vasomotor activity and blood flow mediated by the autonomic nervous system. This study suggests that digital infrared thermal imaging could possibility be of use as an objective evaluation method after carpal tunnel release.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CTR:
-
Carpal tunnel syndrome
- CTS:
-
Carpal tunnel surgery
- DITI:
-
Digital infrared thermal imaging
- NRS:
-
Numerical rating scale of pain
- SWCS:
-
Simovic and Weinberg Clinical Scale
- US:
-
Ultrasound
- CSA:
-
Cross-sectional area
References
Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosén I. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999;282(2):153–8.
Aboonq MS. Pathophysiology of carpal tunnel syndrome. Neurosciences (Riyadh). 2015;20(1):4–9.
Stecco C, Giordani F, Fan C, Biz C, Pirri C, Frigo AC, et al. Role of fasciae around the median nerve in pathogenesis of carpal tunnel syndrome: microscopic and ultrasound study. J Anat. 2020;236(4):660–7.
de Krom MC, Kester AD, Knipschild PG, Spaans F. Risk factors for carpal tunnel syndrome. Am J Epidemiol. 1990;132(6):1102–10.
Buchberger W, Schön G, Strasser K, Jungwirth W. High-resolution ultrasonography of the carpal tunnel. J Ultrasound Med. 1991;10(10):531–7.
Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal tunnel syndrome: a review of literature. Cureus. 2020;12(3):e7333.
Schmelzer RE, Della Rocca GJ, Caplin DA. Endoscopic carpal tunnel release: a review of 753 cases in 486 patients. Plast Reconstr Surg. 2006;117(1):177–85.
Liawrungrueang W, Wongsiri S. Effectiveness of surgical treatment in carpal tunnel syndrome Mini-incision using MIS-CTS kits: a cadaveric study. Adv Orthopedics. 2020;2020:8278054.
Siegmeth AW, Hopkinson-Woolley JA. Standard open decompression in carpal tunnel syndrome compared with a modified open technique preserving the superficial skin nerves: a prospective randomized study. J Hand Surg Am. 2006;31(9):1483–9.
Buchberger W. Radiologic imaging of the carpal tunnel. Eur J Radiol. 1997;25(2):112–7.
Mesgarzadeh M, Schneck CD, Bonakdarpour A, Mitra A, Conaway D. Carpal tunnel: MR imaging. Part II Carpal tunnel syndrome. Radiology. 1989;171(3):749–54.
Tchou S, Costich JF, Burgess RC, Wexler CE. Thermographic observations in unilateral carpal tunnel syndrome: report of 61 cases. J Hand Surg. 1992;17(4):631–7.
Nahm FS. Infrared thermography in pain medicine. Korean J Pain. 2013;26(3):219–22.
Ming Z, Zaproudina N, Siivola J, Nousiainen U, Pietikainen S. Sympathetic pathology evidenced by hand thermal anomalies in carpal tunnel syndrome. Pathophysiology. 2005;12(2):137–41.
Meyers S, Cros D, Sherry B, Vermeire P. Liquid crystal thermography: quantitative studies of abnormalities in carpal tunnel syndrome. Neurology. 1989;39(11):1465–9.
Herrick RT, Herrick SK. Thermography in the detection of carpal tunnel syndrome and other compressive neuropathies. J Hand Surg Am. 1987;12(5 Pt 2):943–9.
So YT, Olney RK, Aminoff MJ. Evaluation of thermography in the diagnosis of selected entrapment neuropathies. Neurology. 1989;39(1):1–5.
Ming Z, Siivola J, Pietikainen S, Närhi M, Hänninen O. Postoperative relieve of abnormal vasoregulation in carpal tunnel syndrome. Clin Neurol Neurosurg. 2007;109(5):413–7.
Baic A, Kasprzyk T, Rżany M, Stanek A, Sieroń K, Suszyński K, et al. Can we use thermal imaging to evaluate the effects of carpal tunnel syndrome surgical decompression? Medicine (Baltimore). 2017;96(39):e7982.
Bargiel P, Czapla N, Prowans P, Kotrych D, Ziętek P, Lusina D, et al. Thermography in the diagnosis of carpal tunnel syndrome. Open Med (Wars). 2021;16(1):175–82.
Park D, Kim BH, Lee SE, Kim DY, Eom YS, Cho JM, et al. Application of digital infrared thermography for carpal tunnel syndrome evaluation. Sci Rep. 2021;11(1):21963.
Simovic D, Weinberg DH, Allam G, Hayes MT. A quantitative clinical scale for the carpal tunnel syndrome. 50th Annual Meeting of the American Academy of Neurology (AAN). Minneapolis, 25 April-2 May 1998, Poster 05.119. Neurology. 1998;50;5119.
Stevens JC. AAEM minimonograph #26: the electrodiagnosis of carpal tunnel syndrome. American Association of Electrodiagnostic Medicine. Muscle Nerve. 1997;20(12):1477–86.
Akelman E, Weiss AP. Carpal tunnel syndrome. Etiology and endoscopic treatment. Orthop Clin North Am. 1995;26(4):769–78.
Sun PC, Kuo CD, Chi LY, Lin HD, Wei SH, Chen CS. Microcirculatory vasomotor changes are associated with severity of peripheral neuropathy in patients with type 2 diabetes. Diab Vasc Dis Res. 2013;10(3):270–6.
Fede C, Petrelli L, Pirri C, Neuhuber W, Tiengo C, Biz C, et al. Innervation of human superficial fascia. Front Neuroanat. 2022;16:981426.
Phalen GS. The carpal-tunnel syndrome. Seventeen years' experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am. 1966;48(2):211–28.
Verghese J, Galanopoulou AS, Herskovitz S. Autonomic dysfunction in idiopathic carpal tunnel syndrome. Muscle Nerve. 2000;23(8):1209–13.
Galea LA, Mercieca A, Sciberras C, Gatt R, Schembri M. Evaluation of sympathetic vasomotor fibres in carpal tunnel syndrome using continuous wave Doppler ultrasonography. J Hand Surg (Br). 2006;31(3):306–10.
Zyluk A, Kosovets L. An assessment of the sympathetic function within the hand in patients with carpal tunnel syndrome. J Hand Surg Eur Vol. 2010;35(5):402–8.
Reddeppa S, Bulusu K, Chand PR, Jacob PC, Kalappurakkal J, Tharakan J. The sympathetic skin response in carpal tunnel syndrome. Auton Neurosci. 2000;84(3):119–21.
Kiylioglu N, Akyol A, Guney E, Bicerol B, Ozkul A, Erturk A. Sympathetic skin response in idiopathic and diabetic carpal tunnel syndrome. Clin Neurol Neurosurg. 2005;108(1):1–7.
Zyluk A, Kosowiec L. Regional sympathetic disturbances in carpal tunnel syndrome--a review. Chir Narzadow Ruchu Ortop Pol. 2008;73(1):30–6.
Mondelli M, Reale F, Sicurelli F, Padua L. Relationship between the self-administered Boston questionnaire and electrophysiological findings in follow-up of surgically-treated carpal tunnel syndrome. J Hand Surg (Br). 2000;25(2):128–34.
Kanzato N, Komine Y, Kanaya F, Fukiyama K. Preserved sympathetic skin response at the distal phalanx in patients with carpal tunnel syndrome. Clin Neurophysiol. 2000;111(11):2057–63.
Padua L, Padua R, Lo Monaco M, Aprile I, Tonali P. Multiperspective assessment of carpal tunnel syndrome: a multicenter study. Italian CTS Study Group. Neurology. 1999;53(8):1654–9.
Smith NJ. Nerve conduction studies for carpal tunnel syndrome: essential prelude to surgery or unnecessary luxury? J Hand Surg (Br). 2002;27(1):83–5.
Petrover D, Richette P. Treatment of carpal tunnel syndrome : from ultrasonography to ultrasound guided carpal tunnel release. Joint Bone Spine. 2018;85(5):545–52.
El-Karabaty H, Hetzel A, Galla TJ, Horch RE, Lücking CH, Glocker FX. The effect of carpal tunnel release on median nerve flattening and nerve conduction. Electromyogr Clin Neurophysiol. 2005;45(4):223–7.
Naranjo A, Ojeda S, Araña V, Baeta P, Fernández-Palacios J, García-Duque O, et al. Usefulness of clinical findings, nerve conduction studies and ultrasonography to predict response to surgical release in idiopathic carpal tunnel syndrome. Clin Exp Rheumatol. 2009;27(5):786–93.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
YEP contributed to interpreting the data and writing the manuscript; JWL and DP were in charge and contributed to design of the study, data interpretation and critical revision; SEL, YSE, JMC, JWY, MSK and HDK carried out data collection. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All methods in current study were performed in accordance with the standards of the institutional board, and in compliance with the Declaration of Helsinki and the International Conference on Harmonization-Good Clinical Practice Guideline. The study protocol was approved by the Institutional Review Board (Approval no.: PSSH0475–202201-HR-002-01) of Pohang Stroke and Spine Hospital. Because of the retrospective study design, the Institutional Review Board of Pohang Stroke and Spine Hospital allowed the omission of informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare of not having any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Park, Y.E., Lee, SE., Eom, Y.S. et al. Infrared thermographic changes after decompression surgery in patients with carpal tunnel syndrome. BMC Musculoskelet Disord 24, 79 (2023). https://doi.org/10.1186/s12891-023-06193-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06193-4