
Abstract
Background
Multisector activities are needed to prevent childhood obesity due to its multifactorial background. The first aim was to identify the activities that had been undertaken for obesity prevention and deduce their main targets. Second, we analyzed the public health policy approaches (upstream, midstream, and downstream) which were followed. Finally, we studied the perception of interviewees regarding their sectors’ roles in implementing the local obesity program.
Methods
Deductive content analysis was used to analyze semi-structured interviews with 34 key professionals (from seven administrative sectors) who had participated in multisector health promotion during 2009–2016 and five representatives of other core parties.
Results
Several midstream and upstream activities were targeted at making physical activity (PA) and healthy eating (HE) integral parts of children’s lifestyle. One long-term strategy was to create environments for PA accessible to every inhabitant and build and renovate the interiors and yards of schools and day-care centers. The healthiness of meals was increased progressively. In addition to midstream and upstream activities, as a downstream activity, an intervention targeting children at risk of obesity was implemented. The impact of management on the activities was considerable; childhood obesity prevention was included in the city strategy and systematically coordinated at the highest managerial level. Altogether, various sectors operated efficiently to promote obesity-preventing lifestyles; however, not all (important) sectors recognized their role in the multisector process.
Conclusion
Most of the activities to guide children towards obesity-preventing lifestyles were either at the midstream or upstream level. Among the latter, considerable work is aimed at creating opportunities to practice PA and making it a natural part of the daily life. The aim of familiarizing children with lifestyles that include PA and HE was shared across sectors, including sectors that had not yet acknowledged their role in obesity prevention. Strong support from city management and systematic coordination of the activity are important factors that contribute to the engagement of several administrative sectors in working towards a shared aim, such as the prevention of childhood obesity.
Similar content being viewed by others


Background
Obesity among children threatens human health and reduces life expectancy [1, 2]. In Finland, in 2018, 27% of 2–16-year-old boys and 18% of girls were overweight and 8 and 4% were obese, respectively [3]. Health problems caused by obesity may emerge during childhood [4, 5] and could lead to obesity in adulthood [5, 6].
Risk factors for childhood obesity interact in complex ways and genetic factors also play a role [5, 7]. The web of contributing factors operates at individual-, household-, community-, and wider societal levels [8, 9]. The individual-level factors that most strongly affect obesity risk include diet [10, 11], physical activity (PA) [10, 12], and sedentary behaviors [13, 14]. These lifestyle factors have been targets of preventive programs [8, 15,16,17].
The environments in which obesity-related behaviors are shaped include family, school, and day-care centers [18,19,20]. Children’s eating habits are influenced by the type of food available at their homes [21] and their PA depends on parental support [22]. Thus, the lifestyles of families should be targeted in the social contexts in which children live and grow [23,24,25]. In addition, physical living environments may influence energy intake, behavioral activities, and social norms related to lifestyle [26,27,28].
There are no simple means to prevent obesity because of its multifactorial background. Obesity prevention programs may be efficient (e.g., [17]); however, policy approaches and widening the spread of related activities in different sectors throughout society could increase the likelihood of longer-lasting effects [29,30,31]. Based on the knowledge of health determinants [32], public policies and environmental interventions have been found to promote healthy eating (HE) and PA [8, 16].
A framework is required to identify opportunities to prevent obesity at various societal levels. The Obesity Policy Action framework (OPA) by Sacks, Swinburn, and Lawrence [33] is based on a summarized understanding of policy researchers and public health practitioners on policy areas that could be involved. Obesity prevention policies refer to a system of laws, regulatory measures, courses of action, and funding priorities [33]. The framework is theoretically based on the socioecological model which combines the multiple levels on which the various health determinants [32] leading to obesity operate. Thus, the model forms a basis for comprehensive and systematically organized activity aimed at behavior changes among populations and their subgroups [33, 34]. When applying this model, three levels are often recognized. The macro- or society-level includes various public policies aimed at providing opportunities to make healthy lifestyle choices. The interpersonal level covers people’s social and cultural life spheres and communities. The biological and psychological characteristics of individuals play a role on the intrapersonal level. Furthermore, the components of each level interact; for example, personal characteristics may influence the way universally available public services are used [34].
Based on this theoretical model, the OPA framework suggests various instruments that can be used by policymakers to influence the entire population, its subgroups, or individuals. We organized the instruments according to three public health policy approaches. Representing the societal level of the socioecological model, the upstream approach includes policies that influence a wide range of social and economic circumstances, thus creating opportunities for obesity-preventing lifestyles. At the interpersonal or community level of the model, the midstream approach includes ways to influence a population’s behavior in everyday settings. At the intrapersonal level, the downstream approach consists of policy interventions, services, and strategies that offer treatment and support to individuals with obesity or at risk. It is possible to assess the extent to which the implemented activities follow each of these policy approaches by applying the OPA framework to a certain population (e.g., country, municipality). This helps the parties participating in the processes of obesity prevention to integrate policy actions, refine targets, and detect the need for further action [33]. In this study, activities to prevent obesity in the studied municipalities were compared against this model.
In the South Ostrobothnia province, childhood obesity has been a focus of health promotion since the development program for the prevention of type 2 diabetes in 2003–2008. At that time, awareness of obesity risk factors and lifetime consequences was raised among the public, management, and personnel in various administrative sectors [35]. A treatment path called “A Child’s and Adolescent’s Weight Path”, targeting children and parents at risk of obesity, was launched to be used in schools, day-care centers, health care facilities, and family settings [36]. Municipalities, non-governmental organizations (NGOs), and educational institutions participated in this process.
Partly because of this program, the city of Seinäjoki began to focus more on health promotion. Hiring a Director of Health Promotion in 2009 and setting up a health promotion management group, both operating at the city management level, were concrete signs of the beginning of a more systematic approach to the work done across sectors. From 2009 onwards, statistics indicated a significant decrease in the prevalence of overweight and obesity in Seinäjoki. In 2009, 8% of 1-year-olds were overweight or obese; in 2013, the proportion was only 5% and the figures did not increase until 2015. The figures for the 5-year-olds were 17 and 10% in 2009 and 2015, respectively, and did not increase until 2015. In 2011, 14% of 1st-grade students and 16% of 5th-grade students were overweight or obese. In 2013, the proportions were 11 and 16%, respectively; however, in 2015, the figures for the 1st grade and 5th grade students declined to 9 and 8%, respectively [37]. These statistics further boosted obesity prevention activities and emphasized the need to implement multisector cooperation.
We studied the contribution of various administrative sectors, as well as some key organizations, to childhood obesity prevention during 2009–2016. The specific questions were as follows: 1) Which activities did each sector undertake to promote healthy lifestyles, particularly those preventing obesity among children? 2) Which of the main public health policy approaches (upstream, midstream, and downstream) for health promotion and obesity prevention were followed? 3) How did the interviewees perceive their sectors’ roles in implementing the Overcoming Obesity Program?
Methods
Setting
The start of the study period was selected as the year 2009, when systematic health promotion started in Seinäjoki. Since our research started in 2016, the study period covered the years 2009–2016. In 2013, the city started participating in the National Obesity Program 2012–2018 [38], titled the Overcoming Obesity Program 2013–2020. Thus, the data collected in this study covered the years before the launch of the municipal program.
Study design and data collection
The informants were purposively selected by asking the persons coordinating the health promotion activity to name the key professionals in multisector health promotion between 2009 and 2016. The participants represented six administrative sectors. In addition, representatives from three core collaborative partners were interviewed to obtain important information about the process. One researcher contacted the interviewees by phone or e-mail between October and December 2016, inquiring about their interest in being interviewed. In total, 39 people were interviewed; one interview was a group interview with two people and two interviews were obtained as written documents (Table 1). Out of the people contacted, one person refused to participate in the study.
The semi-structured interview guide included the following: 1) job description; 2) sector-specific objectives for health promotion and childhood obesity prevention; 3) activities related to health promotion and disease prevention; 4) resources available for health promotion; 5) opinions regarding the visibility and success of health promotion activities and the Overcoming Obesity Program within the interviewee’s sector; and 6) thoughts about the future actions needed. The interviews lasted between 15 and 120 min and were usually conducted in the participant’s office. The interviews were recorded, transcribed verbatim (355 pages), and anonymized. The transcripts were not sent back to the participants for approval.
Analysis of the interviews
Deductive content analysis [39] was used to answer the research questions. First, three researchers read the transcribed interviews and one of them produced a detailed list of activities undertaken in each administrative sector, as proposed in the National Obesity Prevention Program’s checklist [40] (Table 1). Second, three researchers reviewed the findings and formulated shared opinions, which improved the study’s content validity. At this stage, the researchers organized the activities according to the main targets of increasing PA or HE, to support obesity prevention or promote health and/or well-being (Table 2). To summarize the activities, the core (Table 3) and key (Fig. 1) activities were presented for each sector. Third, a comparison was performed against the OPA framework [33] to interpret the health policy approaches (upstream, midstream, or downstream) followed in each sector (Table 4). Fourth, the responses to the question about the interviews’ perceptions of their sectors’ role in the implementation of the obesity program were analyzed.
Results
The activities to promote health and prevent childhood obesity according to their main targets
In the detailed list, the activities were organized according to their main targets (Table 2). It should be noted that no activity was part of a specifically funded intervention and was performed as a regular employee duty.
Table 3 summarizes the activities through which each of the four main targets were focused on. The cross-cutting target was to create environments in which PA could be practiced and become a natural part of children’s daily lives. For this purpose, day-care centers and schools built and renovated their premises and equipment was made available for games and play. National level activating programs were participated [47, 52] and even the youngest children and their parents were made aware of the national PA recommendations [48]. In some schools, the pupils and teachers were given roles as PA instructors and innovators. PA-weighted curricula were also used. The restructuring of the school day made longer break for activities, possible. Lectures were allowed to be paused for exercising. Information on opportunities regarding PA was distributed, and parents were encouraged to participate.
Sports and technical services constructed multipurpose and easily accessible premises for PA for all city inhabitants. Longstanding work in planning, building, and environmental maintenance by the technical services was done in collaboration with other sectors and NGOs, and citizens’ wishes were listened to. The restructuring of the city center aimed at creating an environment that would inspire PA and routes for light traffic were also constructed. Sports services hired PA instructors, introduced new forms of PA, and encouraged both children and adults to learn new skills. PA groups and events were organized in collaboration with other organizations and information about these matters was circulated. Targeted strategies ensured equal opportunities in PA for children with special needs.
The target of promoting HE was obvious in the mass catering services responsible for the supply of meals in day-care centers and schools. HE was also an important target in these educational sectors. National nutritional recommendations [49] and the criteria for heart-healthiness were followed for food preparation (https://www.sydanmerkki.fi/en/). The meals were regarded as opportunities for exploring new tastes and learning HE; this was also encouraged by specific campaigns [50]. Furthermore, all day-care centers were declared dessert-free and energy drinks were forbidden in all schools. Meal plans were also developed by committees that had representatives from the mass catering services and educational sectors. The professional skills of catering staff were maintained through continuous training. Important dietary advice to children and parents was provided by professionals in oral care, which is a part of primary health care.
The specific target of obesity prevention was visible at the city management level because it was included in the city strategy; furthermore, there was an obesity program operating in the city. In primary health care, systematic monitoring of the children’s height and weight was performed [45] and reported for the entire child population. A specific tool was used to help children at risk of obesity [36].
Much of the work targeted the overall promotion of health and/or well-being. This target was included in the city strategy at the managerial level, and the work done under the leadership of the Director of Health Promotion was supported by the mayor and the multisector health promotion management group. Scientific evidence and previous experience formed the basis for the activities. The guidelines of the national health promotion programs were followed to develop the structures and objectives of the work. This meant that the Health in All Policies approach was applied [41]. The sectors were strongly committed to the action and collaborated with NGOs. Auditing of the entire process was based on using a health overview document, which is a nationally developed and obligatory evaluation and planning document for municipal knowledge management [42, 43]. In addition, surveys of school children were conducted yearly.
The promotion of health and well-being guided the activity in primary healthcare. This included guidance on practicing healthy behaviors in families early. Support for health and psychosocial problems was also available [46]. Children’s overall well-being was also a target in early childhood education and care [51]. In schools, pupils’ well-being was sensitively observed to address the problems early enough. The aim of promoting the well-being of city inhabitants was a motivator for actions in sports and technical services as well. In addition to providing opportunities for PA, restructuring the city center was intended to add to the attractiveness of the environment, bring people together, and enhance recreation and well-being.
In addition to interviewees from the administrative sectors, representatives from three core collaborative partners expressed their observations about the activities that had been carried out (not included in Tables 2 and 3). The success in obesity prevention was attributed to the systematic coordination and the involvement of many crucial sectors in the work, either in collaboration or independently. Further emphasis on the importance of promoting children’s health among the public and various actors was evident by the way the work was conducted and its results were communicated in the municipality. On a practical level, the nutritionist’s input in the hospital district directly served in obesity prevention. The structures and measures that had been developed before the study period were of great importance.
Public health policy approaches for health promotion and obesity prevention in various municipal administrative sectors
Individual activities within the sectors were arranged according to the public health policy approach (Table 4). Upstream policies influence a wider scope of social and economic circumstances to affect the determinants of obesity and create environments or settings for healthy lifestyle choices. Midstream policies directly influence the behavior of populations. Downstream policies for obesity prevention represent actions in health services and clinical interventions for individuals [33].
In many sectors, various public health approaches have been integrated into the activities. Several upstream activities have been targeted to provide opportunities for PA. The city management’s support of the long-term work done by the sports and the technical sectors in the creation of environments for PA all over the city and for all inhabitants was important. At the management level, upstream activity was also directly targeted at obesity prevention in the form of the obesity program implemented in the city and by including the aims of obesity prevention and the promotion of health and well-being in the city strategy. The Director of Health Promotion played a key role in leading the activity and bringing together the relevant professionals and other parties to listen to them and disseminate information. All health-promoting work of professionals among their target populations was strongly supported by city management. The primary healthcare sector operated at an upstream level, because one of its tasks is to monitor the health and development of each child, including the measurement of their height and weight [45]. A central upstream operator, mass catering service, is responsible for offering healthy meals to all children. Early childhood education and care further boosted this work by declaring all day-care centers dessert-free.
Midstream activity is practiced in many sectors that aimed to make PA and HE elementary components of the lifestyles of children and their families; however, action was also targeted directly at obesity prevention, in addition to health and/or well-being among children. In primary health care, one core activity is to provide guidance to families and encourage them to follow healthy lifestyles. The role of the downstream approach is minor. It included a service designed to help children at risk of obesity and special services for children who had difficulties in making use of available PA opportunities.
The perceived role of the overcoming obesity program in the administrative sectors’ action
The managerial level of the city clearly identified its role in obesity prevention, which resulted in the inclusion of obesity prevention in the city strategy and implementation of the obesity program. While the interviewees in primary health care sector were aware of their important work in obesity prevention, they had only gradually become aware of their role in this program. They were convinced about the importance of early intervention, multisector work, and systematic collection of the children’s height and weight data. Both educational sectors identified the importance of their work in obesity prevention. They strongly believed that PA and HE are routes towards obesity prevention. The sports service sector was aware of its role; however, the interviewees representing technical services appeared to be unaware of their sector’s role in the obesity program. Staff members for mass catering were extremely aware of their importance in the obesity program.
Discussion
A key finding was that the importance of health promotion and obesity prevention was not only rhetorical, but also reflected in concrete actions. In addition, the activities were performed without extra resources as a part of the professionals’ duties. A large part of the work was directed at the most targeted determinants of obesity, PA and HE (e.g., [16, 33]). Children were encouraged to adopt physically active lifestyles. Easy-to-access environments and premises for PA were built, and planning was conducted in cross-sector collaboration. For HE, national nutritional guidelines and heart-healthiness were followed to provide healthy meals for children in day-care centers and schools. The prevention of childhood obesity was included in the city strategy and in the systematic monitoring of children’s growth; specific strategies helped children at risk of obesity. In many sectors, multiple activities have targeted the promotion of health and/or well-being among children and all city inhabitants.
The activities were analyzed against the OPA by Sacks et al. [33]. City management operated strongly upstream, creating opportunities and circumstances for the adoption of obesity-preventing lifestyles. Incorporating obesity prevention into the municipal strategy created a supportive environment for action across sectors. The development of the process was based on systematic evaluation [42] and principles of knowledge management [43]. Of crucial importance was the strong leadership of the person responsible for the implementation and coordination of health-promoting activity [53]. Intersectoral collaboration is enhanced if the coordinating person has a sufficiently strong position within the municipal administration [54, 55]. Since this was the case in Seinäjoki, it may have given weight to the director’s initiatives for action and, consequently, strengthened the shared understanding that all sectors’ input was needed (see [56]). The cooperation of the Director of Health Promotion with national programs for health promotion and obesity prevention [40] may have brought new ideas for activities at the local level [57, 58].
The organization of the multiprofessional health promotion activity was dominated by the upstream and midstream levels, with the aim of embedding PA and HE as elementary components of children’s lifestyles. Only two of the reported activities operated downstream. It has been noted that it is important to recognize the interaction between the levels of the socioecological model to fully base health-promoting activities on knowledge about the determinants of health [34]. This helps to create synergies by integrating different public health approaches, sectors, and settings [33, 58, 59]. The interviews revealed synergies and shared targets, particularly in the way the city management, educational sectors, and sports and technical services collaborated to create environments for PA. Additionally, the promotion of HE was a target shared by the mass catering services and educational sectors. Several midstream activities took place in settings in which children leisured and spent a large part of their everyday lives. Furthermore, the work done upstream by management strongly supported the grassroot work for health promotion that the professionals engaged in, midstream.
More information about the prerequisites for the creation of synergies was provided by inquiring about the sectors’ perception of their roles in the implementation of the municipal obesity program. Obesity prevention, as described in the city strategy, stimulated activity in most sectors. In accordance with previous research [26, 60], it was recognized that obesity is not only an individual but also a societal problem that requires collaboration to tackle it [29]. However, in some sectors, obesity programs were not identified. An example was technical services, which were key operators in providing opportunities for PA. A lack of awareness about obesity issues outside the health sector has been observed earlier [61]; it has been said that more efficient collaboration and use of resources would be possible if the awareness of the shared aims also reached sectors which do not have health promotion stated among their objectives [62,63,64]. Altogether, there seemed to be a good basis for implementing shared goals and further development of the synergies between the sectors; however, work remains to be done to spread awareness in some sectors about the importance of their input for efficient municipal health promotion.
The prevailing principle in taking actions in Seinäjoki was universalism; therefore, all opportunities for obesity-preventing lifestyles were meant to be received by every child. No such measures explicitly considered the economic, political, and social resources of children and their families [32, 33]. However, obesity in children is related to their social background [9, 65, 66] through various mechanisms, such as distress [8, 62] or readiness to make healthy nutritional choices [21, 67]. The professionals’ increased awareness of any source of social inequality could help in planning measures that would motivate various subgroups of children to make more efficient use of the opportunities offered at the upstream level to lead healthy lifestyles. The identification of groups that need special support would enable targeting more downstream activities, specifically to those who would benefit from them the most.
The OPA framework highlights the role of civil society and the private sector in obesity prevention [33]. The private sector was not explicitly mentioned in the interviews; however, its integration into obesity prevention activities could strengthen the work done upstream in many ways. This could take place, for example, by advertising and pricing products. Collaboration with several NGOs was active in the city, which adds to the potential of the facilities to reach various subgroups of the population. In addition, other social operators, such as mass media, could also be engaged in these actions.
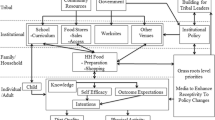
Counteractive forces to the activity, such as a conflict between the healthiness of food and its perceived taste, also existed. Despite these controversies, various new forms of action have been created with intense municipality and international collaborations. Thus, the multisectoral activity carried out enthusiastically in one municipality may be a source of inspiration and a model for activity elsewhere, even though municipalities differ according to leadership, resources, and staff training [58]. Due to this and the complex system causing obesity, no clear solution exists for the organization of the action [8] and the menu of activities involved. For example, even within one municipality, individual schools may choose different repertoires. In Seinäjoki, the activity took place in the everyday environments of children and families [24, 25] and many key people in various sectors committed to it. To condense the messages of this study, we suggest that it may have highlighted some key lines of action which could be followed by various administrative sectors in municipalities to prevent obesity among children (Fig. 1).

Key activities in childhood obesity prevention in various municipal sectors in Seinäjoki between 2009 and 2016
Strengths, limitations, and future research
The interviewees represented the administrative sectors and collaborative partners that formed the central operators in health promotion and obesity prevention during the study period. There may be other parties, not included in the study, which would be useful for understanding the entirety of the municipal health promotion activities. The municipal social services should have been included to reveal any sources of inequality or social problems that hinder children and families from making healthy choices. Social service providers were asked to attend but no response was received, which may be because of the high workload in that sector. The interviewees were informed of the interview guide for the first time by the interviewer. A written interview form given in advance could have given the interviewees more time to consider their answers. In addition, questions about interviewees’ formal education or training in obesity prevention would have enabled the assessment of information against professional backgrounds. It would be useful to analyze the extent to which the organization of collaborative networks is based on professions, fields of education, formal collaboration within the governmental system, and friendly relations. Research is also needed on the significance of various governance systems for the organization of strategies to reduce obesity [57] as well as the influence of various health and health promotion concepts on the working methods in obesity prevention in various sectors.
Conclusion
Obesity prevention was incorporated into the city strategy and systematically coordinated with various sectors strongly engaged in preventive collaboration. Both upstream and midstream public health policy approaches were followed, which meant that opportunities and environments were built and guidance was provided to help children embed PA and HE in their daily lives. Growth and development of the child population were also systematically monitored. The role of the downstream approach was minor but included an individually targeted intervention method for children at risk of obesity and PA opportunities for those with special needs. Altogether, a well-functioning network of highly motivated professionals from many sectors operated for obesity prevention and most of these professionals acknowledged their sectors’ role in this work. However, in some sectors, even if the work done was crucial, professionals did not identify their contributions to the broader work.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author, [LK], upon reasonable request. The data are in Finnish.
Abbreviations
- PA:
-
Physical activity
- HE:
-
Healthy eating
- OPA:
-
The Obesity Policy Action framework
- NGO:
-
Nongovernmental organisation
References
Bauman A, Rutter H, Baur L. Too little, too slowly: international perspectives on childhood obesity. Public Health Res Pract. 2019;29:e2911901. https://doi.org/10.17061/phrp2911901.
NCD risk factor collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight and obesity from 1975–2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390:2627–42. https://doi.org/10.1016/S0140-6736(17)32129-3.
Lundvist A, Jääskeläinen S. Lasten ja nuorten ylipaino ja lihavuus 2018 [Overweight and obesity in children 2018]. THL, Tilastoraportti. 9:2019. http://urn.fi/URN:NBN:fi-fe2019042413181 (in Finnish). Accessed 24 June 2022.
Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lancet. 2010;375:1737–48. https://doi.org/10.1016/S0140-6736(10)60171-7.
Lakshman R, Elks CE, Ong KK. Childhood obesity. Circulation. 2012;126:1770–9. https://doi.org/10.1161/CIRCULATIONAHA.111.047738.
Juonala M, Magnussen CG, Berenson GS, Venn A, Burns TL, Sabin, et al. Childhood adiposity, adult adiposity, and cardiovascular risk factors. N Engl J Med. 2011;365:1876–85. https://doi.org/10.1056/NEJMoa1010112.
van der Klaauw AA, Farooqi IS. The hunger genes: pathways to obesity. Cell. 2015;161:119–32. https://doi.org/10.1016/j.cell.2015.03.008.
Brown CL, Halvorson EE, Cohen GM, Lazorick S, Skelton JA. Addressing childhood obesity: opportunities for prevention. Pediatr Clin N Am. 2015;62:1241–61. https://doi.org/10.1016/j.pcl.2015.05.013.
Stein D, Weinberger-Litman SL, Latzer Y. Psychosocial perspectives and the issue of prevention in childhood obesity. Front Public Health. 2014;2:104. https://doi.org/10.3389/fpubh.2014.00104.
Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC. Tracking of obesity-related behaviours from childhood to adulthood: a systematic review. Maturitas. 2011;70:266–84. https://doi.org/10.1016/j.maturitas.2011.08.005.
Liberali R, Kupek E, de Assis MAA. Dietary patterns and childhood obesity risk: a systematic review. Child Obes. 2020;16:70–85. https://doi.org/10.1089/chi.2019.0059.
Wilks DC, Besson H, Lindroos AK, Ekelund U. Objectively measured physical activity and obesity prevention in children, adolescents and adults: a systematic review of prospective studies. Obes Rev. 2011;12:e119–e29. https://doi.org/10.1111/j.1467-789X.2010.00775.x.
Must A, Parisi SM. Sedentary behavior and sleep: paradoxical effects in association with childhood obesity. Int J Obes. 2009;33(Suppl 1):S82–6. https://doi.org/10.1038/ijo.2009.23.
Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. 2010;35:725–40. https://doi.org/10.1139/H10-079.
Mustila T, Raitanen J, Keskinen P, Luoto R. A pragmatic controlled trial to prevent childhood obesity within a risk group at maternity and child health-care clinics: results up to six years of age (the VACOPP study). BMC Pediatr. 2018;18:89. https://doi.org/10.1186/s12887-018-1065-3.
Newman L, Ludford I, Williams C, Herriot M. Applying health in all policies to obesity in South Australia. Health Promot Int. 2016;31:44–58. https://doi.org/10.1093/heapro/dau064.
Waters E, de Silva-Sanigorski A, Hall BJ, Brown T, Campbell KJ, Gao Y, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2011;12:CD001871. https://doi.org/10.1002/14651858.CD001871.pub3.
Korkalo L, Nissinen K, Skaffari E, Vepsäläinen H, Lehto R, Kaukonen R, et al. The contribution of preschool meals to the diet of Finnish preschoolers. Nutrients. 2019;11:1531. https://doi.org/10.3390/nu11071531.
Story M, Kaphingst KM, Robinson-O’Brien R, Glanz K. Creating healthy food and eating environments: policy and environmental approaches. Annu Rev Public Health. 2008;2008(29):253–72. https://doi.org/10.1146/annurev.publhealth.29.020907.090926.
Verjans-Janssen SRB, van de Kolk I, Van Kann DHH, Kremers SPJ, Gerards SMPL. Effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI and energy balance-related behaviors—a systematic review. PLoS One. 2018;13:e0204560. https://doi.org/10.1371/journal.pone.0204560.
Vepsäläinen H, Korkalo L, Mikkilä V, Lehto R, Ray C, Nissinen K, et al. Dietary patterns and their associations with home food availability among Finnish pre-school children: a cross-sectional study. Public Health Nutr. 2018;21:1232–42. https://doi.org/10.1017/S1368980017003871.
Xu H, Wen LM, Rissel C. Associations of parental influences with physical activity and screen time among young children: a systematic review. J Obes. 2015;2015:546925. https://doi.org/10.1155/2015/546925.
Draper CE, Grobler L, Micklesfield LK, Norris SA. Impact of social norms and social support on diet, physical activity and sedentary behaviour of adolescents: a sco** review. Child Care Health Dev. 2015;41:654–67. https://doi.org/10.1111/cch.12241.
Morton KL, Atkin AJ, Corder K, Suhrcke M, van Sluijs EM. The school environment and adolescent physical activity and sedentary behaviour: a mixed-studies systematic review. Obes Rev. 2016;17:142–58. https://doi.org/10.1111/obr.12352.
Wilson DK, Sweeney AM, Kitzman-Ulrich H, Gause H, St George SM. Promoting social nurturance and positive social environments to reduce obesity in high-risk youth. Clin Child Family Psychol Rev. 2017;20:64–77. https://doi.org/10.1007/s10567-017-0230-9.
Commission on Ending Childhood Obesity. Report of the Commission on Ending Childhood Obesity. Geneva: World Health Organization; 2016. http://apps.who.int/iris/bitstream/10665/204176/1/9789241510066_eng.pdf?ua=1. Accessed 29 November 2016
Sallis JF, Glanz K. Physical activity and food environments: solutions to the obesity epidemic. Milbank Q. 2009;87:123–54. https://doi.org/10.1111/j.1468-0009.2009.00550.x.
Townshend T, Lake A. Obesogenic environments: current evidence of the built and food environments. Perspect Public Health. 2017;137:38–44. https://doi.org/10.1177/1757913916679860.
Gortmaker SL, Swinburn BA, Levy D, Carter R, Mabry PL, Finegood DT, et al. Changing the future of obesity: science, policy, and action. Lancet. 2011;378:838–47. https://doi.org/10.1016/S0140-6736(11)60815-5.
Nishtar S, Gluckman P, Armstrong T. Ending childhood obesity: a time for action. Lancet. 2016;387:825–7. https://doi.org/10.1016/S0140-6736(16)00140-9.
World Health Organization. Population-based approaches to childhood obesity prevention. Geneva: world health Organization; 2012. http://www.who.int/dietphysicalactivity/childhood/WHO_new_childhoodobesity_PREVENTION_27nov_HR_PRINT_OK.pdf. Accessed 22 April 2021.
CSDH. Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the commission on social determinants of health. Geneva: world health Organization; 2008. http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf. Accessed 8 February 2021.
Sacks G, Swinburn BA, Lawrence M. Obesity policy action framework and analysis grids for a comprehensive policy approach to reducing obesity. Obes Rev. 2009;10:76–86. https://doi.org/10.1111/j.1467-789X.2008.00524.x.
Sallis JF, Owen N, Fisher EN. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education. Theory, research, and practice. San Francisco: John Wiley & Sons, Inc.; 2008. p. 251–306.
Saaristo T, Peltonen M, Keinänen-Kiukaanniemi S, Vanhala M, Saltevo J, Niskanen L. National type 2 diabetes prevention programme in Finland: FIN-D2D. Int J Circumpolar Health. 2007;66:101–12. https://doi.org/10.3402/ijch.v66i2.18239.
Etelä-Pohjanmaan Sairaanhoitopiiri, Perusterveydenhuollon ja terveyden edistämisen yksikkö. Lapsen ja nuoren painopolku [A Child’s and Adolescent’s Weight Path]. 2021. http://www.epshp.fi (in Finnish). Accessed 24 June 2022.
Ylihärsilä O. Hyvinvointia ravinnosta ja liikunnasta. Lihavuus laskuun ohjelman toteutus Seinäjoella. [Wellbeing from physical activity and healthy nutrition. Implementation of the overcoming obesity Programme in Seinäjoki]. HYTE-oppimisverkoston kansallinen foorumi [National Forum of the HYTE Learning Network]. 2014. https://slideplayer.fi/slide/11169231/ (in Finnish). Accessed 23 Apr 2021.
THL. The national obesity programme 2012–2018. Helsinki: Terveyden ja hyvinvoinnin laitos. 2019. https://thl.fi/en/web/thlfi-en/research-and-expertwork/projects-and-programmes/the-national-obesity-programme-2012-2015 (in Finnish). Accessed 23 Apr 2021.
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107–15. https://doi.org/10.1111/j.1365-2648.2007.04569.x.
THL. Lihavuus laskuun. Hyvinvointia ravinnosta ja liikunnasta. Toiminta ja toimeenpanosuunnitelma 2016–2018. [Wellbeing from physical activity and healthy nutrition]. Helsinki: Terveyden ja hyvinvoinnin laitos, Työpaperi 18. 2016. http://www.julkari.fi/bitstream/handle/10024/130539/URN_ISBN_978-952-302-665-0.pdf?sequence=1 (in Finnish). Accessed 22 Apr 2021.
Ministry of Social Affairs and Health. Health 2015 public health programme. Helsinki: Brochures; 2001. p. 8eng. https://julkaisut.valtioneuvosto.fi/handle/10024/70167. Accessed 22 April 2021.
Health Care Act, 1326/2010, § 12. https://finlex.fi/en/laki/kaannokset/2010/en20101326. Accessed 8 Feb 2021.
Ståhl T, Wiss K, Hakamäki P, Saaristo V. Hyvinvoinnin ja terveyden edistämisen toteutuminen kunnassa—rakenteet, vastuut, seuranta ja voimavarat [Promotion of health and wellbeing in municipalities – structures, responsibilities, monitoring and resources.]. Tutkimuksesta tiiviisti 31/2015. Terveyden ja hyvinvoinnin laitos, Helsinki: Terveyden ja hyvinvoinnin laitos. 2015. http://www.julkari.fi/bitstream/handle/10024/126897/URN_ISBN_978-952-302-527-1.pdf?sequence=1 (in Finnish). Accessed 22 Apr 2021.
Finnish Heart Association. Neuvokas perhe [Smart family method]. 2020. https://neuvokasperhe.fi/en/. (in Finnish). Accessed 22 Apr 2021.
Ministry of Social Affairs and Health. Primary Health Care. 2021. https://stm.fi/en/primary-health-care. Accessed 22 Apr 2021.
Seinäjoki. Pilari [The Pillar Center]. 2021. https://www.seinajoki.fi/sosiaali-ja-terveys/perhekeskuspalvelut/pilari-13-25-vuotiaiden-palvelut/ (in Finnish). Accessed 10 June 2021.
LiikU. Liikkuva varhaiskasvatus - Ilo kasvaa liikkuen. [Early Childhood Education in the Move. Joy Grows through Motion]. 2018. https://www.liiku.fi/varhaiskasvattajille/liikkuva-varhaiskasvatus/ (in Finnish). Accessed 23 April 2021.
Ministry of Education and Culture. Varhaisvuosien fyysisen aktiivisuuden suositukset 2016. Iloa, leikkiä ja yhdessä tekemistä, 2016 [Recommendations for physical acivity in the early years. Joy, play, and doing things together]. Helsinki: Publications of the Ministry of Education and Culture 2106:21. 2016. http://urn.fi/URN:ISBN:978-952-263-410-8 (in Finnish). Accessed 22 Apr 2021.
National Nutrition Council. Eating and learning together—recommendations for school meals. Helsinki: Juvenes Print. 2017. http://www.julkari.fi/bitstream/handle/10024/134867/URN_ISBN_978-952-302-844-9.pdf?sequence=1&isAllowed=y. Accessed 22 Apr 2021.
Etelä-Pohjanmaan Sairaanhoitopiiri, Perusterveydenhuollon ja terveyden edistämisen yksikkö. Kaappaa kasvis! [Grab the Veggie!]. 2020. http://www.epshp.fi/kaappaakasvis (in Finnish). Accessed 8 Feb 2021.
Ministry of Education and Culture. Finnish education system. 2018. https://minedu.fi/en/education-system#ecec. Accessed 22 Apr 2021.
Blom A, Tammelin T, Laine K, Tolonen H. (2018) bright spots, physical activity investments that work: the Finnish schools on the move programme. Br J Sports Med. 2018;52:820–2. https://doi.org/10.1136/bjsports-2017-097711.
Rantala R, Bortz M, Armada F. Intersectoral action: local governments promoting health. Health Promot Int. 2014;29(Suppl 1):i92–i102. https://doi.org/10.1093/heapro/dau047.
Hagen S, Helgesen M, Torp S, Fosse E. Health in all policies: a cross-sectional study of the public health coordinators’ role in Norwegian municipalities. Scand J Public Health. 2015;43:597–605. https://doi.org/10.1177/1403494815585614.
Hofstad H. The ambition of health in all policies in Norway: the role of political leadership and bureaucratic change. Health Policy. 2016;120:567–75. https://doi.org/10.1016/j.healthpol.2016.03.001.
Campbell MK. Biological, environmental, and social influences on childhood obesity. Pediatr Res. 2016;79:205–11. https://doi.org/10.1038/pr.2015.208.
Freudenberg N, Libman K, O’Keefe E. A tale of two obesCities: the role of municipal governance in reducing childhood obesity in new York City and London. J Urban Health. 2010;87:755–70. https://doi.org/10.1007/s11524-010-9493-x.
Weiss D, Lillefjell M, Magnus E. Facilitators for the development and implementation of health promoting policy and programs—a sco** review at the local community level. BMC Public Health. 2016;16:140. https://doi.org/10.1186/s12889-016-2811-9.
Hendriks AM, Kremers SP, Gubbels JS, Raat H, de Vries NK, Jansen MW. Towards health in all policies for childhood obesity prevention. J Obes. 2013;2013:632540. https://doi.org/10.1155/2013/632540.
Schwartz MB, Puhl R. Childhood obesity: a societal problem to solve. Obes Rev. 2003;4:57–71. https://doi.org/10.1046/j.1467-789x.2003.00093.x.
Aarts MJ, Jeurissen MP, van Oers HA, Schuit AJ, van de Goor IA. Multi-sector policy action to create activity-friendly environments for children: a multiple-case study. Health Policy. 2011;101:11–9. https://doi.org/10.1016/j.healthpol.2010.09.011.
Krech R. Healthy public policies: looking ahead. Health Promot Int. 2011;26(Suppl 2):ii268–i72. https://doi.org/10.1093/heapro/dar066.
Melkas T. Health in all policies as a priority in Finnish health policy: a case study on national health policy development. Scand J Public Health. 2013;41(Suppl):3–28. https://doi.org/10.1177/1403494812472296.
Molnar A, Renahy E, O’Campo P, Muntaner C, Freiler A, Shankardass K. Using win-win strategies to implement health in all policies: a cross-case analysis. PLoS One. 2016;11:e0147003. https://doi.org/10.1371/journal.pone.0147003.
Kautiainen S, Koivisto AM, Koivusilta L, Lintonen T, Virtanen SM, Rimpelä A. Sociodemographic factors and a secular trend of adolescent overweight in Finland. Int J Pediatr Obes. 2009;4:360–70. https://doi.org/10.3109/17477160902811173.
Parikka S, Mäki P, Levälahti E, Lehtinen-Jacks S, Martelin T, Laatikainen T. Associations between parental BMI, socioeconomic factors, family structure and overweight in Finnish children: a path model approach. BMC Public Health. 2015;15:271. https://doi.org/10.1186/s12889-015-1548-1.
MacFarlane A, Crawford D, Ball K, Savige G, Worsley A. Adolescent home food environments and socioeconomic position. Asia Pac J Clin Nutr. 2007;16:748–56.
Acknowledgements
We warmly thank all the interviewed professionals, the City of Seinäjoki for the permission for this study and MD, PhD Taina Mustila for her valuable comments on the manuscript.
Funding
This work was supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital [project number 5500/311].
Author information
Authors and Affiliations
Contributions
LK and SA designed the research, and LK, SA and TS analysed the data. MK carried out the interviews. LK drafted the first version of the manuscript, which was critically reviewed by all other authors, who then approved the final version for submission. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The city of Seinäjoki granted formal approval for the research and for the access and use of the interview material collected in the study (a decision signed by the Head of Office, 18 October 2016, paragraph 41/2016). Every interviewee signed an informed consent form before the interview and was informed that participation in the study was voluntary, that withdrawing at any point was possible and that the individuals could not be identified at any stage of the research. No ethics review was needed because the study was not medical research involving human subjects (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Koivusilta, L., Alanne, S., Kamila, M. et al. A qualitative study on multisector activities to prevent childhood obesity in the municipality of Seinäjoki, Finland. BMC Public Health 22, 1298 (2022). https://doi.org/10.1186/s12889-022-13658-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13658-z