
Abstract
Background
Patients with ankylosing spondylitis (AS) have significantly lower quality of life (QoL) than the general population. Holistic interventions addressing QoL comprise spa- or balneotherapy including radon. These interventions have shown to be beneficial in reducing pain and improving QoL in AS-patients. We explored the association of spa-therapy including low-dose radon with QoL in AS-patients over an extended time period.
Methods
Registry data collected for the “Radon indication registry” in the Austrian Gastein valley comprising data on QoL (EuroQol EQ-5D) directly before the treatment (baseline), directly(t1), 3 (t2); 6(t3) and 9(t4) months after the treatment, age, sex and body mass index (BMI) were analysed. Linear regression models explored the association of measurement time with 1) EQ-5D-5L utilities and 2) EuroQol visual analogue scale (VAS) score. Alterations of 0.05 (utilities) and 5.00 (VAS) were considered clinically relevant.
Results
Two-hundred-ninety-one AS-patients were included in the analyses. Forty-four percent (n = 128) were women, the mean age was 52 (SD 10) and the average BMI was 26 (SD 4). Utilities (t1: 0.09 [0.07;0.11]; t2: 0.08 [0.06; 0.10]; t3: 0.06 [0.05;0.09]; t4: 0.04 [0.02;0.06]) and VAS (t1: 11.68 [9.38; 13.97]; t2: 12.20 [9.78; 14.61]; t3: 9.70 [7.24; 12.17]; t4: 6.11 [3.57; 8.65]) were significantly higher at all timepoints compared to baseline. Improvements were clinically relevant at all timepoints in case of the VAS and until 6 months after treatment for the utilities.
Conclusion
AS-patients who received spa therapy including radon show significantly and clinically relevant improvements in Qol until 6–9 months after treatment.
Similar content being viewed by others


Introduction
Ankylosing spondylitis (AS) is the most common form of the rheumatic disease group of spondyloarthritis. It occurs in approximately 23.8 per 10,000 Europeans [1] and is more prevalent in men than women. AS affects the axial skeleton leading to inflammatory back pain, damage to physical structures as well as impairments in physical functioning. These impairments may result in reduced participation and decreased quality of life (QoL). [1,2,3,4] The growing understanding of QoL as key factor when measuring the effectiveness of healthcare interventions as well as the embracement of bio-psychosocial models rather than just biological models for the evaluation of health emphasize the relevance of interventions focussing on the improvement of QoL [5, 6].
Previous research has pointed out that AS-patients have significantly lower QoL than the general population but that pharmacological treatment is beneficial in improving their QoL. Particularly the combination of anti-TNF-α therapy in combination with physical exercise may reduce the adverse effect of AS on QoL [7, 8].
However, the evidence on the effectiveness of alternative or complementary non-pharmacological interventions in improving QoL in AS patients is still limited. Common symptom-oriented interventions like physiotherapeutic treatment are effective in the reduction of disease activity and pain as well as the improvement of functional capacity [9] Yet, holistic interventions have the potential of addressing a wider range of the AS-patient’s health state including mental health and participation in daily life [10, 11]. Those aspects are particularly relevant when assessing QoL from a patient’s perspective.
Holistic interventions for AS regularly comprise multidisciplinary treatments including spa- or balneotherapy/speleotherapy. Still, little is known about the effect of these interventions on QoL. Kamioka et al. summarized the body of knowledge in an overview of systematic reviews with meta-analysis based on randomized controlled trials of balneotherapy and spa-therapy from 2000 to 2019 and did not identify any review focussing on spa-therapy in relation to QoL [12]. A limited number of studies specifically addressed the effectiveness of combined spa‐exercise therapy on QoL. For example, Colina et al. demonstrated that in AS patients, combining pharmacological treatment with spa-therapy resulted in significantly better QoL than pharmacological treatment alone six months after treatment initiation [13]. A randomized controlled trial by van Tubergen et al. showed that QoL, expressed by EuroQol-5D utilities, was significantly higher in patients that received spa-therapy (one with and one without radon treatment) compared to those who received usual care until 40 weeks after the treatment. In this study, the application of utilities enabled valuation of QoL from a societal perspective (i.e., utility values accounted for preferences the society has for a particular health state).[14].
Among spa-therapies, treatment with low-dose radon has shown to be effective in achieving long-term pain reduction in persons with musculoskeletal diseases (including AS) [11, 15,16,17,18,19] and showed promising results with regard to improvements in functionality [20, 21] as well as in QoL [22, 23]. However, to the best of our knowledge, until now no data exist on the association of spa therapy including radon with systematically monitored QoL in patients with AS over an extended period of time while accounting for both, QoL from a societal perspective and individually perceived QoL.
Therefore, the aim of the current study was to explore whether spa treatment including low-dose radon results in sustained significant and clinically relevant improvement of QoL in patients with AS.
Methods
The current study concerns a longitudinal analysis of prospectively collected registry data from the ongoing “Radon indication registry for the assessment of pain reduction, increase of quality of life and improvement in body functionality throughout low-dose radon hyperthermia therapy” (registration ID ISRCTN67336967; https://doi.org/10.1186/ISRCTN67336967) in the valley of Gastein in Austria. The registry collects data from individuals visiting the valley of Gastein for the purpose of spa-treatment including radon for a variety of rheumatic diseases. They are recruited for participation by the physicians of participating spa centres in the Gastein valley. Data are collected following informed consent by means of standardized paper questionnaires that are completed by participants directly before commencement of the treatment (baseline), directly after the treatment and 3; 6 and 9 months after the treatment. Questionnaires are sent out by medical employees of the participating centres for the last three timepoints and are handed over in person for the first two timepoints. Questionnaires are then sent back to the spa centres and handed over to the Gastein research institute after pseudonymization. There a research assistant enters the data manually into the database.
Population
At the time of analysis for the current manuscript, the radon indication registry comprised 469 AS patients, 541 patients with low back pain, 176 patients with rheumatoid arthritis, 124 patients with osteoarthritis (OA) of the knee, 45 patients with OA of the hip, 16 patients with fibromyalgia and 32 patients with Psoriatic arthritis. For the current study, only AS patients were included if they had provided complete data at each timepoint for all variables included in the analyses. (Fig. 1).

Flow chart of study sample selection
Intervention
The intervention consisted of an individualized (i.e. based on local spa-physicians prescription) spa-treatment including radon in the valley of Gastein in the Austrian Alps with an average duration of 17.5 days (SD 3.5). This so-called low-dose radon balneo/speleo therapy (LDRnBST; radon-therapy) is part of a holistic treatment program for patients with AS and is applied in terms of balneo- and/or speleotherapy. The former includes bathing in water (~ 37 °C) with low activity of radon (average 707.57 (SD 233.27)Bq/l measured by liquid scintillation, Triathler™ LSC Hidex) as applied by the local facilities according to standardized treatment regimens. The thermal water consists of several mineral substances e.g., sodium – 80,01 mg/l; potassium – 5,71 mg/l; calcium – 19,84 mg/l; magnesium – 0,75 mg/l; hydrogen carbonate – 57,91 mg/l; chloride – 24,96 mg/l; flourid – 5,61 mg/l; sulphate – 130,67 mg/l; carbon dioxide – 6,87 mg/l.[24].
A balneotherapy intervention including low-dose radon consists of approximately 10 baths with a duration of 20 min. Speleotherapy including low-dose radon describes the process of relaxation while being exposed to a low activity of radon (average 44 kBq/m3, as indicated by healing gallery), high humidity (70–100%) and mild hyperthermia (37–41.5 °C) in the healing gallery of Gastein (a former gold mine located in moderate altitude (1270 m) above sea level) for an average time of 60 min on alternate days (i.e. an average of 11 speleotherapy sessions).[25] Both forms of radon therapy evoke a mild form of hyperthermia and increase the body temperature.
Outcomes
The EuroQol EQ-5D-5L (© EuroQol Research Foundation. EQ-5D™, hereafter referred to as EQ-5D) is a self-reported questionnaire consisting of two parts, a descriptive system comprising 5 dimensions of health (i.e., mobility, self-care, usual activities, pain/discomfort, anxiety/depression) and a visual analogue scale (VAS) capturing participant’s self-rated health status on a 0–100 scale with higher values representing better health. Using the unique score from each of the 5 dimensions of health a utility index score can be calculated (i.e., von Neumann-Morgenstern utility value for current health) [26].
Single values for each of the 5 dimensions reflect the level of problem with each dimension resulting in an individual health state. This health state can be converted into a weighted health state by applying scores from the EQ-5D preference weights extracted from the general population which can take a value from 0 (death) to 1 (full health).
The EQ-5D utility index and EuroQol VAS were used as outcome variables for the current study. In absence of Austrian population weights, German population weights were used to calculate the EQ-5D utility index [27].
Main independent variable of interest and covariates
The timepoint of survey completion by the participants was used as main independent variable of interest. Covariates were chosen a priori and included age (in years), sex (men/women) and body mass index (BMI; BMI = weight[kg]/height[m]2) due to their already established influence on health and health related QoL [28,29,30].
Statistical analyses
First, descriptive statistics were used to characterize the sample in terms of age, gender and BMI at baseline (i.e., directly before the intervention) and to describe the EQ-5D utility index and VAS-score for each of the timepoints of measurement. Next, two linear regression models were computed to explore the association of timepoint of measurement with a) the EQ-5D utility index and b) the EuroQol VAS-score while adjusting for age, sex and BMI. After each model, margins and their 95% confidence interval (CI) were calculated to produce specific age, gender and BMI standardized estimates for the utility index and VAS score.
P-values ≤ 0.05 were considered statistically significant. A change of ≥ 0.05 in the EQ-5D utility index and of ≥ 5.00 in the EuroQol VAS was considered clinically relevant [31, 32].
Results
The final sample included in the analyses consisted of 291 participants who provided complete data for all timepoints (Fig. 1). The sample consisted of 128 women, the mean age was 52 years and the average BMI was 26. Table 1 shows the unstandardized EQ-5D utility index and VAS scores for each timepoint. Figure 2 illustrates the course of the dimensions (i.e. mobility, self-care, usual activities, pain/discomfort, anxiety/depression) based on which the utility index was calculated.

Unadjusted average course of health based on EQ-5D health dimensions (dimension score range 1–5 with lower scores representing better health)
Health over time EQ-5D utility index
The age, sex and BMI standardized association of timepoint of measurement and utility index showed that at each timepoint, the index value was significantly higher than the baseline value indicating better health. Directly, 3 months and 6 months after the intervention the index value increased by 0.09 [95%CI 0.07;0.11], 0.08 [95% CI 0.06; 0.10] and 0.06 [95% CI 0.05;0.09], respectively. Since all increases exceeded 0.05, they reflected a clinically relevant change [31].
Nine months after the intervention the utility index was still increased (0.04 [95% CI 0.02;0.06]) but this improvement was not clinically relevant. (Table 2).
Health over time euroQol VAS
The age, sex and BMI standardized association of timepoint of measurement and EuroQol VAS showed that at each timepoint, the VAS score was significantly higher than the baseline value indicating better health. Directly, 3 months, 6 months and 9 months after the intervention the VAS score increased by 11.68 [95%CI 9.38; 13.97], 12.20 [95% CI 9.78; 14.61], 9.70 [95% CI 7.24; 12.17] and 6.11 [95% CI 3.57; 8.65], respectively. These increases reflected a clinically relevant change since they were larger than 5.00 [32]. (Table 2).
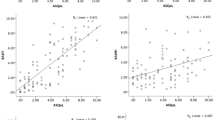
Figure 3 illustrates the age, sex and BMI adjusted course of self-reported health state based on EuroQol VAS scores and utility index score.

Age, sex and BMI adjusted course of self-reported health state based on EuroQol VAS scores and utility index score (utility index range 0–1; VAS-score range 0–100 with higher scores representing better health)
Discussion
To our knowledge, this is the first time that systematically collected registry data have been used to explore the association between spa-therapy including radon with alterations in QoL in AS patients over a period of 9 months. Significant improvements in QoL were seen immediately and were sustained until 9 months after the intervention. Predicted mean scores based on linear regression models showed these improvements were clinically relevant until 6 months after the intervention in case of the EQ-5D utility index and until 9 months after the intervention in case of the EQ-VAS while accounting for individual differences in patient characteristics. Generally, these findings are in agreement with other studies focussing on the benefits of spa therapy for QoL in AS patients.[13, 14, 22, 23].
Some differences were found in the course of the utility index compared to the course of the VAS-score. The utility index showed the largest improvement directly after the intervention while the VAS score was highest 3 months after the intervention. The latter is in agreement with other publications focussing on symptom relief and alterations in QoL through spa-therapy including radon which show a delayed therapy response. For example, van Tubergen et al. found the same delay when focussing on the EQ-5D utility index [14]. However, in our study the delay was only observed in the VAS-score. A possible explanation might be found in the different population preferences accounted for in the calculation of utilities in the current study (German preference weights) compared to the study of van Tubergen et al. (Dutch preference weights). Yet, the unadjusted illustration of the 5 dimensions of health prior to the application of preference weights shows the same course of improvement suggesting that another explanation is more likely. Selection bias might be one: The observation may be attributable to the specific population included. Provision of data for the radon registry is voluntarily and participants included in the current study had provided complete data at all timepoints. This might indicate high motivation attributable to favourable treatment effects that are more precisely represented by the utility index than by the VAS score. An interesting side finding was that men had significantly higher EQ-VAS scores compared to women independent of their age, BMI or the timepoint of measurement. Previous research showed, that women with AS have less improvement in AS related outcome measures compared to men. However, the reason for this phenomenon remained unclear [33]. In the current study the difference between men and women was not clinically relevant and only occurred in case of the VAS but not the utility index, which might suggest that perception of health plays a relevant role.
Clinically relevant changes attributable to spa therapy including radon have, to our knowledge, not been addressed by previous studies. The current evidence points out that in our cohort of AS-patients clinically relevant improvements in QoL can be sustained until 6 months (utility index) or even 9 months (VAS) after intervention. From a clinical perspective, this indicates the benefits of a repetitive treatment pattern. To achieve stable results, a periodic intervention should be scheduled every 6 months.
Limitations and Strengths
As in all studies based upon registry data limitations arise from the fact that data collection is not monitored or performed by the researcher and that data on confounders is somewhat limited [34].
In the current study data on the frequency of interventions prior to the first timepoint of measurement were not systematically collected. This might have resulted in biased baseline values as participants who have received the intervention repeatedly likely have a better baseline health state than those who receive the intervention for the first time leading to a potential underestimation of the improvement in first-time participants. Moreover, it should be considered that in pre-post estimations, the nature of self-reported measures may lead to biased responses due to the direct effect of an intervention on participant’s perception of health rather than their actual health (i.e. response shift) [35].
Confounders in the association of QoL with AS have been identified in previous literature and might have affected the current analyses as well. For example, a lower level of education and being a smoker is associated with lower QoL but this information was not available.[36].
Strengths of the study include a relatively large study sample with complete data over an extended period of time as well as the independence of data collection. Since data on the effectiveness of spa therapy including radon on the improvement of QoL in AS patients is still scarce, the current study provides relevant insights and opportunities for further research among other patient populations, and in comparison with usual care.
Conclusion
In conclusion, the current study reveals that AS patients who received spa-therapy including low-dose radon show significantly and clinically relevant improvements in Qol and that these improvements are sustained for up to 9 months. It may be considered a valuable (complementary) treatment option for this purpose. Extrapolation of the results may support the decision of policy makers and insurances to refund bi-annual spa therapy including radon for patients with AS.
Availability of data and materials
The datasets used and/or analysed during the current study are publicly available from the open data storage platform Zenodo using the following link: https://doi.org/10.5281/zenodo.5926209.
Abbreviations
- AS:
-
Ankylosing spondylitis
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- EQ:
-
EuroQol
- QoL:
-
Quality of life
- RnIR:
-
Radon indication registry for the assessment of pain reduction, increase of quality of life and improvement in body functionality throughout low-dose radon hyperthermia therapy
- VAS:
-
Visual analogue scale
References
Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ. Global prevalence of ankylosing spondylitis. Rheumatology (Oxford). 2014;53(4):650–7.
Rusman T, van Vollenhoven RF, van der Horst-Bruinsma IE. Gender Differences in Axial Spondyloarthritis: Women Are Not So Lucky. Curr Rheumatol Rep. 2018;20(6):35.
Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369(9570):1379–90.
van Genderen S, Plasqui G, van der Heijde D, van Gaalen F, Heuft L, Luime J, et al. Social Role Participation and Satisfaction With Life: A Study Among Patients With Ankylosing Spondylitis and Population Controls. Arthritis Care Res (Hoboken). 2018;70(4):600–7.
Calvert MJ, Freemantle N. Use of health-related quality of life in prescribing research. Part 1: why evaluate health-related quality of life? J Clin Pharm Ther. 2003;28(6):513–21.
Addington-Hall J, Kalra L. Who should measure quality of life? BMJ. 2001;322(7299):1417–20.
Tanski W, Swiatoniowska-Lonc N, Dudek K, Jankowska-Polanska B. Benefit of Biological Drugs for Quality of Life in Patients with Ankylosing Spondylitis: A Systematic Review and Meta-Analysis of Clinical Trials. Adv Exp Med Biol. 2021;1335:63–78.
Kotsis K, Voulgari PV, Drosos AA, Carvalho AF, Hyphantis T. Health-related quality of life in patients with ankylosing spondylitis: a comprehensive review. Expert Rev Pharmacoecon Outcomes Res. 2014;14(6):857–72.
Gravaldi LP, Bonetti F, Lezzerini S, De Maio F. Effectiveness of Physiotherapy in Patients with Ankylosing Spondylitis: A Systematic Review and Meta-Analysis. Healthcare. 2022;10(1):132.
Packham J. Optimizing outcomes for ankylosing spondylitis and axial spondyloarthritis patients: a holistic approach to care. Rheumatology (Oxford). 2018;57(6):29–34.
Moder A, Foisner W, Hitzl W, Fagerer N, Ritter M, Kullich W. Schmerz, Krankenstände, Befindlichkeit, Medikamentenverbrauch und Funktionsverbesserung im Jahr vor und nach einer kombinierten Radonthermalkur. Physikalische Medizin, Rehabilitationsmedizin, Kurortmedizin. 2011;21(05):215–9.
Kamioka H, Nobuoka S, Iiyama J. Overview of Systematic Reviews with Meta-Analysis Based on Randomized Controlled Trials of Balneotherapy and Spa Therapy from 2000 to 2019. Int J Gen Med. 2020;13:429–42.
Colina M, Ciancio G, Garavini R, Conti M, Trotta F, Govoni M. Combination treatment with etanercept and an intensive spa rehabilitation program in active ankylosing spondylitis. Int J Immunopathol Pharmacol. 2009;22(4):1125–9.
Van Tubergen A, Boonen A, Landewe R, Rutten-Van Molken M, Van Der Heijde D, Hidding A, et al. Cost effectiveness of combined spa-exercise therapy in ankylosing spondylitis: a randomized controlled trial. Arthritis Rheum. 2002;47(5):459–67.
Lind-Albrecht G. Der therapeutische Einsatz von Radon. arthritis +rheuma. 2007;27:272–8.
Lind-Albrecht G. Einfluss der Radonstollentherapie auf Schmerzen und Verlauf bei Spondylitis ankylosans (M. Bechterew): eine randomisierte prospektive Studie. Dissertation thesis. Johannes-Gutenberg-University Mainz. 1994.
Ruhle PF, Wunderlich R, Deloch L, Fournier C, Maier A, Klein G, et al. Modulation of the peripheral immune system after low-dose radon spa therapy: Detailed longitudinal immune monitoring of patients within the RAD-ON01 study. Autoimmunity. 2017;50(2):133–40.
Ruhle PF, Klein G, Rung T, Tiep Phan H, Fournier C, Fietkau R, et al. Impact of radon and combinatory radon/carbon dioxide spa on pain and hypertension: Results from the explorative RAD-ON01 study. Mod Rheumatol. 2019;29(1):165–72.
Kullmann M, Ruhle PF, Harrer A, Donaubauer A, Becker I, Sieber R, et al. Temporarily increased TGFbeta following radon spa correlates with reduced pain while serum IL-18 is a general predictive marker for pain sensitivity. Radiat Environ Biophys. 2019;58(1):129–35.
Moder A, Hufnagl C, Lind-Albrecht G, Hitzl W, Hartl A, Jakab M, et al. Effect of combined Low-Dose Radon- and Hyperthermia Treatment (LDRnHT) of patients with ankylosing spondylitis on serum levels of cytokines and bone metabolism markers: a pilot study. Int J Low Radiat. 2010;7(6):423–35.
Lange U, Dischereit G, Tarner I, Frommer K, Neumann E, Muller-Ladner U, et al. The impact of serial radon and hyperthermia exposure in a therapeutic adit on pivotal cytokines of bone metabolism in rheumatoid arthritis and osteoarthritis. Clin Rheumatol. 2016;35(11):2783–8.
Falkenbach A, Kovacs J, Franke A, Jorgens K, Ammer K. Radon therapy for the treatment of rheumatic diseases–review and meta-analysis of controlled clinical trials. Rheumatol Int. 2005;25(3):205–10.
Franke A, Franke T. Long-term benefits of radon spa therapy in rheumatic diseases: results of the randomised, multi-centre IMuRa trial. Rheumatol Int. 2013;33(11):2839–50.
Greinwald H. Gasteiner Kur: Therme und Heilstollen ; ein Ratgeber für Heilungssuchende und Gesunde. 1st ed. Badgastein: Badgastein: Krauth; 1986. p. 136.
Gastein Healing Gallery. https://www.gasteiner-heilstollen.com/en/heilstollen-therapy/healing-climate/. Accessed 1 Jan 2022.
Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–43.
Ludwig K, Graf von der Schulenburg JM, Greiner W. German Value Set for the EQ-5D-5L. Pharmacoeconomics. 2018;36(6):663–74.
Laxy M, Teuner C, Holle R, Kurz C. The association between BMI and health-related quality of life in the US population: sex, age and ethnicity matters. Int J Obes (Lond). 2018;42(3):318–26.
Gordeev VS, Maksymowych WP, Evers SM, Ament A, Schachna L, Boonen A. Role of contextual factors in health-related quality of life in ankylosing spondylitis. Ann Rheum Dis. 2010;69(1):108–12.
Levinsky M, Schiff M. Lifetime cumulative adversity and physical health deterioration in old age: Evidence from a fourteen-year longitudinal study. Soc Sci Med. 2021;289: 114407.
Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35(11):1095–108.
Luo N, Chew LH, Fong KY, Koh DR, Ng SC, Yoon KH, et al. Do English and Chinese EQ-5D versions demonstrate measurement equivalence? An exploratory study. Health Qual Life Outcomes. 2003;1:7.
van der Horst-Bruinsma IE, Zack DJ, Szumski A, Koenig AS. Female patients with ankylosing spondylitis: analysis of the impact of gender across treatment studies. Ann Rheum Dis. 2013;72(7):1221–4.
Thygesen LC, Ersbøll AK. When the entire population is the sample: strengths and limitations in register-based epidemiology. Eur J Epidemiol. 2014;29(8):551–8.
Sibthorp J, Paisley K, Gookin J, Ward P. Addressing Response-shift Bias: Retrospective Pretests in Recreation Research and Evaluation. J Leis Res. 2007;39(2):295–315.
Bodur H, Ataman S, Rezvani A, Bugdayci DS, Cevik R, Birtane M, et al. Quality of life and related variables in patients with ankylosing spondylitis. Qual Life Res. 2011;20(4):543–9.
Acknowledgements
We want to thank various people for their contribution to this study, especially Margret Schmid, Heike Thies, Roswitha Mayer, Christine Söllner and Claudia Pacher for organisational work. We are grateful for the assistance in data collection by Celina Ablinger, Julia Preishuber-Pflügl, Florentina Egger and Marlena Beyreis. We thank all physicians and medical technical assistants of Stiftung Kurtherme Badehospiz, Healing Gallery Bad Gastein, Cure and Rehabilitation Center Bad Hofgastein and Baerenhof Health Care & Rehabilitation Center for their assistance during this project.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
AvZ conceptualized the current study, conducted and interpreted the analyses, wrote the initial draft of the manuscript and finalized its current version. VS; HD and JF prepared and organized the data before analysis, were involved in the conceptual framework and protocol for the original data collection and reviewed and critically commented on the manuscript. JU; WF; MK; SE and MO were involved in the recruitment of participants, reviewed and critically commented on the manuscript. MR, BH and MG were involved in the concept of the current study and the design for the original data collection, reviewed and critically commented on the manuscript. All authors agreed on the final version before submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the County of Salzburg (No 415–E/1966/3–2015). All participants provided informed consent prior to their participation. The conduct of the study, the acquisition, provision and analyses of data in this study are in agreement with the European General Data Protection Regulation 2018 and in accordance with the Declaration of Helsinki.
Consent for publication
N/A
Competing interest
The authors have no conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
van der Zee-Neuen, A., Strobl, V., Dobias, H. et al. Sustained improvements in EQ-5D utility scores and self-rated health status in patients with ankylosing spondylitis after spa treatment including low-dose radon – an analysis of prospective radon indication registry data. BMC Musculoskelet Disord 23, 743 (2022). https://doi.org/10.1186/s12891-022-05691-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05691-1