
Abstract
Background
To compare potential of ultrashort time-to-echo (UTE) T2* map** and T2* values from T2*-weighted imaging for assessing lumbar intervertebral disc degeneration (IVDD),with Pfirrmann grading as a reference standard.
Methods
UTE-T2* and T2* values of 366 lumbar discs (L1/2-L5/S1) in 76 subjects were measured in 3 segmented regions: anterior annulus fibrosus, nucleus pulposus (NP), and posterior annulus fibrosus. Lumbar intervertebral discs were divided into 3 categories based on 5-level Pfirrmann grading: normal (Pfirrmann grade I),early disc degeneration (Pfirrmann grades II-III), and advanced disc degeneration (Pfirrmann grades IV-V). Regional differences between UTE-T2* and T2* relaxometry and correlation with degeneration were statistically analyzed.
Results
UTE-T2* and T2*value correlated negatively with Pfirrmann grades (P < 0.001). In NP, correlations with Pfirrmann grade were high with UTE-T2* values (r = − 0.733; P < 0.001) and moderate with T2* values (r = -0.654; P < 0.001). Diagnostic accuracy of detecting early IVDD was better with UTE-T2* map** than T2* map** (P < 0.05),with receiver operating characteristic analysis area under the curve of 0.715–0.876.
Conclusions
UTE-T2* relaxometry provides another promising magnetic resonance imaging sequence for quantitatively evaluate lumbar IVDD and was more accurate than T2*map** in the earlier stage degenerative process.
Similar content being viewed by others

Introduction
Low back pain (LBP) is a leading cause of disability worldwide, placing a great burden on the global health care system [1, 2]. Intervertebral disc (IVD) degeneration (IVDD) is a significant contributor to nonspecific LBP, with a lifetime prevalence of over 80% [3, 4].
Early stages of IVDD are mainly in the form of biochemical changes, including proteoglycan (PG) reduction, dehydration, and collagen degeneration. It will lead to a decrease in hydrostatic pressure, resulting in nucleus pulposus (NP) dehydration and loss of the structural and mechanical properties of the IVDs. In advanced stages of IVDD, along with loss of hydration and the subsequent drop in disc pressure, IVD height decreases under load [5,6,7,8,9]. These degenerative changes are accompanied by structural lesions, such as disc herniation, causing LBP, neurogenic claudication, and even cauda equina syndrome. At this stage, treatment strategy is limited to conservative treatment alone or surgical excision [10]. Early detection of alterations in IVDD is important for develo** preventative strategies or reestablishing degenerated IVDs, such as gene therapy, stem cell therapy, and growth factor therapy [11,12,13].
Conventional magnetic resonance imaging (MRI) is widely used for morphologic, qualitative assessment of IVDD in the clinical workup. Lumbar IVDD is commonly scored using the Pfirrmann grading system, which is based on the assessment of structure and loss of the signal intensity on T2-weighted imaging (T2WI). This grading system provides a standardized and reliable assessment of MRI disc morphology, but cannot detect early degeneration of IVDs characterized by a loss of PG quantitatively [14, 15].
Several quantitative MRI techniques to evaluate IVD degeneration objectively have been reported, such as diffusion-weighted imaging, diffusion tensor imaging, glycosaminoglycan chemical exchange saturation transfer, sodium, delayed gadolinium-enhanced MRI, T2/T2*, and T1rho map**. Previous studies have demonstrated that T2* map** could be quantitative imaging biomarkers for evaluating the biochemical state of the discs and correlating that with histology, water content, and degeneration [16].
Ultrashort time-to-echo (UTE) imaging as a novel MRI technique has the capacity to catch very short T2* signals (0.008 ~ 0. 50 ms) [17,18,19,20], It has been confirmed to be sensitive to changes in the deep tissue matrix and to subtle and even preclinical degeneration [21]. To date, UTE-T2* imaging has been reported to be a reliable tool for quantitative assessment of the biochemical changes of short T2 tissues, including tendon, cartilage, and ligament, etc. [20,21,22,23,24,25]. However, to the best of our knowledge, studies on UTE-T2* quantitative technique in evaluating IVDD are scarce. We hypothesized that quantitative UTE-T2* map** is capable of revealing degenerative changes in the discs.
The present study aimed to assess whether lumbar IVDD can be evaluated using UTE-T2* map** and to compare the potential of UTE-T2*and T2* values in the diagnosis of early IVDD.
Materials and methods
Subjects
Ethics approval for this study was provided by the ethics commission of the Fudan University Affiliated Zhongshan Hospital **. T2WI images were used for Pfirrmann grading. Detailed acquisition parameters were assigned to T2WI, UTE-T2* map**, and T2* map**.
For T2WI, repetition time (TR)/echo time (TE) = 2500/120 ms, slice thickness/gap = 5/0.5 mm, field of view (FOV) = 300 × 300 mm, matrix = 256 × 192, and bandwidth = 41.7 kHz. For UTE-T2* map**, TR = 112.4 ms, TE = 0.032/3.8/8.8/13.2 ms, slice thickness/gap = 3/0.5 mm, flip angle = 15, FOV = 300 × 300 mm, matrix = 300 × 256, and bandwidth = 62.5 kHz. Maps of the T2* was calculated using R2*(R2* = 1/T2*) [26, 27].For R2* map**, TR = 12.5 ms, TE = 1.40 /2.29 /3.18/4.07/ 4.96/5.85/ 6.74 / 7.63 / 8.52 ms, slice thickness/gap = 5/0 mm, flip angle = 5, FOV = 300 × 300 mm, matrix = 256 × 192, and bandwidth = 111.1 kHz.
Image analysis
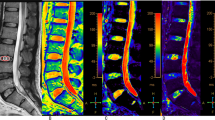
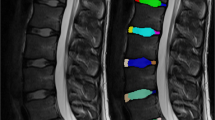
All lumbar IVDs were evaluated by 2 musculoskeletal radiologists each with more than six years of experience using T2WI and assigned a Pfirrmann grade (Table 1) [28]. Disc degenerations also were divided into three categories [11]: normal (Pfirrmann grade I), early disc degeneration (Pfirrmann grade II-III), and advanced disc degeneration (Pfirrmann grade IV-V). UTE-T2* values were calculated by mono-exponential fitting using custom code in MATLAB (MathWorks, Natick, MA). Five circular regions of interest (ROIs) of equal size were manually drawn on the midline slice of sagittal UTE-T2* and T2* map**s from anterior to posterior (Fig. 1), including the anterior annulus fibrosus (AAF; ROI 1), nucleus pulposus (NP; ROI 2–4), and posterior annulus fibrosus (PAF; ROI 5) [29].

MR images of the lumbar spine of a 39-year-old woman. Every lumbar IVD was cut into 5 uniform parts in each UTE-T2* and T2* map**. An ROI of 1 represented AAF, ROI 2–4 represented NP, and ROI 5 represented PAF. IVD, intervertebral disc; NP, nucleus pulposus; PAF, posterior annulus fibrosus; ROI, region of interest; UTE, ultrashort time-to-echo
Statistical analysis
Statistical analysis was conducted using SPSS 22.0 software (IBM, Armonk, NY) and Medcalc 20.022 (Mariakerke, Belgium). The Kruskal–Wallis test was performed to determine differences among the 5-level Pfirrmann grades. The differences between the two methods were expressed using the ± 95% confidence intervals (CIs) from the Bland–Altman analysis. Correlations of quantitative values with Pfirrmann grades were analyzed using Spearman's rank correlation. Receiver operating characteristic (ROC) analysis was performed and area under the curve (AUC), sensitivity, specificities, positive likelihood ratio (+ LR), and negative likelihood ratio (− LR) were obtained to assess the diagnostic efficacy of each quantitative parameter for differentiating normal IVDs from early disc degeneration and to differentiate early disc degeneration from advanced disc degeneration. AUCs were compared using the DeLong method [30]. A P value less than 0.05 was considered statistically significant.
Results
Clinical characteristics
Seventy-six subjects aged 54.4 ± 15.7 years (range, 19–85 years) were recruited into this study. They included 29 males (aged 51.8 ± 17.2 years; range, 19–82 years) and 47 females (aged 54.5 ± 14.9 years; range, 27–85 years). Five intervertebral discs (L1/L2–L5/S1) per subject were examined, of which 14 discs were excluded due to previous vertebral fusion operation (n = 2), collapsed disc space (Pfirrmann grade V) that made it impossible to measure the quantitative values (n = 9), and image quality problems (n = 3). A total of 366 IVDs were included in this study.
Using the Pfirrmann grading system, 73 discs were categorized as grade I; 110 discs, as grade II; 164 discs, as grade III; and 19 discs, as grade IV. The flowchart for the enrollment of the study population is presented in Fig. 2. The distribution of the UTE-T2*and T2* values with respect to Pfirrmann grades is provided in Table 2.

Flow diagram of the study enrolment discs
Correlation of UTE-T2*and T2* values with Pfirrmann grades
The Kruskal–Wallis test demonstrated that all quantitative values for all segments were significantly different among different Pfirrmann grades (Table 2). Bland–Altman plots are shown in Fig. 3. There was no significant bias between UTE-T2*and T2* values in NP and PAF(P > 0.05).UTE-T2* values showed high correlations with Pfirrmann grade in NP (r = − 0.733; P < 0.001). Moderate correlations with Pfirrmann grade were observed in T2* value of NP (r = -0.654; P < 0.001). Comparing the Spearman correlation coefficient, the highest correlation value was seen in NP and the lowest was seen in AAF. Among those, the UTE-T2* value of NP showed the highest correlation values with Pfirrmann grades. Results of Spearman's correlation analysis are summarized in Fig. 4.

Bland–Altman plots comparing both UTE-T2* and T2* values of AAF, NP, PAF. Bias (solid line) and limits of agreement (dashed line) are shown for each variable. The mean score is plotted on the x-axis, while the difference between the two methods is plotted on the y-axis (mean difference ± 1.96 SD). AAF, anterior annulus fibrosus; NP, nucleus pulposus; PAF, posterior annulus fibrosus

Scatter plots of the values in AAF, NP, and PAF according to the Pfirrmann grades. a, c, and e are respectively UTE-T2* relaxation time of AAF, NP, and PAF correlated with disc degeneration grading; b, d, and f are respectively T2* value of AAF, NP, and PAF correlated with disc degeneration grading
Post hoc multiple comparisons among each Pfirrmann grades
There were significant differences in UTE-T2* values of NP and PAF between each Pfirrmann grade. T2* values were found to be significantly different between Pfirrmann grade II and grade III in AAF, NP, and PAF (Fig. 5).

Post hoc multiple comparisons among 4 Pfirrmann grades. There were significant differences in UTE-T2* values of NP and PAF between each Pfirrmann grades. T2* values were found to be significantly different between Pfirrmann grades II and III in AAF, NP, and PAF. *P values of < 0.05 and **P values of < 0.001 were considered statistically significant. NP, nucleus pulposus; PAF, posterior annulus fibrosus; UTE, ultrashort time-to-echo
Diagnostic performance of UTE-T2* and T2* values in distinguishing each degeneration groups
ROC curves of UTE-T2* and T2* values for distinguishing each degeneration groups are plotted in Fig. 6 The corresponding diagnostic test characteristics are provided in Table 3. The AUC values of UTE-T2* map** in AAF, NP, and PAF were 0.715,0.876,0.787, respectively, for identification of the early disc degeneration, and 0.726,0.893,0.804, respectively, for identification of the advanced disc degeneration. The AUC values of T2* map** in AAF, NP, and PAF were 0.620, 0.763, 0.670, respectively, for identification of the early disc degeneration, and 0.570, 0.842, 0.720, respectively, for identification of the advanced disc degeneration.

Receiver operating characteristic (ROC) analysis. Graphs show ROC curves to distinguish each degeneration groups. Numbers are areas under the curves with 95% confidence intervals in parentheses
For pairwise comparisons of ROC curves, UTE-T2* values in NP and PAF were better in identifying early degeneration IVDs than those in T2*. There were no significant differences among UTE-T2* and T2* map** in AAF. Comparing between different segments, diagnostic performance of NP was the highest in predicting the early degeneration IVDs, AAF and PAF performed similarly. For differentiating early and advanced disc degeneration, the UTE-T2* value of PAF was better than that of T2* and there were no significant differences among UTE-T2* and T2* map** in AAF and NP. Comparing between different segments, diagnostic performance of NP was better than AAF, AAF and PAF performed similarly in predicting the advanced disc degeneration.
Overall, the diagnostic efficacy of UTE T2* map** was better than that of T2* map** for evaluating IVDD, especially in NP. The results of this study demonstrated that the UTE-T2* value in NP showed high correlations with Pfirrmann grade (r = − 0.733; P < 0.001) and that AUCs for the assessment of the early disc degeneration (AUC 0.876) were significantly higher than those for T2*(AUC 0.763).
Discussion
This study is the first to investigate and compare the diagnostic efficacies of UTE-T2* and T2* map** in detecting IVDD in humans. The results may help to confirm the feasibility and specificity of UTE-T2* as an objective and quantitative tool to identify early degenerative changes of the disc and show promise for clinicians to modify the diagnostics and therapeutic management strategies more accurately.
Conventional MRI, such as the Pfirrmann scale with T2WI, was limited in detecting ultrastructural alterations of early IVDD. Early stages of disc degeneration include biochemical changes, such as a loss or reduction of PG content, which can ultimately lead to dehydration. T2 relaxation reflected the integrated environment of the IVD, including water, protein, collagen, and other solutes [31], and was sensitive to water content and the composition of the collagen network structure. Researchers have reported that T2* relaxation time showed a good correlation with PG and collagen contents in 18 humans cadaveric IVDs [32]. Our findings confirmed an increase in the quantitative T2* values between the AAF and NP and a decrease between the NP and the PAF. In line with an earlier report [33, 34],T2 and T2* map** provided roughly similar results. The inverse correlation of the T2 relaxation time in the disc with Pfirrmann grade has been reported by Welsch et al. [35] and Noebauer et al. [36], the early study reported a low-to-moderate correlation between Pfirrmann grades and T2 relaxation times, which were consistent with the Spearman's correlation coefficient between Pfirrmann grades and T2*value in our results. Both T2 and T2* map** differ in the biochemical sensitivity of disc tissue, with T2 map** being sensitive to tissue hydration, while T2* map** being more sensitive to changes in tissue integrity [35].T2* map** provide more valuable biochemical information on the IVDs ultrastructure, together with three-dimensional acquisition capability and higher spatial resolution in a short scan time [37].
UTE-T2* map** was acquired using different echo times in the short (1–10 ms) and ultrashort echo time range [19, 22]. Because UTE-T2* map** can catch the short T2* relaxations from tissues, it is more sensitive to biochemical collagen matrix changes compared with conventional MRI techniques, based on histologic standards [19].
Multiple large general-population–based studies have proved that UTE-T2* map** can detect cartilage subsurface matrix changes, which can be indicative of reduced cartilage health from injury or early degeneration noninvasively [20, 23, 25]. Similar to the results reported by Detiger et al. [16], we observed a trend of decreasing UTE-T2* value with increasing degree of degeneration. The previous study revealed a significant correlation between T2* relaxation time and glycosaminoglycans (GAG) content in the nucleus pulposus, as well as histologic scoring with varying grades of degeneration [16]. During the aging process, the quantity and quality of PG and collagen contents diminish, along with a decrease in short T2* signal accordingly [21, 25, 34, 38]. T2* relaxometry appeared to be sensitive to water and PG contents. This may be the initial step in the degenerative cycle [25, 34, 38], which could be the underlying reasons for the decreased UTE-T2* and T2* value.
In NP and PAF, UTE-T2* map** showed significantly higher diagnostic accuracy in differentiating early disc degeneration from normal than did T2*. Theoretically, both UTE-T2* and T2* map** measured the T2* value of the tissue. UTE MRI technique mitigates the rapid signal loss from short T2* by reducing the TE to the scale of 0–200 microseconds to sample the free induction decay as early as possible. With considerably shorter TEs (0.032 ms in this study) than T2*, UTE-T2*map** allows signals from very short T2 components to be detected [23]. Thus, UTE-T2*map** is less sensitive to the magic angle effect and more sensitive to water protons and their local environment, making it a satisfactory method for evaluating disc generation. Because T2* relaxation time has been reported to reflect both the water content and PG content reduction [16], it is not hard to understand why the UTE-T2* value has better diagnostic accuracy than T2* for differentiating early disc degeneration.
Previous studies have reported that T2 relaxation time of Pfirrmann grades IV is significantly shorter than Pfirrmann grades III, and no significant differences were found between Pfirrmann grades IV and V, both of which show extremely low signal intensity [39]. The results of our study showed that compared to T2* values, UTE-T2* values conveyed significantly higher diagnostic performance in distinguishing the early disc degeneration from the advanced in PAF. Takashima et al. [40] reported that short T2* relaxation times with UTE are promising for assessing progressive IVD degeneration with poor water content, such as fibrosis change of IVDD with short T2 relaxation time. Our results are consistent with those findings quantitatively. Takashima et al. did not further discuss the quantitative evaluation of the early disc degeneration because their study population did not include grade I IVDs. Our results would appear to complement and refine their research.
A previous report on healthy ovine IVDs demonstrated that the T2 values show regional variation in discs and reported that high T2 values were observed in NP and low T2 values in the AAF and PAF when histologically evaluated [41]. Disc degeneration is believed to originates in NP with depletion of GAG, followed by a reduction in water content [5, 42]. Similar to previous reports, our study showed that correlations with Pfirrmann grade and UTE-T2* and T2* values were highest in NP and lowest in AAF. Our results also showed that NP had the highest diagnostic accuracy in predicting the early degeneration IVDs, while AFP and PFP were similar in predicting the early degeneration IVDs. These results suggest that the destruction of hydrophilic GAGs within NP was the main cause of the accumulation of cleaved extracellular matrix fragments with disc aging [16].
There were some limitations in this study. First, our study had no detailed histologic confirmation associated with IVDD changes. This is hard to achieve in humans. In addition, the relationship between T2* values and biochemical changes in IVDD has been previously established in human cadaveric lumbar discs [32]. Second, we were unable to compare the related clinical symptoms with the degree of degeneration in MRI quantitative parameters. Future research is warranted to explore these ideas. Third, no patient in this study showed grade V IVDs because grade V IVDs tend to have a collapsed disc space or a vacuum phenomenon, which is unable to measure the quantitative values due to susceptibility artifacts. If the complete grade V IVDs data set were available, quantitative evaluation of advanced IVD degeneration could be closer to reality. However, as our principal purpose was to detect early disc degeneration, the impact of incomplete grade V IVDs dataset on our results is within acceptable limits.
Conclusions
We demonstrated that UTE-T2*map** was more accurate than T2* map** in quantitatively diagnosing early intervertebral disc degeneration. In particular, UTE-T2* map** allowed for precisely distinguishing disc degeneration, potentially providing a promising imaging biomarker with potential applications in intervertebral disc degeneration for the emerging cell-based therapies.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LBP:
-
Low back pain
- IVD:
-
Intervertebral disc
- IVDD:
-
Intervertebral disc degeneration
- PG:
-
Proteoglycan
- NP:
-
Nucleus pulposus
- T2WI:
-
T2-weighted imaging
- UTE:
-
Ultrashort time-to-echo
- TR:
-
Repetition time
- TE:
-
Echo time
- FOV:
-
Field of view
- PAF:
-
Posterior annulus fibrosus
- AAF:
-
Anterior annulus fibrosus
- ROI:
-
Region of interest
- ROC:
-
Receiver operating characteristic
References
Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical approach for primary care. Med J Aust. 2017;206:268–73. https://doi.org/10.5694/mja16.00828.
Ogon I, et al. Imaging diagnosis for intervertebral disc. JOR Spine. 2020;3: e1066. https://doi.org/10.1002/jsp2.1066.
Liao Z, et al. Exosomes from mesenchymal stem cells modulate endoplasmic reticulum stress to protect against nucleus pulposus cell death and ameliorate intervertebral disc degeneration in vivo. Theranostics. 2019;9:4084–100. https://doi.org/10.7150/thno.33638.
Bashkuev M, Reitmaier S, Schmidt H. Relationship between intervertebral disc and facet joint degeneration: a probabilistic finite element model study. J Biomech. 2020;102:109518. https://doi.org/10.1016/j.jbiomech.2019.109518.
Zeng F, et al. A comparative study of diffusion kurtosis imaging and T2* map** in quantitative detection of lumbar intervertebral disk degeneration. Eur Spine J. 2019;28:2169–78. https://doi.org/10.1007/s00586-019-06007-z.
Griffith JF, et al. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine (Phila Pa 1976). 2007;32:E708-712. https://doi.org/10.1097/BRS.0b013e31815a59a0.
Menezes-Reis R, et al. Lumbar intervertebral discs T2 relaxometry and T1ρ relaxometry correlation with age in asymptomatic young adults. Quant Imaging Med Surg. 2016;6:402–12. https://doi.org/10.21037/qims.2016.08.01.
Wang F, et al. A histocytological and radiological overview of the natural history of intervertebral disk: from embryonic formation to age-related degeneration. Eur Spine J. 2019;28:633–48. https://doi.org/10.1007/s00586-019-05903-8.
Yang B, Wendland MF, O’Connell GD. Direct quantification of intervertebral disc water content using MRI. J Magn Reson Imaging. 2020;52:1152–62. https://doi.org/10.1002/jmri.27171.
Gugliotta M, et al. Surgical versus conservative treatment for lumbar disc herniation: a prospective cohort study. BMJ Open. 2016;6:e012938. https://doi.org/10.1136/bmjopen-2016-012938.
Wu, PH., Kim, HS. & Jang, IT. 2020 Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int J Mol Sci 21. https://doi.org/10.3390/ijms21062135.
Tong W, et al. Cell therapy for the degenerating intervertebral disc. Transl Res. 2017;181:49–58. https://doi.org/10.1016/j.trsl.2016.11.008.
Roh, EJ. et al. 2021. Genetic Therapy for Intervertebral Disc Degeneration. Int J Mol Sci 22. https://doi.org/10.3390/ijms22041579
Zobel BB, et al. T1ρ magnetic resonance imaging quantification of early lumbar intervertebral disc degeneration in healthy young adults. Spine (Phila Pa 1976). 2012;37:1224–30. https://doi.org/10.1097/BRS.0b013e31824b2450.
Togao O, et al. A qualitative and quantitative correlation study of lumbar intervertebral disc degeneration using glycosaminoglycan chemical exchange saturation transfer, pfirrmann grade, and T1-ρ AJNR. Am J Neuroradiol. 2018;39:1369–75. https://doi.org/10.3174/ajnr.A5657.
Detiger SE, et al. MRI T2* map** correlates with biochemistry and histology in intervertebral disc degeneration in a large animal model. Eur Spine J. 2015;24:1935–43. https://doi.org/10.1007/s00586-014-3498-1.
Chang EY, Du J, Bae WC, Chung CB. Qualitative and quantitative ultrashort echo time imaging of musculoskeletal tissues. Semin Musculoskelet Radiol. 2015;19:375–86. https://doi.org/10.1055/s-0035-1563733.
Du J, Takahashi AM, Chung CB. Ultrashort TE spectroscopic imaging (UTESI): application to the imaging of short T2 relaxation tissues in the musculoskeletal system. J Magn Reson Imaging. 2009;29:412–21. https://doi.org/10.1002/jmri.21465.
Chang EY, Du J, Chung CB. UTE imaging in the musculoskeletal system. J Magn Reson Imaging. 2015;41:870–83. https://doi.org/10.1002/jmri.24713.
Qiao Y, et al. UTE-T2(⁎) analysis of diseased and Healthy achilles tendons and correlation with clinical score: an in vivo preliminary study. Biomed Res Int. 2017;2017:2729807. https://doi.org/10.1155/2017/2729807.
Chu CR, et al. Quantitative magnetic resonance imaging UTE-T2* map** of cartilage and meniscus healing after anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42:1847–56. https://doi.org/10.1177/0363546514532227.
** of tendon healing after arthroscopic rotator Cuff repair: a longitudinal study. Am J Sports Med. 2020;48:2677–85. https://doi.org/10.1177/0363546520946772.
Yang J, et al. Quantitative ultrashort echo time magnetization transfer (UTE-MT) for diagnosis of early cartilage degeneration: comparison with UTE-T2* and T2 map**. Quant Imaging Med Surg. 2020;10:171–83. https://doi.org/10.21037/qims.2019.12.04.
Williams AA, Titchenal MR, Do BH, Guha A, Chu CR. MRI UTE-T2* shows high incidence of cartilage subsurface matrix changes 2 years after ACL reconstruction. J Orthop Res. 2019;37:370–7. https://doi.org/10.1002/jor.24110.
Titchenal MR, et al. Cartilage subsurface changes to magnetic resonance imaging UTE-T2* 2 years after anterior cruciate ligament reconstruction correlate with walking Mechanics associated with knee osteoarthritis. Am J Sports Med. 2018;46:565–72. https://doi.org/10.1177/0363546517743969.
Ogawa S, et al. Functional brain map** by blood oxygenation level-dependent contrast magnetic resonance imaging. A comparison of signal characteristics with a biophysical model. Biophys J. 1993;64:803–12. https://doi.org/10.1016/s0006-3495(93)81441-3.
Kühn JP, et al. Proton-density fat fraction and simultaneous R2* estimation as an MRI tool for assessment of osteoporosis. Eur Radiol. 2013;23:3432–9. https://doi.org/10.1007/s00330-013-2950-7.
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976). 2001;26:1873–8. https://doi.org/10.1097/00007632-200109010-00011.
Mok GSP, et al. Comparison of three approaches for defining nucleus pulposus and annulus fibrosus on sagittal magnetic resonance images of the lumbar spine. J Orthop Translat. 2016;6:34–41. https://doi.org/10.1016/j.jot.2016.02.003.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Chai JW, Kang HS, Lee JW, Kim SJ, Hong SH. Quantitative analysis of disc degeneration using axial T2 map** in a percutaneous annular puncture model in rabbits. Korean J Radiol. 2016;17:103–10. https://doi.org/10.3348/kjr.2016.17.1.103.
Ellingson AM, Nagel TM, Polly DW, Ellermann J, Nuckley DJ. Quantitative T2* (T2 star) relaxation times predict site specific proteoglycan content and residual mechanics of the intervertebral disc throughout degeneration. J Orthop Res. 2014;32:1083–9. https://doi.org/10.1002/jor.22633.
Cui YZ, Yang XH, Liu PF, Wang B, Chen WJ. Preliminary study on diagnosis of lumbar disc degeneration with magnetic resonance T1p, T2 map** and DWI quantitative detection technologies. Eur Rev Med Pharmacol Sci. 2016;20:3344–50.
Imanishi T, Akeda K, Murata K, Sudo A. Effect of diminished flow in rabbit lumbar arteries on intervertebral disc matrix changes using MRI T2-map** and histology. BMC Musculoskelet Disord. 2019;20:347. https://doi.org/10.1186/s12891-019-2721-y.
Welsch GH, et al. Parametric T2 and T2* map** techniques to visualize intervertebral disc degeneration in patients with low back pain: initial results on the clinical use of 3.0 Tesla MRI. Skeletal Radiol. 2011;40:543–51. https://doi.org/10.1007/s00256-010-1036-8.
Noebauer-Huhmann IM, et al. Sodium MR imaging of the lumbar intervertebral disk at 7 T: correlation with T2 map** and modified Pfirrmann score at 3 T–preliminary results. Radiology. 2012;265:555–64. https://doi.org/10.1148/radiol.12111920.
Liang X, et al. Feasibility study for evaluating lumbar intervertebral disc degeneration using histogram analysis of T2* values. Eur Spine J. 2020;29:2600–8. https://doi.org/10.1007/s00586-020-06476-7.
Ishikawa T, et al. Evaluation of lumbar intervertebral disc degeneration using T1rho and T2 magnetic resonance imaging in a rabbit disc injury model. Asian Spine J. 2018;12:317–24. https://doi.org/10.4184/asj.2018.12.2.317.
Takashima H, et al. Correlation between T2 relaxation time and intervertebral disk degeneration. Skeletal Radiol. 2012;41:163–7. https://doi.org/10.1007/s00256-011-1144-0.
Takashima H, et al. Lumbar disc degeneration assessment using T2* relaxation time with ultra-short TE. Magn Reson Imaging. 2020;73:11–4. https://doi.org/10.1016/j.mri.2020.07.004.
Kolf A-K, et al. T2* map** of ovine intervertebral discs: normative data for cervical and lumbar spine. J Orthop Res. 2016;34:717–24. https://doi.org/10.1002/jor.23071.
Siemionow K, An H, Masuda K, Andersson G, Cs-Szabo G. The effects of age, sex, ethnicity, and spinal level on the rate of intervertebral disc degeneration. Spine. 2011;36:1333–9. https://doi.org/10.1097/BRS.0b013e3181f2a177.
Acknowledgements
The authors would like to thank patients from Fudan University Affiliated Zhongshan Hospital **amen Branch for their participation in the study.
Funding
The study received statutory funding from the Science and Technology Guided Project of Fujian Province, China( Grant No. 2019D025);no additional funding was received.
Author information
Authors and Affiliations
Contributions
Li-Heng Liu contributed to study design, Jian-Jun Zhou conceived and designed the study; Li-Lan Wu performed the study, analyzed the data and wrote the paper. Sheng-**ang Rao and Pu-Yeh Wu contributed to critical revisions of the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The subjects were informed of the study goals and test protocols before giving their signed informed consent for participation. The study protocol received approval from the Local Bioethics Committee (certificate of approval No. B2021-007) of the Fudan University Affiliated Zhongshan Hospital **amen Branch in Fujian (China) according to the principles and policies of the Declaration of Helsinki. All methods were performed in accordance with the relevant guidelines and regulations in the Ethics approval and consent to participate.
Consent for publication
Informed consent to publish was obtained from the participants for publication of the images.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, LL., Liu, LH., Rao, SX. et al. Ultrashort time-to-echo T2* and T2* relaxometry for evaluation of lumbar disc degeneration: a comparative study. BMC Musculoskelet Disord 23, 524 (2022). https://doi.org/10.1186/s12891-022-05481-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05481-9