
Abstract
Background:
What combination of risk factors for Alzheimer’s disease (AD) are most predictive of cognitive decline in cognitively unimpaired individuals remains largely unclear. We studied associations between APOE genotype, AD-Polygenic Risk Scores (AD-PRS), amyloid-β pathology and decline in cognitive functioning over time in a large sample of cognitively unimpaired older individuals.
Methods:
We included 276 cognitively unimpaired older individuals (75 ± 10 years, 63% female) from the EMIF-AD PreclinAD cohort. An AD-PRS was calculated including 83 genome-wide significant variants. The APOE gene was not included in the PRS and was analyzed separately. Baseline amyloid-β status was assessed by visual read of [18F]flutemetamol-PET standardized uptake value images. At baseline and follow-up (2.0 ± 0.4 years), the cognitive domains of memory, attention, executive function, and language were measured. We used generalized estimating equations corrected for age, sex and center to examine associations between APOE genotype and AD-PRS with amyloid-β status. Linear mixed models corrected for age, sex, center and education were used to examine associations between APOE genotype, AD-PRS and amyloid-β status, and their interaction on changes in cognitive functioning over time.
Results:
Fifty-two participants (19%) had abnormal amyloid-β, and 84 participants (31%) carried at least one APOE ε4 allele. APOE genotype and AD-PRS were both associated with abnormal amyloid-β status. Increasingly more risk-full APOE genotype, a high AD-PRS and an abnormal amyloid-β status were associated with steeper decline in memory functioning in separate models (all p ≤ 0.02). A model including 4-way interaction term (APOE×AD-PRS×amyloid-β×time) was not significant. When modelled together, both APOE genotype and AD-PRS predicted steeper decline in memory functioning (APOE β(SE)=-0.05(0.02); AD-PRS β(SE)=-0.04(0.01)). Additionally, when modelled together, both amyloid-β status and AD-PRS predicted a steeper decline in memory functioning (amyloid-β β(SE)=-0.07(0.04); AD-PRS β(SE)=-0.04(0.01)). Modelling both APOE genotype and amyloid-β status, we observed an interaction, in which APOE genotype was related to steeper decline in memory and language functioning in amyloid-β abnormal individuals only (β(SE)=-0.13(0.06); β(SE)=-0.22(0.07), respectively).
Conclusion:
Our results suggest that APOE genotype is related to steeper decline in memory and language functioning in individuals with abnormal amyloid-β only. Furthermore, independent of amyloid-β status other genetic risk variants contribute to memory decline in initially cognitively unimpaired older individuals.
Similar content being viewed by others


Background
Alzheimer’s disease (AD) is the most common cause of dementia. The development of AD starts with a preclinical stage where pathophysiological changes in brain amyloid-β are present, [1,2,3,4] while cognition is still intact. [5, 6] Once amyloid-β pathology is present it can take several years to decades to develop dementia. [7] AD drug development programs are shifting their focus to individuals in the earliest disease stage, because this is when individuals could benefit most from disease-modifying therapy. For this, it is important to be able to identify cognitively unimpaired individuals at risk of future cognitive decline in the ageing population.
Genetic risk factors might help to identify individuals with increased risk of develo** AD. With heritability estimates of 58–79%, late-onset AD is a highly heritable disease. [8, 9] A well-known major genetic risk factor for AD is the apolipoprotein E (APOE) ɛ4 allele. APOE ɛ4 heterozygotes are at three-fold greater risk of AD and ɛ4 homozygotes at eight- to fifteen-fold compared to APOE ɛ4 non-carriers. [10] Additionally, it has been shown that APOE ɛ4 carriers have a higher prevalence of amyloid-β pathology at younger ages relative to non-carriers [5] and that APOE ɛ4 predicts cognitive decline in healthy controls. [11, 12] However, up to 40% of AD cases do not carry an APOE ɛ4 allele and the age at onset of AD dementia in APOE ɛ4 carriers varies widely, indicating that other genes or environmental risk factors are involved in causing the disease. Genome wide association studies (GWAS) in AD showed that, in addition to APOE ɛ4, over 80 genetic variants were significantly associated with AD. [13] By combining these multiple genetic variants, a so-called ‘polygenic risk score’ (PRS) can be calculated for each individual. Typically, higher PRS scores reflect increased risk for AD. [14] In cognitively unimpaired individuals, a high AD-PRS has been shown to be associated with amyloid-β pathology [15,16,17,18] and cognitive decline. [17,18,19,20,21] However, some studies did not find an association between AD-PRS and amyloid-β pathology [16] or cognitive decline. [22,23,24] Discrepant findings could be related to variability in the proportion of amyloid-β positive individuals in cognitively unimpaired groups, which ranges from 24 to 33%[5]. Other explanations for discordant results could be related to the number of genetic variants included in the AD-PRS, variability of cognitive tasks or composite scores used, or the follow-up duration. Furthermore, some studies included the APOE genotype in the AD-PRS, while other studies did not [16, 25,26,27]. Thus, it remains unclear to what extent the independent aspects of amyloid-β, APOE genotype and AD-PRS are related to cognitive decline in cognitively unimpaired individuals.
The aim of the present study was to investigate how APOE genotype, AD-PRS (APOE region excluded) and amyloid-β pathology relate to decline in cognition over time in cognitively unimpaired older individuals, and whether such effects are observed for specific cognitive domains (i.e., memory, attention, executive function and language).
Methods
Participants
Participants were part of the EMIF-AD PreclinAD study, which is a study investigating risk factors for amyloid-β pathology and cognitive decline in cognitively unimpaired older adults. [28] The PreclinAD study recruited participants from two sites: the Manchester and Newcastle Age and Cognitive Performance Research Cohort (ACPRC) in Manchester [29] and the Netherlands Twin Register (NTR) [30] in Amsterdam. Baseline inclusion criteria for the EMIF-AD PreclinAD study were age ≥ 60 years, Telephone Interview for Cognitive Status modified score of ≥ 23, [31] delayed recall score > − 1.5 SD of demographics-adjusted normative data on the Consortium to Establish a Registry for Alzheimer’s Disease 10-word list, [32] global Clinical Dementia Rating (CDR) score of 0, with a score of 0 on the memory sub domain [33] and a 15-item Geriatric Depression Scale score of < 11. [34] Baseline exclusion criteria were any neurological, systemic or psychiatric disorder that could cause cognitive impairment. Included participants had cognitive data available, an AD-PRS, an amyloid-β positron emission tomography (PET)-scan and/or APOE genotype data at their baseline visit (n = 276, of which 97 were complete twin pairs). All participants underwent an extensive baseline assessment including Mini-Mental State Examination (MMSE), neuropsychological assessment, acquiring years of education, and blood sampling. At two-year follow-up, MMSE, CDR and neuropsychological assessment were repeated, which were also used to monitor disease progression. According to protocol, if cognitive impairment was suspected by the study physician a neurologist was consulted and, if necessary or possible, a diagnostic work-up in the Alzheimer Center Amsterdam was performed. Each participant gave written informed consent, in accordance with the Medical Ethics Review Committee of the VU University Medical Center, the National Research Ethics Service Committee North West—Greater Manchester South and the Helsinki Declaration of 1975.
Neuropsychological assessment
In Manchester, neuropsychological testing was performed during the research facility visit at both baseline and follow-up. In Amsterdam, neuropsychological testing at baseline was performed at home, and during follow-up at the VU University Medical Center or at home when participants were unable to come to the hospital (n = 19, 10%). We used the following tests to assess memory performance: the total immediate recall and delayed recall of the Rey Auditory Verbal Learning Test (RAVLT), [35, 36] the twenty minute recall of the Rey Complex Figure Test (RCFT), [37, 38] the total errors of the Cambridge Neuropsychological Test Automated Battery (CANTAB) Paired Associate Learning (PAL) test, [39, 40] and the total score of the Face Name Associated Memory Examination (FNAME) names and occupations delayed recall. [41, 42] To assess attention, we used the Trail Making Test (TMT) part A, [43] the forward condition of the Digit Span (total span score), [44] the simple accuracy score of the CANTAB Reaction Time (RTI) test and the mean response latency of the CANTAB Rapid Visual information Processing (RVP) test. [40] To test executive function, we used the TMT part B [43] (corrected for TMT part A), the backward condition of the Digit Span (total span score), [44] letter fluency (in English testing the letters F A S and in Dutch the letters D A T [45]) and the between errors score of the CANTAB Spatial-working Memory (SWM) test. [40] For language function, we used category fluency (animal fluency) one minute and the graded naming test (GNT). [46,47,48,49] FNAME data were missing in 22 participants (8%) at baseline and in 20 participants (9%) at follow-up. CANTAB RVP data were missing in 30 participants (11%) at baseline and in 31 participants (14%) at follow-up, due to lack of time or fatigue effects. For all other tests, 0-3% of test scores were missing.
Genoty** and polygenic risk scoring
All genetic variants in our cohort were determined by applying standard genoty** and imputation methods and we applied established quality control methods. [50, 51] The genotype imputation method has been previously described. [52] In short, all individuals were genotyped using Illumina Global Screening array (GSA) with shared custom content (Illumina, Incl). We used high-quality genoty** in all individuals (individual call rate > 98%, variant call rate > 95%). All individuals’ reported sex matched with their genetic sex. Variants that departed from Hardy–Weinberg equilibrium were excluded at p < 1 × 10− 6. Genotypes were prepared for imputation using bcftools (v1.9) [53] for removing ambiguous (single nucleotide polymorphisms) SNPs, and flip** and swap** alleles to align to GRCh37/hg19. This was followed by haplotype phasing using SHAPEIT2 [54] and imputation of unobserved genotypes using Minimac3 [55] using a precompiled Haplotype Reference Consortium (HRC) reference panel. [56] We calculated a weighted individual AD-PRS based on the 83 genetic variants that showed genome-wide significant (GWS, p < 5e− 8) evidence of association with AD. [13]APOE haplotypes were not included in the AD-PRS. The selected variants were directly genotyped (median genoty** rate = 1) or imputed with high quality (median imputation score R² = 0.98, minimum R² = 0.5). The AD-PRS was generated by multiplying the genotype dosage of each risk allele for each variant by its respective weight and then summing across all variants. [57] Weights used can be found in (Table S1). [13] For analyses we used an ordinal APOE genotype variable (0 = APOE ɛ2ɛ2:ɛ2ɛ3; 1 = APOE ɛ3ɛ3; 2 = APOE ɛ2ɛ4:ɛ3ɛ4; 3 = APOE ɛ4ɛ4) and a normalized AD-PRS (mean = 0, standard deviation = 1). From all participants APOE data was missing for one participant (0.4%) and AD-PRS data was missing for five participants (1.8%). This study is independent of the discovery of the 83 genetic variants associated with AD, because participants were not included in Bellenguez et al. (2022).
Amyloid-β PET-scan
At baseline, all participants were scanned from 90 to 110 min (4 × 5 min frames) after intravenous injection of 185 MBq (± 10%) [18F]flutemetamol. [28, 58] In Manchester, PET-scans were performed on a high-resolution research tomography brain scanner (HRRT; Siemens/CTI, Knoxville, TN, USA) at the Wolfson Molecular Imaging Centre of the University of Manchester. A 7-min transmission scan using a 137Cs point source was acquired for subsequent attenuation and scatter correction of the PET data. [59] In Amsterdam, PET-scans were performed on a Philips Ingenuity TF PET-MRI (Philips Healthcare, Cleveland, USA) at the Amsterdam UMC, location VU University Medical Center. Full acquisition details have been described previously. [28, 60] Immediately prior to each part of the PET-scan, a T1-weighted gradient echo pulse MRI scan was acquired for attenuation correction of the PET data. Three GE healthcare (GEHC) certified readers (SFC in Manchester; BNMvB and LEC in Amsterdam) visually rated standardized uptake value images as amyloid-β negative (predominantly white matter uptake) or positive (binding in one or more cortical brain region or striatum unilaterally), blinded to clinical and demographic data and according to GEHC guidelines. [61] Majority visual read was applied for both Manchester and Amsterdam obtained PET-scans.
Statistical analysis
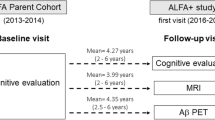
We imputed missing cognitive test scores (0–14% of participants per test) by single imputation, using predictive mean matching as method [62] with follow-up time, genetic relatedness, baseline age, sex, education, amyloid-β status, and MMSE score as predictors. After imputation, baseline and two-year follow-up individual cognitive test scores were standardized using their baseline mean and standard deviation across the total sample (n = 285) (Fig. 1). CANTAB PAL, RVP and SWM scores and the TMT part A and B scores were inverted by multiplying the z score with − 1, so that for all tests lower scores reflect worse performance. Next, we averaged z-scores of the domain specific tests into four cognitive composite scores (i.e., memory, attention, executive function, and language).

Flowchart of participant selection. None of the participants developed AD dementia or MCI between baseline and follow-up. Abbreviations: EMIF-AD = European Information Framework for Alzheimer’s Disease; amyloid-β = amyloid-beta; APOE = apolipoprotein E; PRS = polygenic risk score
First, we compared demographic variables between amyloid-β normal and amyloid-β abnormal groups using generalized estimating equations (GEE), including a random effect to account for family-relatedness in the Amsterdam cohort. We studied associations of APOE genotype (continuous dose: 0 = APOE ɛ2ɛ2:ɛ2ɛ3; 1 = APOE ɛ3ɛ3; 2 = APOE ɛ2ɛ4:ɛ3ɛ4; 3 = APOE ɛ4ɛ4) and AD-PRS (z-score) with amyloid-β status using separate GEE models (amyloid-β ~ APOE; amyloid-β ~ AD-PRS, respectively), including age, sex and center as covariates and APOE genotype and population substructure (principal components (PC) 1–3) depending on AD-PRS or APOE genotype as predictor. Next, we studied associations of APOE genotype (continuous dose), AD-PRS (z-score) and baseline amyloid-β status with changes in memory functioning over time using linear mixed effects models (LMMs). Models included subject-specific random intercepts and fixed slopes, a random effect for family, thereby correcting for clustering in the data, and were adjusted for age, sex, years of education and center. APOE genotype or population substructure (PC1-3) were added depending on using APOE genotype or AD-PRS as predictor. First, we tested with separate models the effects of APOE genotype, AD-PRS and amyloid-β status on memory decline with memory composite score as outcome (Memory ~ APOE×time; Memory ~ AD-PRS×time; Memory ~ amyloid-β×time, respectively). Next, we tested in separate models main and interaction effects of APOE genotype and AD-PRS on memory decline (Memory ~ APOE×AD-PRS×time), of APOE genotype and amyloid-β status on memory decline (Memory ~ APOE×amyloid-β×time) and AD-PRS and amyloid-β status (Memory ~ AD-PRS×amyloid-β×time). Finally, we tested the 4-way interaction of APOE×AD-PRS×amyloid-β×time on memory. Interaction terms were removed when not significant (p > 0.05). All models were repeated using cognitive composite scores of attention, executive function and language as outcome.
All analyses were corrected for multiple testing using the false discovery rate (FDR). FDR-corrected p values < 0.05 were considered significant. [63] Statistical analyses were performed in RStudio version 3.6.1 “Action of the Toes” (http://www.r-project.org/), using the following packages: mice_3.13.0, gee_4.13-20, lme4_1.1–26, lmerTest_3.1-2, emmeans_1.4.8, ggplot2_3.3.5.
Results
Demographics
We included 276 cognitively unimpaired older participants (Fig. 1) (mean age 74.7 ± 9.7, 63% female, 11.5 ± 2.7 years of education, mean follow-up 2.0 ± 0.4 years). Fifty-two participants (19%) had a positive visual read of their PET-scan. These participants were older, and had a lower composite memory, executive function and language score compared to participants with an amyloid-β negative PET-scan (Table 1).
Associations of APOE genotype and AD-PRS with amyloid-β status
Using separate models, we found that both higher APOE dose scores and higher AD-PRS were associated with a higher probability of amyloid-β positivity (odds ratio [OR] 3.99 [95% confidence interval (CI) 2.29 to 6.84], per allele; OR 1.43 [95% CI 1.02 to 2.00], respectively) (Fig. 2).

Associations between APOE genotype, AD-PRS and amyloid-β status. Values given are odds ratio [95% confidence interval] as estimated by Generalized estimating equations (predictor: APOE genotype or normalized AD-PRS; outcome: amyloid-β status (reference = amyloid-β negative status), including random effect for family-relatedness (comparable with logistic regressions, but corrected for clustering in the data), adjusted for age, sex, center, and population substructure (PC1-3). The odds ratio for the AD-PRS reflects the odds of having an amyloid-β positive status per one standard deviation increase in the AD-PRS. Amyloid-β status was based on visual read [18F]flutemetamol PET standardized uptake value images. Abbreviations: AD = Alzheimer’s Disease; APOE = apolipoprotein E; CI = confidence interval; OR = odds ratio; PC = principal components; PRS = polygenic risk score
Associations of APOE genotype, AD-PRS and amyloid-β with cognitive functioning
At baseline, no significant associations were observed between APOE genotype, AD-PRS and amyloid-β status with memory performance. Across the total group, memory scores declined over two years (β(SE) = -0.03(0.01), p = 0.04). Higher APOE dose was associated with steeper decline in memory functioning (β(SE) = -0.05(0.02), p = 0.008; Table 2; Fig. 3 A). Individuals with a high AD-PRS showed steeper decline in memory functioning over time than individuals with low AD-PRS (β(SE) = -0.04(0.01), p = 0.006; Table 2; Fig. 3B). Individuals with abnormal amyloid-β showed steeper decline in memory functioning over time than individuals with normal amyloid-β (β(SE) = -0.08(0.04), p = 0.02; Table 2; Fig. 3 C). We then examined the interactions of APOE genotype and AD-PRS on the rate of memory decline, which was not significant. Repeating analyses including APOE genotype and AD-PRS as main effects in the same model, we found that both higher APOE genotype dosage and a high AD-PRS were associated with steeper decline in memory over time (Table 2). When examining interactions of APOE genotype dosage and amyloid-β status on the rate of memory decline, we found a significant interaction effect (p-interaction = 0.02) (Fig. 4). Repeating analyses after stratifying for amyloid-β status, we found that a higher APOE dose was associated with steeper memory decline in individuals with abnormal amyloid-β (β(SE) = -0.13(0.06), p = 0.03), and no association was found in individuals with normal amyloid-β (β(SE) = -0.02(0.02), p = 0.46; Table 2). When examining interactions of AD-PRS and amyloid-β status on the rate of memory decline, no significant effects were found. Repeating analyses including AD-PRS and amyloid-β status as main effects in the same model, we found that both abnormal amyloid-β and high AD-PRS were related to steeper decline in memory over time (Table 2). The model including the 4-way interaction term (APOE×AD-PRS×amyloid-β×time) was not significant. After removing ɛ2ɛ4 carriers from the sample, the results and interpretation did not change (Table S2).

Effects of APOE genotype, AD-PRS and amyloid-β status on changes in memory composite scores. Model-based estimation of longitudinal changes in memory composite score, based on APOE genotype (A), polygenic risk score (PRS) for Alzheimer’s Disease (B) and amyloid-β status (C). Neuropsychological tests were z-transformed and averaged for the composite memory score. APOE genotype dosage variable used as factor for plots: ɛ2 heterozygous/homozygous (APOE ɛ2ɛ2:ɛ2ɛ3), ɛ3ɛ3 (APOE ɛ3ɛ3), ɛ4 heterozygous (APOE ɛ2ɛ4:ɛ3ɛ4) and ɛ4 homozygous (APOE ɛ4ɛ4). AD-PRS depicted in tertiles. Amyloid-β status was based on visual read [18F]flutemetamol PET standardized uptake value images. Fixed-effect covariates were baseline age, sex, education, center and population substructure. For statistics see Table 2. AD = Alzheimer’s disease; APOE = apolipoprotein E; PET = positron emission tomography; PRS = polygenic risk score

Interaction effects between APOE genotype and amyloid-β status with memory functioning over time. Amyloid-β status was based on visual read [18F]flutemetamol PET standardized uptake value images. APOE dosage variable used as factor for plots: ɛ2 heterozygous/homozygous (APOE ɛ2ɛ2:ɛ2ɛ3, n = 34), ɛ3ɛ3 (APOE ɛ3ɛ3, n = 157), ɛ4 heterozygous (APOE ɛ2ɛ4:ɛ3ɛ4, n = 77) and ɛ4 homozygous (APOE ɛ4ɛ4, n = 7). Neuropsychological tests were z-transformed and averaged for the composite memory score. Interaction effect was statistically significant, see Table 2. Abbreviations: APOE = apolipoprotein E
Examining composite attention, executive function and language scores, we found across the whole group all scores improved over two years (attention: β(SE) = 0.05(0.02), p = 0.02; executive function: β(SE) = 0.06(0.02), p = 0.004; language: β(SE) = 0.11(0.02), p < 0.001). However, individuals with higher APOE dose showed steeper decline in language functioning (β(SE) = -0.07(0.03), p = 0.04; Table S3, Figure S1G). When examining interactions of APOE genotype and AD-PRS as main effects in the same model, we found that higher APOE genotype dosage was associated with steeper decline in language over time, while AD-PRS was not (Table S3). We then examined interactions of APOE genotype dosage and amyloid-β status on the rate of language decline, and we found a significant interaction effect (p-interaction = 0.003) (Figure S2). Repeating analyses after stratifying for amyloid-β status, we found that higher APOE dose was associated with steeper language decline in individuals with abnormal amyloid-β (β(SE) = -0.22(0.07), p = 0.002), and no association was found in individuals with normal amyloid-β (β(SE) = -0.02(0.04), p = 0.62; Table S3). No significant associations were found for APOE genotype, AD-PRS and amyloid-β status with attention and executive function performance over time.
Discussion
In a cognitively unimpaired older population, we found that both higher APOE genotype dosage and higher AD-PRS were related to amyloid-β abnormality. Furthermore, we observed in separate models that AD-PRS, APOE genotype dosage and abnormal amyloid-β were associated with steeper decline in memory functioning over time in separate models. The association of higher APOE genotype dosage with steeper memory decline was dependent on amyloid-β abnormality, whereas AD-PRS explained variance in memory decline over time independently of APOE genotype dosage and amyloid-β status. In addition, APOE genotype dosage was associated with steeper decline in language functioning over time, and this association was dependent on amyloid-β abnormality. These results suggest that amyloid-β status, APOE genotype and AD-PRS all explain parts of cognitive decline in older individuals with initially normal cognition.
Our findings that both higher APOE genotype dosage and higher AD-PRS were associated with amyloid-β pathology replicates previous findings in cognitively unimpaired individuals. [64, 65] This suggests that besides APOE ɛ4 other genes may contribute to amyloid-β abnormality. Pathway-enrichment analyses [13] of the SNPs that were included in the AD-PRS showed most significant genes to be related to amyloid-β and tau, but also to lipid metabolism and immunity, highlighting the role of microglia and its potential interaction with amyloid precursor protein (APP) metabolism in AD development. [66]
At baseline, none of the variables examined were associated with memory performance as measured by a composite consisting of five memory tests. We previously did find an association between abnormal amyloid-β and lower baseline RCFT 3-minute recall scores in the Amsterdam cohort of the EMIF-AD preclinAD study. [67] Combining the two EMIF-AD cohorts in the sample of this study, using a composite memory score that combines multiple tests instead of separate tests and assessing associations with LMMs instead of GEEs may explain the different findings. When examining memory performance over time, we observed that an abnormal amyloid-β status was related to steeper decline in memory functioning over time compared to a normal amyloid-β status, which is in line with previous preclinical AD studies. [68,69,70] We also found that both a high AD-PRS and high APOE genotype dosage was related to decline in memory functioning over time. This observation is largely consistent with earlier studies in cognitively unimpaired individuals. [18, 19, 22, 24, 71] We further extend the literature by showing that APOE genotype dosage and high AD-PRS explained variance in memory decline independently. Further research is needed to understand whether specific risk genes contribute to the rate of cognitive decline in preclinical AD. While the effect of high APOE genotype dosage was specific for individuals with abnormal amyloid-β (which is in line with a previous study [72]), the high AD-PRS was related to steeper memory decline independently of amyloid-β status. Possibly, some SNPs included in the AD-PRS reflect risk for cognitive decline, through pathways which might be unrelated to amyloid-β pathology. Previous studies using pathway analysis methods on AD GWAS results showed that genetic variants linked to AD risk were associated with the immune system, [73] endocytosis, cholesterol metabolism, amyloid-β clearance and tau metabolism. [74, 75] Future research should investigate if pathway-specific PRSs contribute to distinct aspects of cognitive decline in AD. Additionally, APOE genotype dosage was associated with decline in language performance over time, dependent on amyloid-β abnormality. We previously showed in cognitively unimpaired individuals that the very first cognitive changes in the early stages of AD are to be found in memory and language domains. [76] As all cognitive scores improved over two years, reflecting learning effects, and we found no relation between APOE genotype, AD-PRS and amyloid-β status and decline on attention and executive function, it is possible with a longer follow-up period these individuals may start to show decline in these domains as well. Furthermore, our study evaluated genetic risk factors for AD development while previous population studies indicated that environmental factors also influence dementia risk. [77] We previously showed environmental factors to contribute to onset of amyloid-β aggregation, but not particularly to cognitive decline. [76] For future research, it will be of interest to investigate the contribution of risk genes and their possible interaction with environmental risk factors to AD development.
A strength of the present study is the relatively large sample of cognitively unimpaired older individuals with a substantial age range (60–94), AD biomarkers, genetic risk data, and repeated neuropsychological assessment available. Possible limitations are that by using a dichotomous variable for amyloid-β burden, more sensitive information could have been lost, because binary visual reads disregard the potential significance of quantifying early, pathological, amyloid-β accumulation. [78] In relation to APOE genotypes, we placed both APOE ɛ2ɛ4 and ɛ3ɛ4 carriers into the same category of the APOE genotype variable even though previous studies have shown that ɛ3ɛ4 carriers may have worse outcomes than ɛ2ɛ4 carriers. [79] However, removing ɛ2ɛ4 carriers from our sample did not change the results nor interpretation (Table S2). Since it has been shown that predictive performance of AD-PRS based on European samples is lower in non-European ancestry samples, [80] our results might not be directly generalizable due to the fact our study was solely based on a European sample. Although AD-PRS was associated with steeper memory decline in our study, effect sizes were small, which may limit its potential clinical use. Additionally, none of the participants progressed to mild cognitive impairment or dementia yet. In this study, 50 participants did not complete follow-up assessment and their current cognitive status is unknown. Comparing their baseline characteristics to remaining individuals in the study showed that they were older and were more often female and APOE ɛ4 carriers compared to the 226 individuals who were assessed at follow-up (see Table S4). The follow-up duration of an average of two years may have been too short to observe decline or clinical progression in initially cognitively unimpaired individuals, who take on average 5–6 years to show decline or clinical progression. [81] For this reason we aim to continue following our cohort.
Conclusion
Our findings provide further support among cognitively unimpaired older individuals that, in addition to abnormal amyloid-β and APOE genotype, the AD-PRS is also associated with memory decline. Future research should further investigate which specific genetic variants contribute to memory decline and through which mechanism, because this will be important for develo** treatments that may prevent decline in cognition.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request and after signing a material transfer agreement.
Abbreviations
- AD:
-
Alzheimer’s disease
- APOE :
-
apolipoprotein E
- APP:
-
amyloid precursor protein
- CANTAB:
-
Cambridge Neuropsychological Test Automated Battery
- CI:
-
confidence interval
- FNAME:
-
Face Name Associated Memory Examination
- GEE:
-
generalized estimating equations
- GEHC:
-
GE Healthcare
- GSA:
-
Global Screening array
- GWAS:
-
Genome Wide Association Studies
- LMM:
-
linear mixed effects models
- MMSE:
-
Mini-Mental State Examination
- OR:
-
odds ratio
- PAL:
-
Paired Associate Learning
- PC:
-
Population Substructure
- PET:
-
positron emission tomography
- PRS:
-
Polygenic Risk Scores
- RAVLT:
-
Rey Auditory Verbal Learning Test
- RCFT:
-
Rey Complex Figure Test
- SNPs:
-
single nucleotide polymorphisms
References
Jack CRJ, et al. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. The lancet neurology. 2013;12.2: 207-216.
Gordon BA, et al. Spatial patterns of neuroimaging biomarker change in individuals from families with autosomal dominant Alzheimer’s disease: a longitudinal study. Lancet Neurol. 2018;17:241–50.
Bateman RJ, et al. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N Engl J Med. 2012;367:795–804. doi:https://doi.org/10.1056/NEJMoa1202753.
Tomlinson BE, Blessed G, Roth M. Observations on the brains of non-demented old people. J Neurol Sci. 1968;7:331–56.
Jansen WJ, et al. Prevalence Estimates of Amyloid Abnormality Across the Alzheimer Disease Clinical Spectrum. JAMA Neurol. 2022. doi:https://doi.org/10.1001/jamaneurol.2021.5216.
Donohue MC, et al. Association Between Elevated Brain Amyloid and Subsequent Cognitive Decline Among Cognitively Normal Persons. JAMA. 2017;317:2305–16. doi:https://doi.org/10.1001/jama.2017.6669.
Sperling RA, et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & dementia. 2011;7.3: 280-292.
Gatz M, et al. Role of genes and environments for explaining Alzheimer disease. Arch Gen Psychiatry. 2006;63:168–74. doi:https://doi.org/10.1001/archpsyc.63.2.168.
Dubois B, et al. Preclinical Alzheimer’s disease: definition, natural history, and diagnostic criteria. Alzheimer’s Dement. 2016;12:292–323.
Corder EH, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science. 1993;261:921–3.
Caselli RJ, et al. Cognitive domain decline in healthy apolipoprotein E ε4 homozygotes before the diagnosis of mild cognitive impairment. Arch Neurol. 2007;64:1306–11.
Lim YY, et al. APOE ε4 moderates amyloid-related memory decline in preclinical Alzheimer’s disease. Neurobiol Aging. 2015;36:1239–44. doi:https://doi.org/10.1016/j.neurobiolaging.2014.12.008.
Bellenguez C, et al. New insights into the genetic etiology of Alzheimer’s disease and related dementias. Nature genetics. 2022:1–25.
Scheltens P, et al. Alzheimer’s disease. The Lancet. 2021;397:1577–90.
Ebenau JL, et al. Risk of dementia in APOE ε4 carriers is mitigated by a polygenic risk score. Alzheimer’s & Dementia: Diagnosis Assessment & Disease Monitoring. 2021;13:e12229.
Darst BF, et al. Pathway-specific polygenic risk scores as predictors of amyloid-β deposition and cognitive function in a sample at increased risk for Alzheimer’s disease. J Alzheimers Dis. 2017;55:473–84.
Mormino EC, et al. Polygenic risk of Alzheimer disease is associated with early- and late-life processes. Neurology. 2016;87:481–8. doi:https://doi.org/10.1212/WNL.0000000000002922.
Porter T, et al. Utility of an Alzheimer’s disease risk-weighted polygenic risk score for predicting rates of cognitive decline in preclinical Alzheimer’s disease: a prospective longitudinal study. J Alzheimers Dis. 2018;66:1193–211.
Carrasquillo MM, et al. Late-onset Alzheimer’s risk variants in memory decline, incident mild cognitive impairment, and Alzheimer’s disease. Neurobiol Aging. 2015;36:60–7.
Skoog I, et al. A non-APOE polygenic risk score for Alzheimer’s disease is associated with CSF neurofilament light in a representative sample of cognitively unimpaired 70-year-olds. The Journals of Gerontology: Series A (2021).
Marden JR, et al. Using an Alzheimer’s Disease polygenic risk score to predict memory decline in black and white Americans over 14 years of follow-up Running head: AD polygenic risk score predicting memory decline. Alzheimer Dis Assoc Disord. 2016;30:195.
Verhaaren BF, et al. Alzheimer’s disease genes and cognition in the nondemented general population. Biol Psychiatry. 2013;73:429–34.
Andrews SJ, Das D, Cherbuin N, Anstey KJ, Easteal S. Association of genetic risk factors with cognitive decline: the PATH through life project. Neurobiol Aging. 2016;41:150–8.
Riaz M, et al. Effect of APOE and a polygenic risk score on incident dementia and cognitive decline in a healthy older population. Aging Cell. 2021;20:e13384.
Ge T, et al. Dissociable influences of < em > APOE</em > ε4 and polygenic risk of AD dementia on amyloid and cognition. Neurology. 2018;90:e1605–12. doi:https://doi.org/10.1212/wnl.0000000000005415.
Tan CH, et al. Polygenic hazard score: an enrichment marker for Alzheimer’s associated amyloid and tau deposition. Acta Neuropathol. 2018;135:85–93.
Cruchaga C, et al. Polygenic risk score of sporadic late-onset Alzheimer’s disease reveals a shared architecture with the familial and early-onset forms. Alzheimer’s Dement. 2018;14:205–14.
Konijnenberg E, et al. The EMIF-AD PreclinAD study: study design and baseline cohort overview. Alzheimers Res Ther. 2018;10:75. doi:https://doi.org/10.1186/s13195-018-0406-7.
Rabbitt PMA, et al. The University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age, 1983 through 2003. Aging Neuropsychol Cognition. 2004;11:245–79. doi:https://doi.org/10.1080/13825580490511116.
Willemsen G, et al. The Adult Netherlands Twin Register: twenty-five years of survey and biological data collection. Twin Res Hum Genet. 2013;16:271–81. doi:https://doi.org/10.1017/thg.2012.140.
de Jager CA, Budge MM, Clarke R. Utility of TICS‐M for the assessment of cognitive function in older adults. International journal of geriatric psychiatry. 2003;18.4:318-324.
Morris, JC, et al. The consortium to establish a registry for Alzheimer’s disease (CERAD): I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology. 1989
Morris, JC. Current vision and scoring rules the clinical dementia rating (CDR). Neurology. 1993;43:2412-2414.
Yesavage, JA, et al. Development and validation of a geriatric depression screening scale: a preliminary report. Journal of psychiatric research. 1982;17.1:37-49.
Saan R, Deelman B De 15-woordentest A en B (een voorlopige handleiding). Groningen: Afdeling Neuropsychologie, AZG (1986).
Rey A L’examen clinique en psychologie [Clinical psychological examination] Presses Universitaires de France. Paris, France (1964).
Meyers JE, Bayless JD, Meyers KR. Rey complex figure: memory error patterns and functional abilities. Applied Neuropsychology. 1996;3.2:89-92.
Snitz BE, et al. Cognitive trajectories associated with beta-amyloid deposition in the oldest-old without dementia. Neurology. 2013;80:1378–84. doi:https://doi.org/10.1212/WNL.0b013e31828c2fc8.
Reijs BLR, et al. Memory Correlates of Alzheimer’s Disease Cerebrospinal Fluid Markers: A Longitudinal Cohort Study. J Alzheimers Dis. 2017;60:1119–28. doi:https://doi.org/10.3233/Jad-160766.
Robbins TW, et al. Cambridge Neuropsychological Test Automated Battery (CANTAB): a factor analytic study of a large sample of normal elderly volunteers. Dement Geriatr Cogn Disord. 1994;5:266–81.
Papp KV, et al. Development of a Psychometrically Equivalent Short Form of the Face-Name Associative Memory Exam for use Along the Early Alzheimer’s Disease Trajectory. Clin Neuropsychologist. 2014;28:771–85. doi:https://doi.org/10.1080/13854046.2014.911351.
Rentz, DM, et al. Face-name associative memory performance is related to amyloid burden in normal elderly. Neuropsychologia. 2011;49.9:2776-2783.
Reitan, RM. Validity of the Trail Making Test as an indicator of organic brain damage. Perceptual and motor skills. 1958;8.3:271-276.
Wechsler, D. Wechsler adult intelligence scale-revised (WAIS-R). Psychological Corporation. 1981.
Schmand B, Groenink SC, van den Dungen M. [Letter fluency: psychometric properties and Dutch normative data]. Tijdschr Gerontol Geriatr. 2008;39:64–76. doi:https://doi.org/10.1007/bf03078128.
Lindeboom J, Schmand B, Tulner L, Walstra G, Jonker C. J Neurol Neurosurg Psychiatry. 2002;73:126–33.
McKenna P, Warrington EK. J Neurol Neurosurg Psychiatry. 1980;43:781–8.
Van der Elst W, Van Boxtel MPJ, Van Breukelen GJP, Jolles J. The Stroop Color-Word Test: Influence of Age, Sex, and Education; and Normative Data for a Large Sample Across the Adult Age Range. Assessment. 2006;13:62–79. doi:https://doi.org/10.1177/1073191105283427.
Bird CM, Papadopoulou K, Ricciardelli P, Rossor MN, Cipolotti L. Monitoring cognitive changes: Psychometric properties of six cognitive tests. Br J Clin Psychol. 2004;43:197–210. doi:https://doi.org/10.1348/014466504323088051.
Bos I, et al. The EMIF-AD Multimodal Biomarker Discovery study: design, methods and cohort characteristics. Alzheimers Res Ther. 2018;10:64. doi:https://doi.org/10.1186/s13195-018-0396-5.
Hong S, et al. Genome-wide association study of Alzheimer’s disease CSF biomarkers in the EMIF-AD Multimodal Biomarker Discovery dataset. Translational Psychiatry. 2020;10:403. doi:https://doi.org/10.1038/s41398-020-01074-z.
Tesi N, et al. Immune response and endocytosis pathways are associated with the resilience against Alzheimer’s disease. Translational psychiatry. 2020;10:1–12.
Narasimhan V, et al. BCFtools/RoH: a hidden Markov model approach for detecting autozygosity from next-generation sequencing data. Bioinformatics. 2016;32:1749–51.
Delaneau O, Marchini J, Zagury J-F. A linear complexity phasing method for thousands of genomes. Nat Methods. 2012;9:179–81. doi:https://doi.org/10.1038/nmeth.1785.
Das S, et al. Next-generation genotype imputation service and methods. Nat Genet. 2016;48:1284–7. doi:https://doi.org/10.1038/ng.3656.
McCarthy S, et al Haplotype Reference, C.(2016). A reference panel of 64,976 haplotypes for genotype imputation. Nat Genet48, 1279–1283.
Dudbridge F. Power and predictive accuracy of polygenic risk scores. PLoS Genet. 2013;9:e1003348.
Nelissen N, et al. Phase 1 Study of the Pittsburgh Compound B Derivative 18F-Flutemetamol in Healthy Volunteers and Patients with Probable Alzheimer Disease. J Nucl Med. 2009;50:1251–9. doi:https://doi.org/10.2967/jnumed.109.063305.
Sibomana M, et al. in IEEE Symposium Conference Record Nuclear Science 2004. 2647–2651 (IEEE).
Collij L, et al. Assessing Amyloid Pathology in Cognitively Normal Subjects using [(18)F]Flutemetamol PET: Comparing Visual Reads and Quantitative Methods. J Nucl Med. 2018. doi:https://doi.org/10.2967/jnumed.118.211532.
GEHealthcare. EPAR product information - summary of product characteristics. (2014).
Van Buuren S, Groothuis-Oudshoorn K. mice: Multivariate imputation by chained equations in R. J Stat Softw. 2011;45:1–67.
Benjamini Y, Hochberg Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J Roy Stat Soc: Ser B (Methodol). 1995;57:289–300.
Sleegers K, et al. A 22-single nucleotide polymorphism Alzheimer’s disease risk score correlates with family history, onset age, and cerebrospinal fluid Aβ42. Alzheimer’s Dement. 2015;11:1452–60.
Lopresti BJ, et al. Influence of apolipoprotein-E genotype on brain amyloid load and longitudinal trajectories. Neurobiol Aging. 2020;94:111–20.
Bellenguez C, et al New insights on the genetic etiology of Alzheimer’s and related dementia. MedRxiv (2020).
Konijnenberg E, et al. Association of amyloid pathology with memory performance and cognitive complaints in cognitively normal older adults: a monozygotic twin study. Neurobiol Aging. 2019;77:58–65.
Mortamais M, et al. Detecting cognitive changes in preclinical Alzheimer’s disease: A review of its feasibility. Alzheimer’s Dement. 2017;13:468–92. doi:https://doi.org/10.1016/j.jalz.2016.06.2365.
Doraiswamy PM, et al. Amyloid-β assessed by florbetapir F 18 PET and 18-month cognitive decline: a multicenter study. Neurology. 2012;79:1636–44.
Landau SM, et al. Amyloid deposition, hypometabolism, and longitudinal cognitive decline. Ann Neurol. 2012;72:578–86.
De Jager PL, et al. A genome-wide scan for common variants affecting the rate of age-related cognitive decline. Neurobiol Aging 33, 1017. e1011–7. e1015 (2012).
Mormino EC, et al. Amyloid and APOE ε4 interact to influence short-term decline in preclinical Alzheimer disease. Neurology. 2014;82:1760–7.
International Genomics of Alzheimer’s Disease. C. Convergent genetic and expression data implicate immunity in Alzheimer’s disease. Alzheimers Dement. 2015;11:658–71. doi:https://doi.org/10.1016/j.jalz.2014.05.1757.
Kunkle BW, et al. Genetic meta-analysis of diagnosed Alzheimer’s disease identifies new risk loci and implicates Aβ, tau, immunity and lipid processing. Nat Genet. 2019;51:414–30.
Sims R, Hill M, Williams J. The multiplex model of the genetics of Alzheimer’s disease. Nat Neurosci. 2020;23:311–22. doi:https://doi.org/10.1038/s41593-020-0599-5.
Tomassen J, et al. Abnormal cerebrospinal fluid levels of amyloid and tau are associated with cognitive decline over time in cognitively normal older adults: A monozygotic twin study. Alzheimer’s & Dementia: Translational Research & Clinical Interventions. 2022;8:e12346. doi:https://doi.org/10.1002/trc2.12346.
Livingston G, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet. 2020;396:413–46. doi:https://doi.org/10.1016/S0140-6736(20)30367-6.
Villeneuve S, et al. Existing Pittsburgh Compound-B positron emission tomography thresholds are too high: statistical and pathological evaluation. Brain. 2015;138:2020–33.
Liu C-C, Kanekiyo T, Xu H, Bu G. Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Reviews Neurol. 2013;9:106–18.
Duncan L, et al. Analysis of polygenic risk score usage and performance in diverse human populations. Nat Commun. 2019;10:1–9.
Vermunt L, et al. Duration of preclinical, prodromal, and dementia stages of Alzheimer’s disease in relation to age, sex, and APOE genotype. Alzheimer’s Dement. 2019;15:888–98.
Acknowledgements
The authors want to thank all EMIF-AD PreclinAD participants for their efforts to join and complete this demanding study.
Funding
This work has received support from the EU/EFPIA Innovative Medicines Initiative Joint Undertaking EMIF grant agreement n°115372. This work also received in-kind sponsoring of the CANTAB device from Cambridge Cognition and the PET tracer from GE Healthcare. S.F.C. is supported by the NIHR Cambridge Biomedical Research Centre (BRC-1215-20014). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Author information
Authors and Affiliations
Contributions
PJ.V., D.I.B., and Ph.S. contributed to conception and design of the study; J.T., A.dB., S.J.vdL., L.M.R., E.K., S.F.C., M.Y., B.N.M.vB., L.E.C., D.I.B., E.J.C.dG., K.H. and B.M.T. contributed to acquisition and analysis of data; J.T., A.dB., B.M.T. and PJ.V. contributed to drafting the text and/or preparation of Figs. 1, 2, 3 and 4. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The National Research Ethics Service Committee North West—Greater Manchester South performed ethical approval of the study for Manchester. The Medical Ethics Review Committee of the VU University Medical Center performed approval of the study for Amsterdam. Each participant gave written informed consent. The research is performed according to the principles of the Helsinki Declaration of 1975 and in accordance with the Medical Research Involving Human Subjects Act and codes on ‘good use’ of clinical data and biological samples as developed by the Dutch Federation of Medical Scientific Societies.
Consent for publication
Not applicable.
Competing interests
J.T., A.dB., S.J.vdL., L.M.R., E.K., S.F.C., M.Y., B.N.M.vB., L.E.C., D.I.B., E.J.C.dG., K.H., B.M.T. and PJ.V. declare that they have no competing interests. Ph.S. has received consultancy fees (paid to the institution) from AC Immune, Brainstorm Cell, EIP, ImmunoBrain Checkpoint, Genentech, Novartis and Novo Nordisk. He is PI of studies with AC Immune, FUJI-film/Toyama, UCB, and Vivoryon. He is a part-time employee of Life Sciences Partners Amsterdam.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.


Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
{kind=link}
Cite this article
Tomassen, J., den Braber, A., van der Lee, S.J. et al. Amyloid-β and APOE genotype predict memory decline in cognitively unimpaired older individuals independently of Alzheimer’s disease polygenic risk score. BMC Neurol 22, 484 (2022). https://doi.org/10.1186/s12883-022-02925-6
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-022-02925-6