
Abstract
Background
Health literacy is the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others, whether at home, at the workplace, in the community, marketplace, healthcare sector, or the political arena. The main aim of this project is to measure health literacy in the adult population living in the municipality of Leiria over the next 10 years. As secondary objectives it is intended to characterize anxiety and depression, metabolic risk and health behaviors in the same population and over the same period.
Methods
This is a prospective cohort study that collects data on HL, anxiety and depression, health characteristics, health behavior and sociodemographic data. The study population will be composed by adults (≥ 18 years old) who are non-institutionalized and living in private households in Leiria. The random sample is stratified by gender and age groups. A face-to-face interview will be conducted with the Computer Assisted Personal Interview at baseline. Follow-up will be carried out every 2 years via telephone call. The association between independent variables and health literacy is examined by means of variance analysis with measurement repetition, and taking into consideration follow-up.
Discussion
The LiSa project is a population-based study, derived from a random sampling technique that will allow the analysis of health outcomes in a representative sample of the population of the municipality of Leiria. The LiSa study will be a valuable resource for epidemiological research, as it will provide fundamental information to improve public health policies regarding health literacy in Portugal.
Trial registration
Clinical trials: NCT05558631 (registered on 26/09/2022).
Similar content being viewed by others

Background
According to the World Health Organization (WHO), health is considered “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” [1]. Currently, health constitutes an essential axis of development that crosses and involves all sectors of activity, implying the dissemination of health as policies and the active participation of all citizens.
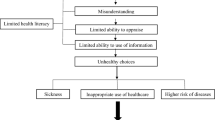
Health literacy (HL) is a topic that has been gaining increasing importance over the last few decades [2]. HL involves the knowledge, motivation and skills to access, understand, evaluate and apply health information in ways which promote and maintain good health [3]. Citizens with a higher level of HL find it easier to make everyday decisions related to healthcare, disease prevention, and health promotion to maintain or improve quality of life [4]. In recent decades in Portugal, the promotion of citizens’ HL has been identified as the way to improve health care, emerging as a concern in the definition of health policies. This is because different studies have shown that an inadequate level of HL can have significant implications for health outcomes, the use of health services and, consequently, health spending [5].
Studies indicate that the incidence of mental illness is increasing, with anxiety and depression being among the most common illnesses in the community [6, 7]. Patients with depression typically experience symptoms of anxiety, and those with symptoms of anxiety also experience depression. It can be difficult to discriminate between these two conditions, however both depression and anxiety disorders require specific and appropriate treatment, as they are associated with significant morbidity and mortality [7].
The gap between individuals who need mental health care and those who receive appropriate care is also a concern, as up to 70% of individuals who need mental health treatment fail to access the services they need [8]. Barriers to access treatments include lack of access to services, the potential client’s limited overall understanding of therapy treatment, and the perception that therapy treatment is too demanding or not relevant to the presenting concerns. These barriers are directly related to (lack of) HL [9].
Given these issues, it is necessary educate about the disease, focusing on the individual drivers which enables empowering citizens with knowledge to make conscious and informed decisions about the promotion of individual and collective health.
In 2021, the Municipality of Leiria prepared the Municipal Health Strategy, a document that serves as a tool to guide the development of health policies and intervention strategies of the Municipality. The document’s SWOT analysis presented HL and mental health as one of the weaknesses in the municipality, while hypertension and diabetes were identified as the leading health problems [10]. The Municipal Health Strategy is a strategic document, aligned with the main documents in the health area, namely the National Health Plan [11] where one of the main objectives are the reduction of alcohol consumption and exposure to tobacco.
Thus arises the LiSa study, a cohort study in Leiria, where citizens will be the essential source of information. The main aim of this project is to measure health literacy in the adult population living in the municipality of Leiria over the next 10 years. Concurrently, it is intended to characterize anxiety and depression and metabolic risk in the same population and over the same period.
Methods
Study design
The study is being developed and implemented by a multidisciplinary, multicenter team (researchers, health professionals, designers, mayors, among others). It is a prospective, longitudinal, closed cohort study over the next ten years with five data collection points. The guidelines from observational studies in epidemiology (STROBE) were applied to the study design [12]. The first data collection (baseline) will be carried out through an individual door-to-door interview, with a pre-established route, while the remaining data collection points will be managed via telephone.
To account the expected loss of participants to follow-up over time, we interviewed experts in cohort studies and potential study participants with the intention of hel** and advising us in develo** the study design. For that we used service design methodologies, namely informal interviews, and user groups definition.
Study population
The study population will be composed by adults (≥ 18 years old) who are non-institutionalized and living in private households in Leiria. Exclusion criteria will be: residents in hospitals, nursing homes, military barracks, or prisons, and residents unable to speak Portuguese or with a complete inability to respond to the questionnaire, either directly or through a person living with them [13].
Sample size
Residents of the municipality of Leiria aged 18 years or more. A sample size of 4003 (2001 males and 2002 females) were determined. A random sample stratified by gender and age groups (18–29, 30–64, 65 or more), for a confidence level of 95% and margin of 5% error was computed, in this case the sample need to collect should be 2287 participants. However, from previous studies [14] it is known that there is a high dropout rate in longitudinal studies, reaching approximately 50% in the 3rd wave. As if pretending to make 5 waves, the sample was increased by 75%. In other words, considering a dropout rate of 75%, data from 4003 participants should be collected. See Table 1.
Recruitment phase: face-to-face interview
The team of interviewers that will carry out the baseline data collection will be composed of 32 interviewers. Prior to the start of the study, all participating interviewers will be trained, by Lisa team, to standardize procedures. This training will cover the study protocol, and topics related to coaching, study design, study characteristics, logistics, ethical and legal issues, sample selection methodology, interview procedures (exercises of roll-play) and software. Only the candidates that successfully do this training will be selected to the interviews face-to-face, to assure the quality of the data collection [15].
Interviewers must be motivated and know very well the study and its objectives. For that, an interviewer’s manual/guide was designed with all the details of the study. The interviewers are grouped in teams of four and the interviews will be done by two interviewers, a male and a female. In each team of four, there is an interviewer coordinator who will manage the interviewer teams (scheduling interviews, travel, etc.), manage conflicts that may arise and make sure that the interviewers’ interaction with the participants is carried out correctly and according to the script.
Data collection
At baseline a face-to-face interview will be conducted with the Computer Assisted Personal Interview (CAPI) system: all interviewers have a tablet with the software which will provide the questionnaire. The questionnaire was designed by LiSa’s research team. Both the survey and software performance were tested in a small sample of subjects, and results validated by the LiSa research team before being used by the interviewers. It is estimated it will take approximately 30 min to complete the survey.
Since there is no reliable list of households in Portugal, a random selection of points in the map of each location will be performed. Addresses will be selected, and afterwards the “random walks” will start. Interviewers will register each selected address and, if someone is at home, they will collect information on age and gender of the different people living in that address, and will give information about the study. After validation of the selected address and inhabitants, the interviews will be scheduled, or if the person is available will be immediately asked to answer the questionnaire. In order to assure the successful data collection, up to three visits to each address (one during the weekend) will be made [13]. At each address, the person whose birthday is closest to the day of the visit (aged 18 years or older) will be selected for the interview.
Between February and April 2023, five interviewers conducted a pilot study, in the largest parish in the council, with the aim of testing the proposed methodology. Taking into account that data collection went well, we will maintain this data collection methodology and start the first data collection in February 2024.
Follow-up
The collection of new data will be carried out every 2 years via telephone call.
One of the approaches to mitigate the abandonment of participants (loss to follow-up) is to ensure good communication between the study team (interviewers, researchers, health professionals, designers, mayors) and cohort participants, using effective communication channels, updated, and provide quick feedback on health information to the participant.
The reasons why participants drop out of the study will be documented in order to analyze the bias of the study results.
Communication of the study
Communication about the LiSa study is very important, the population will more easily join the study if they know the objectives and long-term benefits of the study. Thus, population will learn about the LiSa study in several ways. Outdoors and advertising boards will be spread across the municipality. The screens at the city’s main hospital and health centers will have information about LiSa study. There will be LiSa’s flyers in the pharmacies, health units, coffees, bookstores, parish council and others public places. One week before the interviewers knock on people’s door, flyers will be distributed in the mailbox with dates and times when interviewers will walk in that area. The priests will also announce at Mass when the interviews will take place in that parish.
Variables under study
At baseline, HL, anxiety and depression, health characteristics (metabolic risk, auto-report chronic diseases, anthropometric variables), lifestyle habits (tobacco, alcohol, physical activity) and sociodemographic characteristics are collected from each participant.
Health literacy
HL will be measured through European Health Literacy Survey Questionnaire short-form version (HLS19-Q12). To measure HL in an adequate way for public health-oriented surveys of general population in Europe, the Health Literacy Survey (HLS-EU) was conducted in 2012 [16] using a new measurement tool developed from the conceptual model of Sørensen et al. [17]: the “47-item European Health Literacy Survey Questionnaire” (HLS-EU-Q47) [18]. HLS-EU was developed to measure HL in populations [18] based on a conceptual framework reflecting four information-processing dimensions (i.e., accessing, understanding, appraising, and applying) within three health domains (i.e., health care, disease prevention, and health promotion) [17]. Each item in the questionnaire assesses the perceived difficulty of a specific health-related task for the respondent. Since 47 items were excessively time-consuming for some HL researchers’ short forms have been validated in several languages to be used in the European Health Literacy Survey [4, 19, 20] The HLS19-Q12 was translated and validated in a previous study in Portuguese population [3]. The scale contains 12 items that measure HL. Each item assesses the perceived difficulty of completing a specific health-related task by asking “On a scale from very difficult to very easy, how easy would you say it is to [e.g, find information on symptoms of illnesses that concern you]?” Each item is rated on a 4-point Likert-type scale (1, very difficult; 2, fairly difficult; 3, fairly easy; 4, very easy). To correctly assess respondents’ health literacy, participants must answer at least 10 of the 12 questions. The general HL index (G-HL12) is calculated as follows: G-HL12 index = (mean − 1) x (50/3). Four levels of HL are defined: inadequate (0–25), problematic (25.1–33), adequate (33.1–42), and excellent (42.1–50) [21].
Anxiety and depression
To evaluate symptoms of anxiety and depression we applied the Hospital Anxiety and Depression Scale (HADS) Portuguese validated version [22]. The HADS was originally developed by Zigmond and Snaith [23] as a screening tool to apprehend clinically significant states of anxiety and depression in a non-psychiatric hospital setting. Individual anxiety and depression scores were calculated by summation of the appropriate seven items and thus can range from 0 to 21, with higher scores indicating higher levels of anxiety or depression, respectively. In both subscales, a score between 0 and 7 is “normal,” between 8 and 10 “mild,” between 11 and 14 “moderate,” and between 15 and 21 “severe” (idem). Presence of anxiety and depression symptoms was defined when HADS scale was ≥ 11, since Snaith suggested a score ≥ 11 was indicative of “caseness” to a mood disorder [24]. This scale is used in a lot of observational studies [14, 25].
Health characteristics
Metabolic risk is assessed by the Finnish Diabetes Risk Score-FINDRISC (FINDRISC). FINDRISC is a simple and practical tool originally designed in Finland to identify individuals at high risk of type 2 diabetes mellitus onset, without the need for laboratory tests [26, 27]. The score is based on eight easily identifiable parameters (age, body mass index, waist circumference, hypertension, physical activity level, diet, occurrence of previous hyperglycemia, and family history of diabetes) and provides a measure of the probability of develo** diabetes over the next 10 years. This score is being used in different European populations [28, 29].
Participants will be asked if they had been previously diagnosed with some chronic disease (high cholesterol level, high blood pressure, heart disease, diabetes, and pulmonary disease). Self-reported abdominal circumference, height and weight and based on these data, body mass index (BMI, weight/height2, in kg/m2) will be calculated and categorized according to the World Health Organization classification in four categories: underweight (BMI < 18.5 kg/m2), normal (BMI between 18.5 and 24.9 kg/ m2), overweight (BMI between 25 and 29.9 kg/m2), and obesity (BMI ≥ 30 kg/m2) [30].
Health related behavior
Health related behavior covers the following domains: alcohol intake (daily, occasionally, and never), consumption of fruits and vegetables, smoking habits, and physical activity.
Alcohol intake is measure by Alcohol Use Disorders Identification Test (AUDIT) developed by WHO, it is a simple and effective method of screening for unhealthy alcohol use, defined as risky or hazardous consumption or any alcohol use disorder [31].
Smoking habits (current smoker, past smoker, and never smoked) is accessed by Fagerström Test for Nicotine Dependence. This is a standard instrument for assessing the intensity of physical addiction to nicotine. The test was designed to provide an ordinal measure of nicotine dependence related to cigarette smoking. It contains six items that evaluate the quantity of cigarette consumption, the compulsion to use, and dependence [32, 33].
Study validity
Data collection forms will be further monitored centrally to check for missing data or inconsistencies, including potential participant telephone contact to confirm the answers. Also, a monthly analysis of the collected data will be carried out to monitor its quality. This statistical analysis will be carried out at different levels: by teams of interviewers, by locations, age groups and gender, to minimize errors in the data.
The data collected will be stored on a specific server with a high level of security.
Statistical analysis
Descriptive statistics will be computed to describe the baseline characteristics of the participants (gender, age, education and marital status). Normally distributed variables will be described by the mean and standard deviation. In the case of non-normal distributions, the data will be presented as median and interquartile range. For qualitative variables, absolute and relative frequencies will be calculated. At baseline comparisons between groups (e.g. with and without anxiety) will be undertaken using t-tests for continuous normally distributed variables or Wilcoxon for non-normally distributed variables. Chi-squared tests will be used for categorical variables, and Fisher’s Exact test will be used for categorical variables within smaller sample sizes.
Taking into consideration follow-up, the changes in HL will be evaluated by means of variance analysis with measurement repetition. After checking the statistical model pre-requisites, sociodemographic characteristics will be added by means of linear regression analysis in the final model.
For all calculations the level of statistical significance will be set to p < 0.05 and Stata software will be used.
Discussion
The HLS-EU revealed that 47.6% of respondents in Europe had limited HL (insufficient or problematic), which is reflected in almost half of the people surveyed [16]. The HLS-EU-PT presents itself as an adequate instrument to assess the level of HL of the Portuguese population, it was applied throughout the national territory, including the autonomous regions, through researchers from an academic network. The results revealed that 61% of the Portuguese population surveyed had a problematic or inadequate level of general HL [5]. This problem must be overcome, because at some point in our lives, we all need to be able to find, understand and use health information and services [34]. Low levels of HL are related to a lower ability to manage chronic diseases, greater number of hospitalizations, incorrect use of emergency services and infrequent use of preventive practices [35]. Considering the impact of HL levels on individual and collective health, on the use of health services and, consequently, on health spending, the development of diagnostic tools for the HL level of populations has become crucial [5, 36,37,38].
The LiSa study is a cohort study being implemented in Leiria by a multidisciplinary, multicenter team (epidemiologists, doctors, nurses, designers, mayors, among others) and aims to characterize HL in the adult population of the municipality of Leiria over the next 10 years, with measurements every 2 years. It is also intended to characterize the levels of anxiety and depression, metabolic risk, alcohol and smoking in the adult population, since these are problems very present in today’s society. Most of the existing studies that look for HL in Portugal are based on cross-sectional examinations [3, 5]. Longitudinal studies have advantages in terms of the quantity or quality of the data that collected, details of the life course, establishing the order in which events occurs and reduce recall bias.
The results of this study will be published in well-known international journals, conferences and congresses. Project’s data will be used in national and international dissertations on condition on referral to the cohort. The research results will be present to national decision-makers in oral and written form. The LiSa study has already been presented and announced to Leiria’s community and in the social media.
Data availability
The datasets used and/or analysed during LiSa study will be available from the corresponding author on reasonable request.
References
World Health Organization. Constitution of the World Health Organization. 2006.
Ishikawa H, Kiuchi T. Association of Health Literacy Levels between Family members. Front Public Health. 2019;7.
Arriaga M, Francisco R, Nogueira P, Oliveira J, Silva C, Câmara G, et al. Health Literacy in Portugal: results of the health literacy Population Survey Project 2019–2021. Int J Environ Res Public Health. 2022;19:4225.
Lorini C, Lastrucci V, Mantwill S, Vettori V, Bonaccorsi G, Florence Health Literacy Research Group. Measuring health literacy in Italy: a validation study of the HLS-EU-Q16 and of the HLS-EU-Q6 in Italian language, conducted in Florence and its surroundings. Ann Ist Super Sanita 55(1):10–8.
Pedro AR, Amaral O, Escoval A. Literacia em saúde, Dos Dados à ação: tradução, validação e aplicação do European Health Literacy Survey em Portugal. Revista Portuguesa De Saúde Pública. 2016;34(3):259–75.
Mirzaei M, Yasini Ardekani SM, Mirzaei M, Dehghani A. Prevalence of Depression, anxiety and stress among Adult Population: results of Yazd Health Study. Iran J Psychiatry. 2019;14(2):137–46.
Tiller JWG. Depression and anxiety. Med J Aust. 2013;199:S6.
Henderson C, Evans-Lacko S, Thornicroft G. Mental Illness Stigma, help seeking, and Public Health Programs. Am J Public Health. 2013;103(5):777–80.
Tambling RR, D’Aniello C, Russell BS. Mental Health Literacy: a critical target for narrowing racial disparities in behavioral health. Int J Ment Health Addict. 2021.
Câmara Municipal de Leiria. Estratégia Municipal de Saúde do Município de Leiria 2021/2023. 2021.
Freitas M da, G, Quitério M, de Garcia F, Felício AC, Matos MM, Martinho C et al. C,. Plano Nacional de Saúde 2021–2030. Direção-Ge. 2021.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of Observational studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–9.
Ramiro S, Canhão H, Branco JDC. EpiReumaPt Protocol - Portuguese epidemiologic study of the Rheumatic diseases. Acta Reumatol Port. 2010;35:384–90.
Dias SS, Rodrigues AM, Gregório MJ, de Sousa RD, Branco JC, Canhão H. Cohort Profile: the epidemiology of chronic diseases Cohort (EpiDoC). Int J Epidemiol. 2018;47(6):1741–j1742.
Gouveia N, Rodrigues AM, Ramiro S, Machado P, da Costa LP, Mourão AF et al. EpiReumaPt: how to perform a national population based study - a practical guide. Acta Reumatol Port 40(2):128–36.
Sørensen K, Pelikan JM, Röthlin F, Ganahl K, Slonska Z, Doyle G, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–8.
Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z et al. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health [Internet]. 2012;12(1):80. https://doi.org/10.1186/1471-2458-12-80.
Sørensen K, Van den Broucke S, Pelikan JM, Fullam J, Doyle G, Slonska Z et al. Measuring health literacy in populations: illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health [Internet]. 2013;13(1):948. https://doi.org/10.1186/1471-2458-13-948.
Nolasco A, Barona C, Tamayo-Fonseca N, Irles MÁ, Más R, Tuells J, et al. Alfabetización en salud: propiedades psicométricas del cuestionario HLS-EU-Q16. Gac Sanit. 2020;34(4):399–402.
Emiral GÖ, Aygar H, Atalay B, Balci S. Health literacy scale-european union-Q16: a validity and reliability study in Turkey. Int Res J Med Sci. 2018.
Pedro AR, Raposo B, Luís L, Amaral O, Escoval A, Simões Dias S. Portuguese version of the HLS-EU-Q6 and HLS-EU-Q16 Questionnaire: Psychometric Properties. Int J Environ Res Public Health [Internet]. 2023;20(4).
Pais-Ribeiro J, Silva I, Ferreira T, Martins A, Meneses R, Baltar M. Validation study of a Portuguese version of the hospital anxiety and Depression Scale. Psychol Health Med. 2007;12(2):225–7.
Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand [Internet]. 1983;67(6):361–70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Snaith RP, The Hospital Anxiety And Depression Scale. Health Qual Life Outcomes [Internet]. 2003;1(1):29. https://doi.org/10.1186/1477-7525-1-29.
de Sousa RD, Rodrigues AM, Gregório MJ, Branco JDC, Gouveia MJ, Canhão H et al. Anxiety and Depression in the Portuguese Older Adults: Prevalence and Associated Factors [Internet]. Vol. 4, Frontiers in Medicine. 2017. p. 196. https://www.frontiersin.org/article/https://doi.org/10.3389/fmed.2017.00196.
Lindström J, Tuomilehto J. The diabetes risk score. Diabetes Care. 2003;26(3):725–31.
Kulkarni M, Foraker RE, McNeill AM, Girman C, Golden SH, Rosamond WD, et al. Evaluation of the modified FINDRISC to identify individuals at high risk for diabetes among middle-aged white and black ARIC study participants. Diabetes Obes Metab. 2017;19(9):1260–6.
Dantas R, Azevedo T, Alves M, Balsa M, Albuquerque I, Ferreira M et al. Utilização do FINDRISC no Rastreio da Diabetes em Utentes Assintomático. Revista Portuguesa de Endocrinologia, Diabetes e Metabolismo. 2017;12(1):45–51.
Lindström J, Neumann A, Sheppard K, Gilis-Januszewska A, Greaves C, Handke U, et al. Take action to prevent diabetes – the IMAGE Toolkit for the Prevention of type 2 diabetes in Europe Toolkit for the Prevention of type 2 diabetes in Europe. Horm Metab Res. 2010;42(S 01):S37–55.
Physical status. The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452.
Saunders JB, Aasland OG, Babor TF, De La Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction [Internet]. 1993;88(6):791–804. https://doi.org/10.1111/j.1360-0443.1993.tb02093.x.
Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict. 1991;86 9:1119–27.
Pomerleau CS, Majchrzak MJ, Pomerleau OF. Nicotine dependence and the Fagerström Tolerance Questionnaire: a brief review. J Subst Abuse. 1989;1(4):471–7.
Juvinyà-Canal D, Suñer-Soler R, Boixadós Porquet A, Vernay M, Blanchard H, Bertran-Noguer C. Health Literacy among Health and Social Care University students. Int J Environ Res Public Health. 2020;17(7):2273.
Espanha R, Ávila P. Health literacy Survey Portugal: a contribution for the knowledge on Health and communications. Procedia Comput Sci. 2016;100:1033–41.
Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20(2):175–84.
Porr C, Drummond J, Richter S. Health Literacy as an empowerment Tool for low-income mothers. Fam Community Health. 2006;29(4):328–35.
Paasche-Orlow MK, McCaffery K, Wolf MS. Bridging the International Divide for Health Literacy Research. Patient Educ Couns. 2009;75(3):293–4.
Acknowledgements
The authors would like to thank to Professor Maria Pedro Guarino, coordinator of ciTechCare – Center for Innovative Care and Health Technology of Polytechnic of Leiria for all support of LiSa project.
Funding
This work was funded by Portuguese national funds provided by Fundação para a Ciência e Tecnologia (FCT) (UI/05704/2020) and Câmara Municipal de Leiria.
Author information
Authors and Affiliations
Contributions
SSD, RP, TG, CG, ESS, BA and MJB conceived and design the study, with contribution from AS and AV. The protocol manuscript was drafted by SSD, MJB and TG. All authors have contributed to the current manuscript through review and editing and have approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All study information will be obtained, stored, and analyzed in accordance with the General Data Protection Regulation (Regulation (EU) No. 679/2016, of 27 April), as well as the international requirements of Good Clinical Practice. All results will be published in a form that will not allow any individual participants to be identified (i.e., in tabular, aggregate form only). A participant ID number will be generated for all participants and stored with the data. The participant registration details will be stored separately in a secure password-protected folder. The data collected from the baseline and follow-up surveys will not contain any personally identifiable information, only,The participant ID number to allow survey responses to be linked.This study has been ethically approved by Politécnico de Leiria Ethics Committee (PARECER Nº CE/IPLEIRIA/33/2022). Before registration, all participants read and sign the written consent form. A copy of the signed consent form is given to the participant.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Batalha, M.J., Gabriel, T., Valentim, A. et al. Health literacy – study protocol for LiSa cohort study. BMC Public Health 24, 1737 (2024). https://doi.org/10.1186/s12889-024-19148-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19148-8