
Abstract
Background
Cross-sectional and longitudinal studies have found that problematic mobile phone use, bedtime procrastination, sleep quality, and depressive symptoms are strongly associated. However, studies are inconsistent regarding whether problematic mobile phone use predicts depressive symptoms or vice versa, and sleep factors have been infrequently focused on in this regard. In addition, few studies have examined the longitudinal associations and directions of effects between these factors. Therefore, this study aims to explore the longitudinal relationship among problematic mobile phone use, bedtime procrastination, sleep quality, and depressive symptoms in college students.
Methods
Overall, 1181 college students completed questionnaires on problematic mobile phone use, bedtime procrastination, sleep quality, and depressive symptoms at two time points 12 months apart. A cross-lagged model was used to examine the longitudinal relationship between these factors.
Results
Cross-lagged analyses showed significant bidirectional relationships of problematic mobile phone use with bedtime procrastination and depressive symptoms. Additionally, there were also significant bidirectional relationships of sleep quality with bedtime procrastination and depressive symptoms. Problematic mobile phone use predicted subsequent sleep quality one-way, and bedtime procrastination predicted subsequent depressive symptoms one-way.
Conclusions
This study further expands our understanding of the longitudinal and bidirectional relationships among problematic mobile phone use, bedtime procrastination, sleep quality and depressive symptoms and helps school mental health educators design targeted interventions to reduce problematic mobile phone use, sleep problems, and depressive symptoms among college students.
Similar content being viewed by others

Introduction
With the rapid development of Internet technology, electronic products such as mobile phones have become one of the main tools for individuals to access and supply information [1]; conduct interpersonal communication; obtain entertainment, diversion, and relaxation; receive monetary compensation (such as finding bargains on product and services to save money, getting profitable financial information, or working and doing tasks to make money) [2]; and pursue other activities (such as education and health management), by virtue of their devices’ convenience, accessibility, and powerful functions [3, 4]. However, in the process of using these electronic products and the functions they enable, human beings often experience a variety of problematic behaviors, including overuse and dependence [5], which have gradually become the focus of academic attention. Among groups that typically have access to their own phones, adolescents and young adults, especially college students, are more likely to experience problematic mobile phone use (PMPU) because they have more free time, lower levels of self-control, and increased identity and lifestyle needs (such as online learning, social interaction, games, and shop**) [6,7,8]. A meta-analysis pointed out that the prevalence of PMPU among Chinese college students was as high as 23% [9]. In a previous study, PMPU was defined as uncontrolled or excessive use of mobile phones by individuals that causes problems in daily life [10]. In some studies, it was also referred to as mobile phone dependence [11], mobile phone addiction [12], and smartphone addiction [13]. Similar to the symptoms of substance use disorder, uncontrolled and excessive use was the important symptoms and characteristics of PMPU [14]. In this concept, uncontrolled use was considered a core feature of PMPU, meaning, although aware of the adverse effects, individuals still used and had difficulty controlling the use of mobile phones [10]. Further, excessive use means that an individual’s mobile phone use exceeds a certain time and range. Obviously, this requires a demarcation point to determine whether an individual has excessive mobile phone use. Based on the existing research, it is not feasible to determine the cut-off point by using quantitative methods such as time and frequency, because the motivations and natures or modes of mobile phone use of different individuals are very heterogeneous [15]. For example, when mobile phones were used to contact families and friends, provide social support, or when learning or working with an aim to increase productivity or self-improvement (such as participating in online work conferences, browsing online learning resources, information retrieval, and schedules) [16], the use time of mobile phone can be long and may not have negative consequences; such situations should not be categorized as excessive mobile phone use [17]. Therefore, on the basis of considering the motivation, nature or mode of mobile phone use, current studies tend to use evaluation from the perspective of others (for example, my classmates say that I use mobile phones for too long and too often), rather than quantitative methods to judge excessive use. Specifically, when evaluating excessive use, it need to declare to participants that the mobile phone usage in the evaluation refers to mobile phone use patterns or content are uncontrolled online games, social media, or entertainment (e.g., watching movies and listening music)—and the reason or motivation for use is evasion of reality, failure to regulate stress and negative emotions, and boredom, fear of missing out [14] or specific personality traits such as shyness [10]. In addition, PMPU also showed two characteristics: tolerance (the frequency and duration of mobile phone use by individuals to achieve satisfaction have increased significantly) and withdrawal (individuals experience psychological withdrawal symptoms such as panic, restlessness, and irritability when separated from their mobile phone) [18]. Therefore, in this study, we define PMPU as an individual’s uncontrolled or excessive use of mobile phones and adverse effects when performing activities with the motivation and purpose of relieving negative emotions, relaxing oneself, and satisfying online social and entertainment needs, rather than activities with the motivation and purpose of self-improvement, increase productivity or search for social support, such as work, study, and communication with families and friends.
The concept of PMPU is somewhat controversial, because the main function of mobile phones was the operation of Internet-based applications [19], which indicates that PMPU has many similarities with Internet-based addictions, such as gaming disorders, and may have mutual influences. For example, individuals with Internet addiction are more likely to experience PMPU, and vice versa. Previous research has shown that there was a positive correlation between Internet addiction and PMPU [20]. However, studies have also shown differences between the two in risk factors such as gender and personality characteristics [21]. For example, men experience more Internet addiction, while women demonstrate more PMPU [22]. However, it should be noted that mobile phones not only provide functions such as the Internet and games, but also have various other services and functions such as communications, cameras, multimedia playback, painting, and e-book reading. These services may not be related to the Internet. In addition, individual Internet use relies not only on mobile phones but also on desktop laptops, computers, or digital tablets. Therefore, some symptoms of PMPU may be different from those of Internet addiction. In addition, a study found that, compared with using their phones for playing games, individuals with PMPU were more likely to use social networks [23], which indicates that there may also be differences between PMPU and gaming disorders. Therefore, current research tends to treat PMPU as an independent concept, and has developed some specific assessment tools [15, 24,25,26], which are widely accepted and recognized by scholars. However, it should be noted that none of the existing scales can fully consider the characteristics of uncontrolled or excessive, tolerance and withdrawal to evaluate PMPU [15]. Thus, this study used the Mobile Phone Addiction Tendency Scale (MPATS), which is widely used in mainland China, to focus on the evaluation of uncontrolled use, excessive use evaluated by classmates or friends, tolerance, withdrawal symptoms, and negative consequences [39]. This indirectly indicated that poor sleep quality may cause individuals to develop PMPU. Studies have shown that in individuals with PMPU, constant exposure to blue light can inhibit the secretion of melatonin, and cause sleep and circadian rhythm disorders [40, 41], which might be an important factor in the generation of psychopathological symptoms such as depression [42]. Previous studies have explored the mediating role of sleep quality between PMPU and depressive symptoms using cross-sectional study designs [Measurements PMPU was measured using the MPATS, developed by ** medication, and daytime dysfunction. A Likert 4-level scoring method (0–3 points) was used for each dimension, for a total score of 0–21 points; the higher the score, the lower the sleep quality of the subjects. We used the Chinese version of the PSQI in this study [67]. The Cronbach’s alpha of the scale was 0.70 and 0.73 at T1 and T2, respectively. The PHQ-9 was used to evaluate the frequency of depressive symptoms over the past two weeks [68]. This scale had been translated into Chinese, and showed good psychometric properties in the general population [69]. It is composed of nine items, with 0, 1, 2, and 3 points corresponding to “no,” “several days,” “more than half of the days,” and “almost every day,” respectively, for a total score of 0–27 points; the higher the score, the more serious the depressive symptoms. The Cronbach’s alpha of the scale was 0.86 and 0.89 at T1 and T2, respectively. The descriptive statistics and Pearson’s correlation analysis were conducted using SPSS version 25.0 (IBM Corporation, Armonk NY, USA) for Windows. Data are presented as n (%) for categorical variables and mean ± SD for numerical variables. We used AMOS 23.0 software to perform cross-lagged panel analysis. First, we evaluated the longitudinal measurement invariance of the four scales used in this study, including configural invariance, metric invariance, and scalar invariance [70]. Second, adjusting gender and age, we constructed a cross-lagged model to test the longitudinal bidirectional relationships among PMPU, bedtime procrastination, sleep quality and depressive symptoms in college students. Model fit was evaluated using comparative fit index (CFI), Tucker–Lewis index (TLI), root–mean–square error of approximation (RMSEA) and standard root–mean–square (SRMR). According to previous studies [71], CFI and TLI greater than 0.90 and RMSEA and SRMR less than 0.08 indicate that the model fit is acceptable. Considering that chi-squared is sensitive to sample size, we did not use chi-squared as an indicator of model fit [72]. Meanwhile, we calculated 95% confidence intervals (CI) using a bias-corrected bootstrap sample that was repeated 5000 times. The 95% CI did not include zero, indicating that the effect was statistically significant (p-value < 0.05). In addition, we used the change values of CFI (ΔCFI) and RMSEA (ΔRMSEA) to evaluate the measurement invariance. When ΔCFI≤0.01 and ΔRMSEA≤0.015, the measurement invariance model was acceptable [73].MPATS
The patient Health Questionnaire-9 (PHQ-9)
Data analysis
Results
Measurement invariance test
In order to test the longitudinal measurement invariance of the scales, we first established configural invariance models. The results showed that the configural invariance models of the four scales all fitted well. Subsequently, we set the factor loadings to be equal over time and established metric invariance models. All model fits were good. The fit results of the metric invariance models showed that ΔCFI and ΔRMSEA were both less than 0.01, indicating invariance of factor loadings on each scale over time. On the basis of the metric invariance model, we further restricted the equality of thresholds, to test scalar invariance; ΔCFI and ΔRMSEA were still within the acceptable range. These results indicate that the four scales have measurement invariance at two time points. More results about the model-fitting index are shown in Multimedia Appendix 1.
Descriptive and correlational analyses
Table 1 shows the means, standard deviations, and correlations of the variables. Correlation analysis showed statistically significant correlations among the four variables of PMPU, bedtime procrastination, sleep quality, and depressive symptoms at two time points.
Cross-lagged model
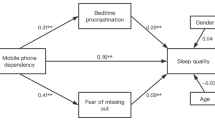
The cross-lagged model showed good fit to the data (χ2(df) = 6.682(3), p > 0.05; CFI = 0.999, TLI = 0.986, RMSEA = 0.032, SRMR = 0.010). Figure 1 and Table 2 display the results for the cross-lagged model. The results suggest that PMPU at T1 positively predicted bedtime procrastination, depressive symptoms at T2 and vice versa, while sleep quality was only significantly predicted one-way. Bedtime procrastination at T1 positively predicted sleep quality at T2, and vice versa and only significantly positively predicted depressive symptoms one-way. Moreover, sleep quality at T1 positively predicted depressive symptoms at T2 and vice versa.

Cross-lagged relationships among PMPU, bedtime procrastination, sleep quality, and depressive symptoms. Notes: *p < 0.05, **p < 0.01. Only statistically significant paths are displayed
Discussion
In this study, we adopted a two-wave longitudinal design and constructed a cross-lagged model to analyze the bidirectional associations among PMPU, bedtime procrastination, sleep quality, and depressive symptoms. These findings help to understand the longitudinal associations and direction of effects among these factors. The results suggest some longitudinal associations in both directions: (1) PMPU with bedtime procrastination and depressive symptoms; (2) sleep quality with bedtime procrastination and depressive symptoms. As far as we know, this is the first study in which bedtime procrastination was bidirectionally associated with problematic phone use and sleep quality. There were also some one-way associations: (1) PMPU predicted sleep quality, and (2) bedtime procrastination predicted depressive symptoms.
This study showed that depressive symptoms were bidirectionally associated with PMPU and sleep quality, consistent with previous studies [37, 46, 74]. However, a recent 6-month longitudinal study in China found that depressive symptoms at baseline predicted follow-up PMPU, as opposed to the converse [13]. A possible reason was that the length of follow-up was different, which may lead to different directions of effect between PMPU and depressive symptoms. Two previous longitudinal studies, of more than 1 year each, in South Korea found a bidirectional relationship between PMPU and depressive symptoms [37, 75]. However, a 3-month short-term longitudinal study in the United States found only a one-way association, in which PMPU at baseline predicted follow-up depressive symptoms [76]. This may mean that it will take longer to observe the bidirectional relationship between the two. However, there have also been longer than 1 year longitudinal studies that found only a one-way relationship [ This study further expands our understanding of the longitudinal and bidirectional relationship among PMPU, bedtime procrastination, sleep quality, and depressive symptoms. In addition, it will assist school mental health educators in designing targeted interventions to reduce PMPU, sleep problems, and depressive symptoms among college students.Conclusion
Availability of data and materials
Data can be obtained by contacting the corresponding author with appropriate reasons.
Abbreviations
- PMPU:
-
Problematic mobile phone use
- CFI:
-
Comparative fit index
- TLI:
-
Tucker–Lewis index
- RMSEA:
-
Root–mean–square error of approximation
- SRMR:
-
Standardized root–mean–square residual
References
Mihailidis P. A tethered generation: exploring the role of mobile phones in the daily life of young people. Mobile Media Communication. 2013;2(1):58–72. https://doi.org/10.1177/2050157913505558.
Song I, Larose R, Eastin MS, Lin CA. Internet gratifications and internet addiction: on the uses and abuses of new media. CyberPsychol Behav. 2004;7(4):384–94. https://doi.org/10.1089/cpb.2004.7.384.
AlTameemy F. Mobile phones for teaching and learning: implementation and students’ and teachers’ attitudes. J Educ Technol Syst. 2017;45(3):436–51. https://doi.org/10.1177/0047239516659754.
Pai RR, Alathur S. Assessing awareness and use of mobile phone technology for health and wellness: insights from India. Health Policy Technol. 2019;8(3):221–7. https://doi.org/10.1016/j.hlpt.2019.05.011.
Elhai JD, Dvorak RD, Levine JC, Hall BJ. Problematic smartphone use: a conceptual overview and systematic review of relations with anxiety and depression psychopathology. J Affect Disord. 2017;207:251–9. https://doi.org/10.1016/j.jad.2016.08.030.
Takao M, Takahashi S, Kitamura M. Addictive personality and problematic mobile phone use. CyberPsychol Behav. 2009;12(5):501–7. https://doi.org/10.1089/cpb.2009.0022.
Busch PA, McCarthy S. Antecedents and consequences of problematic smartphone use: a systematic literature review of an emerging research area. Comput Hum Behav. 2021;114:106414. https://doi.org/10.1016/j.chb.2020.106414.
Bianchi A, Phillips JG. Psychological predictors of problem mobile phone use. CyberPsychol Behav. 2005;8(1):39–51. https://doi.org/10.1089/cpb.2005.8.39.
Tao J, Luo C, Huang J, Liang L. Meta analysis of mobile phone dependence of Chinese college students. Chin J School Health. 2018;39(6):1391–4.
Joel B. Problematic Use of the Mobile phone: a literature review and a pathways model. Curr Psychiatr Rev. 2012;8(4):299–307. https://doi.org/10.2174/157340012803520522.
Zhang G, Yang X, Tu X, Ding N, Lau JTF. Prospective relationships between mobile phone dependence and mental health status among Chinese undergraduate students with college adjustment as a mediator. J Affect Disord. 2020;260:498–505. https://doi.org/10.1016/j.jad.2019.09.047.
Zhang CH, Li G, Fan ZY, Tang XJ, Zhang F. Mobile phone addiction mediates the relationship between alexithymia and learning burnout in Chinese medical students: a structural equation model analysis. Psychol Res Behav Manag. 2021;14:455–65. https://doi.org/10.2147/PRBM.S304635.
Zhou H, Dang L, Lam LW, Zhang MX, Wu AMS. A cross-lagged panel model for testing the bidirectional relationship between depression and smartphone addiction and the influences of maladaptive metacognition on them in Chinese adolescents. Addict Behav. 2021;120:106978. https://doi.org/10.1016/j.addbeh.2021.106978.
Elhai JD, Yang H, Montag C. Cognitive- and emotion-related dysfunctional co** processes: Transdiagnostic mechanisms explaining depression and Anxiety’s relations with problematic smartphone Use. Curr Addiction Rep. 2019;6(4):410–7. https://doi.org/10.1007/s40429-019-00260-4.
Harris B, Regan T, Schueler J, Fields SA. Problematic Mobile phone and smartphone Use scales: a systematic review. Front Psychol. 2020;11:672. https://doi.org/10.3389/fpsyg.2020.00672.
Elhai JD, Contractor AA. Examining latent classes of smartphone users: relations with psychopathology and problematic smartphone use. Comput Hum Behav. 2018;82:159–66. https://doi.org/10.1016/j.chb.2018.01.010.
Elhai JD, Levine JC, Alghraibeh AM, Alafnan AA, Aldraiweesh AA, Hall BJ. Fear of missing out: testing relationships with negative affectivity, online social engagement, and problematic smartphone use. Comput Hum Behav. 2018;89:289–98. https://doi.org/10.1016/j.chb.2018.08.020.
Billieux J, Maurage P, Lopez-Fernandez O, Kuss DJ, Griffiths MD. Can disordered Mobile phone Use be considered a behavioral addiction? An update on current evidence and a comprehensive model for future research. Curr Addiction Rep. 2015;2(2):156–62. https://doi.org/10.1007/s40429-015-0054-y.
Mok JY, Choi SW, Kim DJ, Choi JS, Lee J, Ahn H, et al. Latent class analysis on internet and smartphone addiction in college students. Neuropsychiatr Dis Treat. 2014;10:817–28. https://doi.org/10.2147/NDT.S59293.
Ben-Yehuda L, Greenberg L, Weinstein A. Internet addiction by using the smartphone-relationships between internet addiction, frequency of smartphone use and the state of mind of male and female students. J Reward Defic Syndr Addict Sci. 2016;2(1):22–7. https://doi.org/10.17756/jrdsas.2016-024.
** Jeong Y, Suh B, Gweon G. Is smartphone addiction different from internet addiction? Comparison of addiction-risk factors among adolescents. Behav Inform Technol. 2020;39(5):578–93. https://doi.org/10.1080/0144929X.2019.1604805.
Lee SY, Lee D, Nam CR, Kim DY, Park S, Kwon JG, et al. Distinct patterns of internet and smartphone-related problems among adolescents by gender: latent class analysis. J Behav Addict. 2018;7(2):454–65. https://doi.org/10.1556/2006.7.2018.28.
Jeong S-H, Kim H, Yum J-Y, Hwang Y. What type of content are smartphone users addicted to?: SNS vs. games. Comput Hum Behav. 2016;54:10–7. https://doi.org/10.1016/j.chb.2015.07.035.
Lin Y-H, Chang L-R, Lee Y-H, Tseng H-W, Kuo TBJ, Chen S-H. Development and validation of the smartphone addiction inventory (SPAI). PLoS One. 2014;9(6):e98312. https://doi.org/10.1371/journal.pone.0098312.
Kwon M, Kim D-J, Cho H, Yang S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS One. 2013;8(12):e83558. https://doi.org/10.1371/journal.pone.0083558.
Merlo LJ, Stone AM, Bibbey A. Measuring problematic Mobile phone Use: development and preliminary psychometric properties of the PUMP scale. J Addict. 2013;2013:912807–7. https://doi.org/10.1155/2013/912807.
**ong J, Zhou Z, Chen W, You Z, Zhai Z. Development of the mobile phone addiction tendency scale for college students. Chin Ment Health J. 2012;26:222–5.
Mustafaoglu R, Yasaci Z, Zirek E, Griffiths MD, Ozdincler AR. The relationship between smartphone addiction and musculoskeletal pain prevalence among young population: a cross-sectional study. Korean J Pain. 2021;34(1):72–81. https://doi.org/10.3344/kjp.2021.34.1.72.
Alghnam S, Towhari J, Alkelya M, Alsaif A, Alrowaily M, Alrabeeah F, et al. The association between Mobile phone use and severe traffic injuries: a case-control study from Saudi Arabia. Int J Environ Res Public Health. 2019;16(15):2706. https://doi.org/10.3390/ijerph16152706.
Yang J, Fu X, Liao X, Li Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: a systematic review and meta-analysis. Psychiatry Res. 2020;284:112686. https://doi.org/10.1016/j.psychres.2019.112686.
Li Y, Li G, Liu L, Wu H. Correlations between mobile phone addiction and anxiety, depression, impulsivity, and poor sleep quality among college students: a systematic review and meta-analysis. J Behav Addict. 2020;9(3):551–71. https://doi.org/10.1556/2006.2020.00057.
Li C, Liu D, Dong Y. Self-esteem and problematic smartphone Use among adolescents: a moderated mediation model of depression and interpersonal trust. Front Psychol. 2019;10:9. https://doi.org/10.3389/fpsyg.2019.02872.
Jang S-H, Ha Y. The effects of self-determination, depression, self-esteem, and impulsivity on smartphone overdependence of college students. J Digital Convergence. 2019;17(1):269–80.
Yang X, Zhou Z, Liu Q, Fan C. Mobile phone addiction and adolescents’ anxiety and depression: the moderating role of mindfulness. J Child Fam Stud. 2019;28(3):822–30. https://doi.org/10.1007/s10826-018-01323-2.
Ghasempour A, Mahmoodi-Aghdam M. The role of depression and attachment styles in predicting students’ addiction to cell phones. Addict Health. 2015;7(3–4):192–7.
Chen L, Yan Z, Tang W, Yang F, **e X, He J. Mobile phone addiction levels and negative emotions among Chinese young adults: the mediating role of interpersonal problems. Comput Hum Behav. 2016;55:856–66. https://doi.org/10.1016/j.chb.2015.10.030.
Jun S. The reciprocal longitudinal relationships between mobile phone addiction and depressive symptoms among Korean adolescents. Comput Hum Behav. 2016;58:179–86. https://doi.org/10.1016/j.chb.2015.12.061.
Kang Y, Liu S, Yang L, Xu B, Lin L, **e L, et al. Testing the bidirectional associations of Mobile phone addiction behaviors with mental distress, sleep disturbances, and sleep patterns: a one-year prospective study among Chinese college students. Front Psychiatry. 2020;11:634. https://doi.org/10.3389/fpsyt.2020.00634.
Kater MJ, Schlarb AA. Smartphone usage in adolescents – motives and link to sleep disturbances, stress and sleep reactivity. Somnologie. 2020;24(4):245–52. https://doi.org/10.1007/s11818-020-00272-7.
Touitou Y, Touitou D, Reinberg A. Disruption of adolescents’ circadian clock: The vicious circle of media use, exposure to light at night, sleep loss and risk behaviors. J Physiol Paris. 2016;110(4, Part B):467–79.
Thomee S. Mobile Phone Use and Mental Health. A review of the research that takes a psychological perspective on exposure. Int J Environ Res Public Health. 2018;15(12):2692. https://doi.org/10.3390/ijerph15122692.
Wulff K, Gatti S, Wettstein JG, Foster RG. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat Rev Neurosci. 2010;11(8):589–99. https://doi.org/10.1038/nrn2868.
Zou L, Wu X, Tao S, Xu H, **e Y, Yang Y, et al. Mediating effect of sleep quality on the relationship between problematic Mobile phone Use and depressive symptoms in college students. Front Psychiatry. 2019;10:822. https://doi.org/10.3389/fpsyt.2019.00822.
Liu J, Liu Colin X, Wu T, Liu B-P, Jia C-X, Liu X. Prolonged mobile phone use is associated with depressive symptoms in Chinese adolescents. J Affect Disord. 2019;259:128–34. https://doi.org/10.1016/j.jad.2019.08.017.
Demirci K, Akgonul M, Akpinar A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J Behav Addict. 2015;4(2):85–92. https://doi.org/10.1556/2006.4.2015.010.
Peltz JS, Rogge RD, Bodenlos JS, Kingery JN, Pigeon WR. Changes in psychological inflexibility as a potential mediator of longitudinal links between college students’ sleep problems and depressive symptoms. J Contextual Behav Sci. 2020;15:110–22. https://doi.org/10.1016/j.jcbs.2019.12.003.
Wang W, Du X, Guo Y, Li W, Teopiz KM, Shi J, et al. The Associations Between Sleep Situations and Mental Health Among Chinese Adolescents: A Longitudinal Study. Sleep Med. 2021.
Neuman SB. The displacement effect: assessing the relation between television viewing and Reading performance. Read Res Q. 1988;23(4):414–40. https://doi.org/10.2307/747641.
Baumeister RF, Vohs KD, Tice DM. The strength model of self-control. Curr Dir Psychol Sci. 2007;16(6):351–5. https://doi.org/10.1111/j.1467-8721.2007.00534.x.
Rebetez MML, Rochat L, Barsics C, Van der Linden M. Procrastination as a self-regulation failure: the role of inhibition, negative affect, and gender. Personal Individ Differ. 2016;101:435–9. https://doi.org/10.1016/j.paid.2016.06.049.
Márquez-Hernández VV, Gutiérrez-Puertas L, Granados-Gámez G, Gutiérrez-Puertas V, Aguilera-Manrique G. Problematic mobile phone use, nomophobia and decision-making in nursing students mobile and decision-making in nursing students. Nurse Educ Pract. 2020;49:102910. https://doi.org/10.1016/j.nepr.2020.102910.
Kroese FM, Evers C, Adriaanse MA, de Ridder DT. Bedtime procrastination: a self-regulation perspective on sleep insufficiency in the general population. J Health Psychol. 2016;21(5):853–62. https://doi.org/10.1177/1359105314540014.
Zhang MX, Wu AMS. Effects of smartphone addiction on sleep quality among Chinese university students: The mediating role of self-regulation and bedtime procrastination. Addict Behav. 2020;111:106552.
Yang X, Wang P, Hu P. Trait procrastination and Mobile phone addiction among Chinese college students: a moderated mediation model of stress and gender. Front Psychol. 2020;11:3318. https://doi.org/10.3389/fpsyg.2020.614660.
Rozgonjuk D, Kattago M, Taht K. Social media use in lectures mediates the relationship between procrastination and problematic smartphone use. Comput Hum Behav. 2018;89:191–8. https://doi.org/10.1016/j.chb.2018.08.003.
Deary IJ. The trait approach to personality. In: PJCaIG M, editor. The Cambridge handbook of personality. New York: Cambridge University Press; 2009.
Guo J, Meng D, Ma X, Zhu L, Yang L, Mu L. The impact of bedtime procrastination on depression symptoms in Chinese medical students. Sleep Breath. 2020;24(3):1247–55. https://doi.org/10.1007/s11325-020-02079-0.
Wong ML, Lau EYY, Wan JHY, Cheung SF, Hui CH, Mok DSY. The interplay between sleep and mood in predicting academic functioning, physical health and psychological health: a longitudinal study. J Psychosom Res. 2013;74(4):271–7. https://doi.org/10.1016/j.jpsychores.2012.08.014.
Glozier N, O’Dea B, McGorry PD, Pantelis C, Amminger GP, Hermens DF, et al. Delayed sleep onset in depressed young people. BMC Psychiatry. 2014;14(1):33. https://doi.org/10.1186/1471-244X-14-33.
Tochigi M, Usami S, Matamura M, Kitagawa Y, Fukushima M, Yonehara H, et al. Annual longitudinal survey at up to five time points reveals reciprocal effects of bedtime delay and depression/anxiety in adolescents. Sleep Med. 2016;17:81–6. https://doi.org/10.1016/j.sleep.2015.08.024.
Sirois FM, Melia-Gordon ML, Pychyl TA. “I'll look after my health, later”: An investigation of procrastination and health. Personal Individ Differ. 2003;35(5):1167–84. https://doi.org/10.1016/S0191-8869(02)00326-4.
Li X, Buxton OM, Kim Y, Haneuse S, Kawachi I. Do procrastinators get worse sleep? Cross-sectional study of US adolescents and young adults. SSM Popul Health. 2020;10:100518. https://doi.org/10.1016/j.ssmph.2019.100518.
Ma X, Meng D, Zhu L, Xu H, Guo J, Yang L, et al. Bedtime procrastination predicts the prevalence and severity of poor sleep quality of Chinese undergraduate students. J Am Coll Heal. 2020:1–8. https://doi.org/10.1080/07448481.2020.1785474.
Li G, **e J, An L, Hou G, Jian H, Wang W. A generalizability analysis of the Mobile phone addiction tendency scale for Chinese college students. Front Psychiatry. 2019;10:241. https://doi.org/10.3389/fpsyt.2019.00241.
Kroese FM, De Ridder DT, Evers C, Adriaanse MA. Bedtime procrastination: introducing a new area of procrastination. Front Psychol. 2014;5:611. https://doi.org/10.3389/fpsyg.2014.00611.
Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. https://doi.org/10.1016/0165-1781(89)90047-4.
Zheng B, Li M, Wang KL, Lv J. Analysis of the reliability and validity of the Chinese version of Pittsburgh sleep quality index among medical college students. J Peking Univ Health Sci. 2016;48(3):424–8.
Löwe B, Kroenke K, Herzog W, Gräfe K. Measuring depression outcome with a brief self-report instrument: sensitivity to change of the patient Health questionnaire (PHQ-9). J Affect Disord. 2004;81(1):61–6. https://doi.org/10.1016/S0165-0327(03)00198-8.
Wang W, Bian Q, Zhao Y, Li X, Wang W, Du J, et al. Reliability and validity of the Chinese version of the patient Health questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–44. https://doi.org/10.1016/j.genhosppsych.2014.05.021.
Meredith W. Measurement invariance, factor analysis and factorial invariance. Psychometrika. 1993;58(4):525–43. https://doi.org/10.1007/BF02294825.
Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. 1999;6(1):1–55. https://doi.org/10.1080/10705519909540118.
Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res Online. 2003;8(2):23–74.
Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Model Multidiscip J. 2007;14(3):464–504. https://doi.org/10.1080/10705510701301834.
Raudsepp L. Brief report: problematic social media use and sleep disturbances are longitudinally associated with depressive symptoms in adolescents. J Adolesc. 2019;76:197–201. https://doi.org/10.1016/j.adolescence.2019.09.005.
Park SY, Yang S, Shin CS, Jang H, Park SY. Long-Term Symptoms of Mobile Phone Use on Mobile Phone Addiction and Depression Among Korean Adolescents. Int J Environ Res Public Health. 2019;16(19).
Lapierre MA, Zhao P, Custer BE. Short-term longitudinal relationships between smartphone Use/dependency and psychological well-being among late adolescents. J Adolesc Health. 2019;65(5):607–12. https://doi.org/10.1016/j.jadohealth.2019.06.001.
Coyne SM, Stockdale L, Summers K. Problematic cell phone use, depression, anxiety, and self-regulation: evidence from a three year longitudinal study from adolescence to emerging adulthood. Comput Hum Behav. 2019;96:78–84. https://doi.org/10.1016/j.chb.2019.02.014.
Breslau N, Roth T, Rosenthal L, Andreski P. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry. 1996;39(6):411–8. https://doi.org/10.1016/0006-3223(95)00188-3.
Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–32. https://doi.org/10.1111/jcmm.14170.
Harvey AG, Murray G, Chandler RA, Soehner A. Sleep disturbance as transdiagnostic: consideration of neurobiological mechanisms. Clin Psychol Rev. 2011;31(2):225–35. https://doi.org/10.1016/j.cpr.2010.04.003.
**e X, Dong Y, Wang J. Sleep quality as a mediator of problematic smartphone use and clinical health symptoms. J Behav Addict. 2018;7(2):466–72. https://doi.org/10.1556/2006.7.2018.40.
Lee JE, Jang SI, Ju YJ, Kim W, Lee HJ, Park EC. Relationship between Mobile phone addiction and the incidence of poor and short sleep among Korean adolescents: a longitudinal study of the Korean Children & Youth Panel Survey. J Korean Med Sci. 2017;32(7):1166–72. https://doi.org/10.3346/jkms.2017.32.7.1166.
Tamura H, Nishida T, Tsuji A, Sakakibara H. Association between Excessive Use of Mobile Phone and Insomnia and Depression among Japanese Adolescents. Int J Environ Res Public Health. 2017;14(7).
Yu SJ, Cao YJ, Ma DD. A survey on night sleep quality and daytime tiredness among shift nurses in a tertiary teaching hospital. Chin J Industrial Hyg Occup Dis. 2018;36(11):855–8. https://doi.org/10.3760/cma.j.issn.1001-9391.2018.11.016.
Komarov O, Ko LW, Jung TP. Associations among emotional state, sleep quality, and resting-state EEG spectra: a longitudinal study in graduate students. IEEE Trans Neural Syst Rehabil Eng. 2020;28(4):795–804. https://doi.org/10.1109/TNSRE.2020.2972812.
Sirois FM. “I’ll look after my health, later”: a replication and extension of the procrastination–health model with community-dwelling adults. Personal Individ Differ. 2007;43(1):15–26. https://doi.org/10.1016/j.paid.2006.11.003.
Steel P. The nature of procrastination: a meta-analytic and theoretical review of quintessential self-regulatory failure. Psychol Bull. 2007;133(1):65–94. https://doi.org/10.1037/0033-2909.133.1.65.
Hong W, Liu RD, Ding Y, Jiang S, Yang X, Sheng X. Academic procrastination precedes problematic mobile phone use in Chinese adolescents: a longitudinal mediation model of distraction cognitions. Addict Behav. 2021;121:106993. https://doi.org/10.1016/j.addbeh.2021.106993.
Tucker MA, Hirota Y, Wamsley EJ, Lau H, Chaklader A, Fishbein W. A daytime nap containing solely non-REM sleep enhances declarative but not procedural memory. Neurobiol Learn Mem. 2006;86(2):241–7. https://doi.org/10.1016/j.nlm.2006.03.005.
Barnes CM. Working in our sleep: sleep and self-regulation in organizations. Organ Psychol Rev. 2012;2(3):234–57. https://doi.org/10.1177/2041386612450181.
Altena E, Van Der Werf YD, Sanz-Arigita EJ, Voorn TA, Rombouts SA, Kuijer JP, et al. Prefrontal hypoactivation and recovery in insomnia. Sleep. 2008;31(9):1271–6.
Amini M, Saboory E, Derafshpour L, Fakhari A, Wu JC, Bruggeman R, et al. The impact of sleep deprivation on sexual behaviors and FAAH expression in the prefrontal cortex of male rats. Neurosci Lett. 2020;735:135254. https://doi.org/10.1016/j.neulet.2020.135254.
Chee MW, Choo WC. Functional imaging of working memory after 24 hr of total sleep deprivation. J Neurosci. 2004;24(19):4560–7. https://doi.org/10.1523/JNEUROSCI.0007-04.2004.
Nilsson JP, Söderström M, Karlsson AU, Lekander M, Akerstedt T, Lindroth NE, et al. Less effective executive functioning after one night's sleep deprivation. J Sleep Res. 2005;14(1):1–6. https://doi.org/10.1111/j.1365-2869.2005.00442.x.
van Noordt SJR, Segalowitz SJ. Performance monitoring and the medial prefrontal cortex: a review of individual differences and context effects as a window on self-regulation. Front Hum Neurosci. 2012;6. https://doi.org/10.3389/fnhum.2012.00197.
Hofmann W, Schmeichel BJ, Baddeley AD. Executive functions and self-regulation. Trends Cogn Sci. 2012;16(3):174–80. https://doi.org/10.1016/j.tics.2012.01.006.
Kühnel J, Bledow R, Feuerhahn N. When do you procrastinate? Sleep quality and social sleep lag jointly predict self-regulatory failure at work. J Organ Behav. 2016;37(7):983–1002. https://doi.org/10.1002/job.2084.
van Eerde W, Venus M. A daily diary study on sleep quality and procrastination at work: the moderating role of trait self-control. Front Psychol. 2018;9:2029. https://doi.org/10.3389/fpsyg.2018.02029.
Tice DM, Baumeister RF. Longitudinal study of procrastination, performance, stress, and Health: the costs and benefits of dawdling. Psychol Sci. 1997;8(6):454–8. https://doi.org/10.1111/j.1467-9280.1997.tb00460.x.
Klingsieck KB. Procrastination when good things Don’t come to those who wait. Eur Psychol. 2013;18(1):24–34. https://doi.org/10.1027/1016-9040/a000138.
Sirois F, Pychyl T. Procrastination and the priority of short-term mood regulation: consequences for future self. Soc Personal Psychol Compass. 2013;7(2):115–27. https://doi.org/10.1111/spc3.12011.
van Velthoven MH, Powell J, Powell G. Problematic smartphone use: Digital approaches to an emerging public health problem, vol. 4. London: SAGE Publications Sage UK; 2018. p. 1–9.
Acknowledgments
The authors thank all the participants and investigators for their efforts and are grateful to the editor and reviewers for their work, as well as for their suggestions for this paper.
Funding
This study was supported by the Social Science Fund of Shandong Province (21CJYJ29). The source of funding had no role in study design, data collection, analysis, interpretation, or manuscript writing.
Author information
Authors and Affiliations
Contributions
Guanghui Cui, Shaojie Li, and Yongtian Yin designed the study; Lei Chen, **nyao Liu, Kaixuan Tang and Yawen Li collected data; Guanghui Cui and Shaojie Li analyzed the data. Guanghui Cui wrote the original manuscript, and Yongtian Yin and Shaojie Li revised it. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of the Second Affiliated Hospital of the Shandong University of Traditional Chinese Medicine, and all participants provided written informed consent. All research procedures followed the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Multimedia Appendix 1
. Model fit statistics for tests of measurement invariance.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cui, G., Yin, Y., Li, S. et al. Longitudinal relationships among problematic mobile phone use, bedtime procrastination, sleep quality and depressive symptoms in Chinese college students: a cross-lagged panel analysis. BMC Psychiatry 21, 449 (2021). https://doi.org/10.1186/s12888-021-03451-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-021-03451-4