
Abstract
Background
Family physicians had to deliver care remotely during the COVID-19 pandemic. Their efforts highlighted the importance of develo** a primary care telemedicine (TM) model. TM has the potential to provide a high-quality option for primary care delivery. However, it poses unique challenges for older adults. Our aim was therefore to explore the effects of TM and the determinants of its use in primary care for older adults.
Methods
In this systematic mixed studies review, MEDLINE, PsycINFO, EMBASE, CINHAL, AgeLine, DARE, Cochrane Library, and clinical trials research registers were searched for articles in English, French or Russian. Two reviewers performed study selection, data extraction and assessment of study quality. TM’s effects were reported through the tabulation of key variables. TM use determinants were interpreted using thematic analysis based on Chang’s framework. All data were integrated using a joint display matrix.
Results
From 3,328 references identified, 20 studies were included. They used either phone (n = 8), videoconference (n = 9) or both (n = 3). Among studies reporting positive outcomes in TM experience, ‘user habit or preferences’ was the most cited barrier and ‘location and travel time’ was the most cited facilitator. Only one study reported negative outcomes in TM experience and reported ‘comfort with patient communication’ and ‘user interface, intended use or usability’ as barriers, and ‘technology skills and knowledge’ and ‘location and travel time’ as facilitators.
Among studies reporting positive outcomes in service use and usability, no barrier or facilitator was cited more than once. Only one study reported a positive outcome in health-related and behavioural outcomes.
Conclusions
TM in older adults’ primary care generally led to positive experiences, high satisfaction and generated an interest towards alternative healthcare delivery model. Future research should explore its efficacy on clinical, health-related and healthcare services use.
Key points
-
Most health systems have been able to adapt quickly to virtual consultations with their patients, but there are still opportunities for improvement for older populations.
-
Older patients want to have access to both in-person and virtual consultations when appropriate.
-
Telemedicine for older adults’ primary care generally led to positive experiences, high satisfaction towards alternative healthcare delivery model.
Similar content being viewed by others

Impact statement
We certify that this work is novel of recent novel clinical research. This mixed studies review provides insightful findings on the effects of telemedicine on the general care experience, the service use and usability and the health-related and behavioural outcomes of older adults, in addition to uncovering the determinants of its use by this population. Its conclusions can guide primary care clinicians in an optimal use of telemedicine by listing key elements to foster a clinical context favourable to telemedicine use with an older population.
Why does this paper matter?
This review was designed to explore the literature to understand telemedicine in primary care for older adults. The assessment of the impact of on the general care experience, service use, and health-related outcomes of older adults, as well as determinants of telemedicine use, will inform the qualitative descriptive study of a larger multi-phase research.
Introduction
The COVID-19 crisis has substantially changed the delivery of primary care. Indeed, with the public health measures, a lot of clinic-based care turned into virtual remote care [1]. Telemedicine (TM) became pervasive. TM refers to an alternative to in-person clinic-based care, and is defined as synchronous remote teleconsultations using phone or video [2]. Prior to the pandemic, research already suggested that TM was an effective approach to deliver medical care, including for older adults [3]. Post-pandemic reflections now suggest it could definitely constitute an asset, not only as part of an emergency response but as mainstream usual primary care by providing remote triage, routine follow-up, and remote care [4].
Yet, due to potential age-related changes in perceptual, motor, or cognitive capacities, older adults may present different needs from the general population, potentially affecting the impact of TM among this population and even their use of the approach [5]. Also, most of the available evidence on TM generally focuses on younger populations [6, 7]. As many experts debated on the extent to which COVID-19-related adaptations will be maintained post-pandemic [8], exploring the potential of TM for the primary care of older adults is essential.
Therefore, this systematic mixed studies review aimed to: 1) To assess the effects of TM on the general care experience, service use, as well as on health-related outcomes in a context of primary care practice for older people, 2) To explore the determinants of TM use in the primary care practice of older people.
Methods
This systematic mixed studies review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [9]. We included studies with a variety of designs, either quantitative, qualitative or mixed-methods [10]. Mixed studies reviews are appropriate to understand and conceptualize multi-dimensional complex phenomena [11, 12]. This review is a first phase of a multiphase study on telemedicine for older adults in primary care [13]. The review protocol has been recorded at the PROSPERO, CRD42021237686 https://www.crd.york.ac.uk/prospero.
Data sources
The key concepts of ‘telemedicine’, ‘aged’, and ‘primary health care’ were combined using Boolean logic [14], also using additional related terms such as “ “Video consult*”, “Remote consultation”, “Distance counseling”, “Virtual consultation”. A complete list of terms used for the EMBASE search strategy is available in Supplementary Text S1.
A systematic search was performed by a specialized librarian in MEDLINE, PsycINFO, EMBASE, CINAHL, AgeLine, the Database of Abstracts or Reviews of Effects (DARE), the Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), clinical trials research registers (ClinicalTrials.gov and the WHO’s International Clinical Trials Registry Platform) to identify publications in English, French or Russian, based on our team's linguistic proficiency, published before July 2021. We then conducted a snowballing manual search of the reference lists of the included studies to identify additional relevant papers. A final research update was completed in September 2021.
Study selection
We included all studies presenting primary findings on TM in a context of primary care for community-dwelling older adults or their caregiver. Adults aged over 65 years old living in the community, caregivers, or healthcare providers involved in older adults’ care were included. Telemedicine was defined as synchronous telecommunication (phone, videoconference), provided by a primary care practice involving a family physician, a nurse, or any other healthcare allied professional of the clinic. Only studies reporting relevant outcomes were included, related to experience, effects, determinants and other outcomes such as satisfaction, users’ experience, intention to use, expectations, and frequency of emergency department visits. Detailed inclusion and exclusion criteria are available in Supplementary Table S2.
Two independent reviewers (MI, MLB) selected articles through a two-step process (titles/abstracts, full-text). Any disagreements were resolved by consensus or the involvement of an additional reviewer (VK). Companion articles of included studies were examined and treated as one study.
Data collection
Two reviewers (MI, MLB) independently extracted data using a standardized data collection form. They screened all included articles for: a) study characteristics, including authors, year of publication, country of origin, and study design; b) description of the participants, including sample size, sex, age, and description of the setting of the family medicine practice (e.g., solo vs team-based, healthcare professionals), c) type of TM described and its components (e.g., phone vs video conference), d) any reported outcomes on the experience with TM (e.g., satisfaction with care), health care services use (e.g., number of clinical visits), or clinical outcomes (e.g., health status), e) barriers and facilitators to TM use.
Data synthesis
This mixed studies review used a parallel-results convergent synthesis design [15] in a three-step process (Fig. 1): (1) analysis of data from quantitative and mixed-methods studies, (2) thematic analysis of data from qualitative and mixed-methods studies, and (3) integration of both findings.

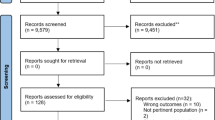
Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) flow diagram
At step 1, we reported TM effects, through findings on the general care experience, on service use and usability and on health-related and behavioural outcomes by tabulating the reported key variables.
At step 2, we coded and interpreted the different reported determinants of TM use using a qualitative thematic deductive analysis based on Chang’s logical framework [16]. Chang’s framework consists of 38 determinants in total, classified into six constructs (healthcare providers, patients, organization, technology, society, and rules/policy), distributed among three dimensions (human, system, and environment). We coded each determinant, identified from the included studies, as either a barrier, an ambivalent determinant or a facilitator.
At step 3, both findings from the previous steps were integrated using a joint display matrix [17]. We combined the findings on TM effects in rows with the findings on determinants of TM use in columns. Two independent reviewers (MI, MLB) visually analyzed patterns and iteratively explored similarities and differences in the direction of findings, in relation to the identified determinants. Any disagreements were resolved by consensus or the involvement of an additional reviewer (VK).
Quality assessment
Two reviewers (MI, MLB) independently assessed quality of each included study using the mixed methods appraisal tool (MMAT) [18]. The MMAT is a validated critical appraisal tool designed to appraise the methodological quality of qualitative, quantitative and mixed-methods studies. In accordance with MMAT standards, no overall quality score was calculated; studies were appraised as having low, moderate or high methodological quality. Any disagreements were resolved by consensus or the involvement of an additional reviewer (VK).
Results
Characteristics of included studies
The searches initially identified 3,328 references. Of these, 2,990 were excluded based on their title/abstracts and 317 based on their full-text. A total of 20 articles were included in the review (Fig. 2): 11 quantitative [19,20,21,22,23,24,25,26,27,28,29], six qualitative [30,31,32,33,34,35], and 3 mixed-method studies [36,37,38]. Their characteristics are summarized in Tables 1 and 2. Overall, the geographic locations of the studies were diverse, with six studies in the United States of America [19, 21,22,23,24, 33], two in the United Kingdom [25, 34], two in the Netherlands [20, 36], two in Sweden [31, 38], one in Spain [29], one in Scotland [37], one in Ireland [27], one in Switzerland [35], one in Poland [28], one in Portugal [26], one in China [32], and one in New Zealand [30]. Eight studies focused on TM with phones [19, 21, 23, 25, 26, 30, 34, 35], nine on TM with videoconference [20, 22, 24, 27, 32, 33, 36,37,38] and three on TM with both phone and videoconference [28, 29, 31]. Overall, studies reported on multiple determinants of TM use in all three dimensions of Chang’s framework [16]. Most cited determinants belonged to the human dimension. The environmental dimension determinants were the less cited. All details on the reported determinants are available in Table 2).

Three-step process of the mixed studies review using a parallel- results convergent synthesis design
TM effects on general care experience
Among the 18 different studies reporting on the effects of TM on the general care experience, eleven described the general experience of TM itself, using semi-structured interviews, non-validated questionnaires, focus groups, validated questionnaires or a case report method. Three reported on satisfaction with TM, using a validated questionnaire, a non-validated questionnaire or a combination of a non-validated questionnaire with interviews. Three reported on TM readiness, using longitudinal data from a national survey, a non-validated questionnaire or interviews. One reported on attitudes regarding TM, using both a validated and a non-validated questionnaire. One reported on interest towards TM, using a non-validated questionnaire. One reported on TM acceptability using semi-structured interviews.
Among studies reporting positive outcomes on the general care experience (n = 11) [19, 20, 22, 24, 25, 27, 29,30,31, 37, 38], ‘user habit or preferences’ was the most cited determinant, reported as a barrier by three studies [22, 25, 29], as a facilitator by one study [27] and as a more ambivalent factor by five studies (Supplementary Table S4) [19, 24, 30, 31, 37]. ‘User habits or preferences’ was also the most cited barrier. Many older adults expressed how they preferred face-to-face interactions and remain within familiar territory, while some mentioned positive experiences with the technology, on which they were ready to build to learn about TM. The most cited facilitator was the ‘location and travel time’, reported as a facilitator by three studies [29,30,31]. Most saw in TM an increased accessibility, particularly for rural areas, and convenient time saving from both sides.
Only one study reported negative outcomes [34], and reported ‘comfort with patient communication’ as a barrier. It reflected a worry expressed by older patients, who questioned whether primary care clinicians would really be in a position to assess their needs over the phone and ‘make accurate diagnoses in these circumstances’, particularly in the case of a new clinical encounter. In addition, the study also reported ‘User interface, intended use or usability’ as a barrier. Older patients also expressed difficulties with some aspects of TM, notably the use of pre-recorded vocal messages, as useful information was “sometimes given too quickly to be noted down”. In contrast, this study reported both the ‘technology skills and knowledge’ and the ‘location and travel time’ as facilitators. While other studies mentioned distrust, inexperience, unreadiness or lack of self-efficacy with the technology, some older adults even claiming they were ‘digital illiterate’, participants from Foster et al.’s study (2001) [34] reported that they felt confident to use the telephone for “medication queries and minor problems”.
TM effects on healthcare service use and usability
Among the nine different studies reporting on service use and usability, seven reported on usability, using an administrative database, semi-structured interviews or a validated questionnaire and two reported on the number of clinical visits, using an administrative database or a non-validated questionnaire.
Among studies reporting positive outcomes in service use and usability (n = 3) [26, 27], the ‘disease characteristics and sociodemographic characteristics’ was the most cited determinant with all three studies reporting it as an ambivalent factor (Supplementary table S4). Certain symptoms and conditions motivated the use of TM to obtain counseling and access to further care via telephone, such as pain and respiratory tract disorders [26]. Certain characteristics also influenced TM use, with women apparently being more disposed than men to use telephone consultations. No barrier or facilitator was cited more than once.
No study reported negative outcomes.
TM effects on health-related and behavioural outcomes
Among the two different studies reporting on health-related and behavioural outcomes, one reported on the ability to cope with illness using a validated tool and one on general health status using a validated questionnaire [25, 30].
Only one study reported a positive outcome in health-related and behavioural outcomes [25]. This study only cited the ‘user habit or preferences’ as a determinant, reported as a barrier (Supplementary Table S4).
No study reported negative outcomes.
Quality assessment
The quality of the included studies was overall very high (Table 3). Only six studies had one item or more with unknown risk of bias due to unavailable, insufficient or unclear information [19, 21, 22, 25, 28, 32]. Two studies had two items or more with unknown risk of bias [28, 32]. No study was at high risk on any of the methodological quality criteria.
Discussion
This review included 21 studies of various designs to explore the effects of TM and the determinants of its use in older adults’ primary care. Both phone and videoconference technologies appeared equally reported. As older adults worldwide are still not using the internet and smartphones as much as their younger counterparts [50, 51], this equal distribution between higher and lower-tech options can be surprising. All primary and original studies reporting findings on TM in a context of primary care for older adults living in the community published before 2021, were included. We defined telemedicine as a synchronous telecommunication (phone, videoconference) in a primary care setting. Accordingly, we have decided not to set a publication start date to ensure that all synchronous TM interventions have been accounted for in our research.
According to our findings, TM also appears to lead to a generally positive experience among older adults. Previous reviews on TM among broader populations and not focused on family medicine similarly reported positive findings on patient satisfaction, despite highlighting methodological difficulties in their identified studies [6]. Our review described limited yet positive effects of TM on service use and on health-related outcomes. Other reviews reporting on the clinical effects of TM among an adult population provided encouraging findings, yet only targeted populations with specific conditions, such as diabetes or hypertension [52,53,54]. Additionally, these reviews mostly looked at clinical interventions relying heavily on monitoring [52], rather than TM as an alternative to in-person visits in primary care.
Lastly, the most commonly cited barrier from our findings pertained to ‘Technology skills and knowledge’ and the most commonly cited facilitator pertained to ‘Location/travel time’. Partially echoing our findings, Kruse et al. [55] further identified the decrease in travel time as a factor of satisfaction in their review on TM within the general population.
In hindsight, TM appears to be quickly moving from an emergent and innovative approach to a more mainstream type of care. Among the 21 studies included in this review, more than half (11/21, 52%) were published in the past five years and none were published before 2000. This already suggests a rapid increase in the interest on the topic. Undoubtedly, with the various applications of TM recently created in a state of emergency, the COVID-19 crisis will now spur the growth in this field towards an even more drastic expansion. Researchers worldwide are already starting to ask how much of the COVID era TM will remain and be definitely integrated in usual care [56].
Yet, there are still limited data targeting the specific population of older adults and the specific practice of primary care. From this review, most evidence were uncontrolled, non-randomized studies, with only two RCTs published on the topic, thus limiting the strength of recommendations [57].
Additionally, as this review illustrated, most reported data were concentrated around the experiences of primary care TM for older adults. Very few authors reported findings on the various outcomes of service use and on health-related outcomes. Furthermore, most reported determinants focused on the experiences of patients and healthcare providers, only briefly touching on organizations and technologies and mostly leaving aside the society and policy categories. Thus, based on this limited diversity in the reported variables, the relative diversity of the authors, the sheer number of publications and their recent date, the limited diversity or methods used and their types, and the high quality of the produced studies, the research field of primary care TM for older adults appears to be at an early to moderate maturity stage [58]. As this moderately new field begins its expansion, researchers will be expected to plan studies using additional study designs, such as RCTs, and to investigate further additional variables, notably service use and health-related outcomes. This addition of new data supporting the efficacy of TM in the primary care of older adults and validating the determinants of its use from various stakeholders’ perspectives, will then allow for more solid recommendations and a successful implementation in the near future [59].
The ‘primary care clinicians’ and ‘patients/caregivers’ categories of the human dimension and the ‘technology’ category of the system dimension all had determinants cited five times or more. From these, ‘comfort with patient communication’ (n = 5), ‘technology skills and knowledge’ (n = 7), ‘user habit/preferences’ (n = 6), ‘technology equipment’ (n = 6) and ‘reliability of technology’ (n = 5) were the most common barriers and ‘location/travel time’ was the most common facilitator.
The relationship older adults hold with the technology thus appears central to most barriers to TM use. Either through their possession of a specific device, their confidence in its ability to properly work, their own literacy and self-efficacy to effectively use it, or their preferences, several pitfalls await the implementation of TM among this population. However, the generational divide in technology use tend to narrow each year and more older adults are using internet now than ever [60]. Many registered an even more rapid increase in internet use with the coronavirus pandemic [61]. Nevertheless, the old age is not a homogeneous group and some older adults are still reluctant to adopt recent technology. Among them, researchers have identified ‘non-users’, ‘reluctant users’, and ‘apprehensive users’, each with different profiles but similar ages [62]. The implementation of primary care TM in older adults might then benefit from overcoming the barriers identified in this review, while targeting the specific groups in which they are most likely to occur.
The time savings associated with TM appears particularly appealing across studies. As caring for oneself and health-related activities can take up to 23 h per month for many older adults [63], the opportunity to limit transportation time may be highly meaningful for some.
Strengths and limitations
This review is the first to provide specific conclusions on TM for older adults’ primary care. Other existing reviews on TM either targeted younger populations [6, 7], populations with specific conditions [52,53,54], or included specific interventions outside the scope of practice of primary care [64]. The methodology of this review relied on a rigorous and comprehensive systematic approach supported by a specialized librarian, a detailed framework [16] to structure data collection, and a validated tool for critical appraisal [18]. Its mixed method design also enlightened the significance of both qualitative and quantitative data to comprehend fully the complexities that underpin the use of TM with older adults. Yet, this review presents some limitations. Notably, the heterogeneity of outcome reported across studies prevented us to run any meta-analysis. Some studies only mentioned old age without specifying the exact age of their participants. Furthermore, not all studies reported medical conditions and comorbidities of their participants, preventing subgroup analysis. Finally, the completion of this systematic review during the COVID-19 pandemic may have impacted research results. Care provided in clinics was forced to tailor their practice to include TM as an option for remote and safe consultations. As a result, we believe further research on TM has been conducted, which may have increased and exaggerated the number of results.
Impact on clinical practice
This review showed that TM might represent a suitable option for older adults, conditional to their clinical context, considering both healthcare professionals and patients’ specificities. In light of our findings, clinicians could thus direct their efforts to the following elements for an optimal use of TM by healthcare professionals:
-
Ensure that clinicians or clinical teams feel able to maintain a clear communication with patients,
-
Support the familiarization of clinicians with available communication technologies, to enhance their confidence in collecting comprehensive patients' information through these tools and facilitate interdisciplinary collaboration inside and outside clinical teams,
-
Encourage leadership-driven TM initiatives and acknowledge or reward the contributions of peers or other groups and organisations in supporting these initiatives.
Considering patients’ specificities, clinicians could also assess how TM could align with their patients’ preferences by:
-
Introducing tools adapted to their technology skills, supporting patients in their TM platform navigation as needed and providing assistance to foster self-efficacy,
-
Promoting the advantages and benefits of selected TM, notably on travel and travel time, to further encourage its acceptability,
-
Advocating for a greater accessibility of technological tools that could improve patients' health, to ensure the access of their patients to appropriate equipment.
Conclusion
This review indicates that TM might be a promising option for older adults receiving primary healthcare. However, to foster TM use among this population, decision-makers should consider the clinical context and both the patient’s and the healthcare professional’s profiles. While more evidence is still needed on the efficacy of TM on various indicators for older adults seen in primary care, the time appears particularly ripe to provide such remote options, with a careful consideration of the determinants of its use.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
Ohannessian R, Duong TA, Odone A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: a call to action. JMIR Public Health Surveill. 2020;6(2): e18810.
World Health Organization. Telemedicine: opportunities and developments in member states. Report on the second global survey on eHealth. World Health Organization; 2010.
Merrell RC. Geriatric telemedicine: background and evidence for telemedicine as a way to address the challenges of geriatrics. Healthc Inf Res. 2015;21(4):223–9.
Smith AC, Thomas E, Snoswell CL, et al. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020;26(5):309–13.
Stronge AJ, Rogers WA, Fisk AD. Human factors considerations in implementing telemedicine systems to accommodate older adults. J Telemed Telecare. 2007;13(1):1–3.
Mair F, Whitten P. Systematic review of studies of patient satisfaction with telemedicine. BMJ. 2000;320(7248):1517.
Shah AC, Badawy SM. Telemedicine in pediatrics: systematic review of randomized controlled trials. JMIR Pediatr Parent. 2021;4(1): e22696.
Weiner S. What happens to telemedicine after COVID-19? Association of American Medical Colleges. https://www.aamc.org/news-insights/what-happens-telemedicine-after-covid-19. Published 2021. Accessed 12-2021.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–34.
Popay J, Roberts H. Methodological issues in the synthesis of diverse sources of evidence. In: Moving beyond effectiveness : methodological issues in the synthesis of diverse sources of evidence. London: National Institute for Health and Clinical Excellence; 2006. pp. 1-10.
Creswell JW, Vicki L, Plano C. Designing and conducting mixed methods research. Sage publications; 2017.
Pluye P, Gagnon M-P, Griffiths F, Johnson-Lafleur J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int J Nurs Stud. 2009;46(4):529–46.
Khanassov V, Ilali M, Vedel I. Protocol of a multiphase study on telemedicine for older adults in primary care. BMJ Open. 2022;12(4): e057061.
Scells H, Zuccon G, Koopman B. Automatic Boolean query refinement for systematic review literature search. 2019.
Hong QN, Pluye P, Bujold M, Wassef M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev. 2017;6(1):1–14.
Chang H. Evaluation framework for telemedicine using the logical framework approach and a fishbone diagram. Healthc Inf Res. 2015;21(4):230–8.
Guetterman TC, Fetters MD, Creswell JW. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann Fam Med. 2015;13(6):554–61.
Hong QN, Gonzalez-Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J Eval Clin Pract. 2018;24(3):459–67.
Welch H, Johnson D, Edson R. Telephone care as an adjunct to routine medical follow-up. A negative randomized trial. Effect Clin Pract. 2000;3(3):123–30.
van Houwelingen CT, Barakat A, Best R, Boot WR, Charness N, Kort HS. Dutch nurses’ willingness to use home telehealth: Implications for practice and education. J Gerontol Nurs. 2015;41(4):47–56.
Townsend CH, Maxwell W, Sears LT. Nurse practitioner patient centered telephone calls in a Va primary care geriatric clinic. J Am Acad Nurse Pract. 2001;13(6):269–75.
Samples LS, Martinez J, Beru YN, Rochester MR, Geyer JR. Provider perceptions of telemedicine video visits to home in a veteran population. Telemed e-Health. 2021;27(4):422–6.
Lam K, Lu AD, Shi Y, Covinsky KE. Assessing telemedicine unreadiness among older adults in the United States during the COVID-19 pandemic. JAMA Intern Med. 2020;180(10):1389–91.
Khoong EC, Butler BA, Mesina O, et al. Patient interest in and barriers to telemedicine video visits in a multilingual urban safety-net system. J Am Med Inform Assoc. 2021;28(2):349–53.
Jiwa M, Freeman J, Coleman M, Joesbury H. Do older patients feel able to cope with illness following telephone consultations? A multi-practice survey in the UK. Curr Med Res Opin. 2005;21(3):339–43.
Jácome M, Rego N, Veiga P. Potential of a nurse telephone triage line to direct elderly to appropriate health care settings. J Nurs Manag. 2019;27(6):1275–84.
Chae YM, Lee JH, Ho SH, Kim HJ, Jun KH, Won JU. Patient satisfaction with telemedicine in home health services for the elderly. Int J Med Inf. 2001;61(2–3):167–73.
Bujnowska-Fedak MM, Pirogowicz I. Support for e-health services among elderly primary care patients. Telemed E-health. 2014;20(8):696–704.
Benaque A, Gurruchaga MJ, Abdelnour C, et al. Dementia care in times of COVID-19: experience at Fundació ACE in Barcelona Spain. J Alzheimer’s Dis. 2020;76(1):33–40.
Waterworth S, Raphael D, Parsons J, Arroll B, Gott M. Older people’s experiences of nurse–patient telephone communication in the primary healthcare setting. J Adv Nurs. 2018;74(2):373–82.
Nymberg VM, Bolmsjö BB, Wolff M, Calling S, Gerward S, Sandberg M. ‘Having to learn this so late in our lives…’Swedish elderly patients’ beliefs, experiences, attitudes and expectations of e-health in primary health care. Scand J Prim Health Care. 2019;37(1):41–52.
Kung K, Wong HF, Chen JY. "An exploratory qualitative study on patients' views of medical e-consultation in a public primary care setting." Hong Kong Practitioner. 2016;38(4):120–7.
Franzosa E, et al. "“There is something very personal about seeing someone’s face”: Provider perceptions of video visits in home-based primary care during COVID-19." J Appl Gerontol. 2021;40(11):1417–24.
Foster J, Dale J, Jessopp L. A qualitative study of older people’s views of out-of-hours services. Br J Gen Pract. 2001;51(470):719–23.
Blozik E, Wildeisen IE, Fueglistaler P, von Overbeck J. Telemedicine can help to ensure that patients receive timely medical care. J Telemed Telecare. 2012;18(2):119–21.
van Houwelingen CT, Ettema RG, Antonietti MG, Kort HS. Understanding older people’s readiness for receiving telehealth: mixed-method study. J Med Internet Res. 2018;20(4): e8407.
Macduff C, West B, Harvey S. Telemedicine in rural care. Part 2: Assessing the wider issues. Nurs Standard (through 2013). 2001;15(33):33.
Gabrielsson-Järhult F, Kjellström S, Josefsson KA. Telemedicine consultations with physicians in Swedish primary care: a mixed methods study of users’ experiences and care patterns. Scand J Prim Health Care. 2021:1–10.
Ware JE, Snyder MK, Wright WR, Davies AR. Defining and measuring patient satisfaction with medical care. Eval Program Plann. 1983;6(3–4):247–63.
Ware JE, Kosinski M, Keller SD. Physical and mental health summary scales: a user’s manual. Boston: The Health Institute; 1994.
Wasson J, Gaudette C, Whaley F, Sauvigne A, Baribeau P, Welch HG. Telephone care as a substitute for routine clinic follow-up. JAMA. 1992;267(13):1788–93.
Vidal-Alaball J, Flores Mateo G, Garcia Domingo JL, et al. Validation of a short questionnaire to assess healthcare professionals’ perceptions of asynchronous telemedicine services: the Catalan version of the health optimum telemedicine acceptance questionnaire. Int J Environ Res Public Health. 2020;17(7):2202.
Howie JG, Heaney DJ, Maxwell M, Walker JJ. A comparison of a Patient Enablement Instrument (PEI) against two established satisfaction scales as an outcome measure of primary care consultations. Fam Pract. 1998;15(2):165–71.
Montaquila J, Freedman V, Spillman B, Kasper J. National Health and Aging Trends Study (NHATS) development of round 1 survey weights. Baltimore: Johns Hopkins University School ofPublic Health; 2012 [cited 2017 May 5].(NHATS Technical Paper No. 2)..
Engelen U, De Peuter S, Victoir A, Van Diest I, Van den Bergh O. Verdere validering van de Positive and Negative Affect Schedule (PANAS) en vergelijking van twee Nederlandstalige versies. Gedrag en gezondheid. 2006;34(2):61–70.
Czaja SJ CN, Dijkstra K, Fisk AD, Rogers WA, Sharit J. Computer and technology experience questionnaire. Create Center Web site. http://create-center.gatech.edu/resources.php. Published 2006. Accessed 08-2021.
Predicting Medical Staff intention to use an online reporting system with modified unified theory of acceptance and use of technology. Telemed e-Health. 2012;18(1):67–73.
Using a modified technology acceptance model to evaluate healthcare professionals' adoption of a new telemonitoring system. Telemed e-Health. 2012;18(1):54–59.
Czaja SJ CN, Dijkstra K, Fisk AD, Rogers WA, Sharit J. Demographic and background questionnaire. Create Center Web site. http://create-center.gatech.edu/resources.php. Published 2006. Accessed 08-2021.
Hunsaker A, Hargittai E. A review of Internet use among older adults. New Media Soc. 2018;20(10):3937–54.
Nelson KB. Tech Trends of the 50+. Washington, DC: AARP Research; 2020.
Robson N, Hosseinzadeh H. Impact of telehealth care among adults living with type 2 diabetes in primary care: a systematic review and meta-analysis of randomised controlled trials. Int J Environ Res Public Health. 2021;18(22).
Zhang W, Cheng B, Zhu W, Huang X, Shen C. Effect of telemedicine on quality of care in patients with coexisting hypertension and diabetes: a systematic review and meta-analysis. Telemed e-Health. 2021;27(6):603–14.
Timpel P, Oswald S, Schwarz PEH, Harst L. Map** the evidence on the effectiveness of telemedicine interventions in diabetes, dyslipidemia, and hypertension: an umbrella review of systematic reviews and meta-analyses. J Med Internet Res. 2020;22(3): e16791.
Kruse C, Fohn J, Wilson N, Patlan EN, Zipp S, Mileski M. Utilization barriers and medical outcomes commensurate with the use of telehealth among older adults: systematic review. JMIR Med Inform. 2020;8(8): e20359.
Chen K, Davoodi NM, Strauss DH, et al. Strategies to ensure continuity of care using telemedicine with older adults during COVID-19: a qualitative study of physicians in primary care and geriatrics. J Appl Gerontol. 2022;41(11):2282–95.
Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64(4):380–2.
Keathley-Herring H, Van Aken E, Gonzalez-Aleu F, Deschamps F, Letens G, Orlandini PC. Assessing the maturity of a research area: bibliometric review and proposed framework. Scientometrics. 2016;109(2):927–51.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):1–15.
Leukel J, Schehl B, Sugumaran V. Digital inequality among older adults: explaining differences in the breadth of Internet use. Inf, Commun Soc. 2021:1–16.
Nimrod G. Not good days for technophobes: older internet users during the COVID-19 pandemic. Educ Gerontol. 2021;47(4):160–71.
Quan-Haase A, Williams C, Kicevski M, Elueze I, Wellman B. Dividing the grey divide: Deconstructing myths about older adults’ online activities, skills, and attitudes. Am Behav Sci. 2018;62(9):1207–28.
Jowsey T, McRae I, Gillespie J, Banfield M, Yen L. Time to care? Health of informal older carers and time spent on health related activities: an Australian survey. BMC Public Health. 2013;13(1):374.
Batsis JA, DiMilia PR, Seo LM, et al. Effectiveness of ambulatory telemedicine care in older adults: a systematic review. J Am Geriatr Soc. 2019;67(8):1737–49.
Acknowledgements
The authors wish to thank Dina Gaid and Rosa Sourial for their contribution during the screening process and Genevieve Gore for assisting the database searches.
Funding
MI was supported by the Canadian Institutes of Health Research under the award Canada Graduate Scholarship-Master’s (CGS M). CGS M plays a crucial role in providing valuable recognition and essential financial aid to Canadian students who are actively pursuing a Master's degree in a health-related field.
VK received funding from Fonds de Recherche du Québec (FRQS) – Impulsion grant, 2022-IMPV-308987, and MIGS grants from the College of Family Physicians of Canada (CFPC). The Impulsion Program plays a vital role in fostering post-pandemic economic recovery by creating favorable conditions and an enabling environment in Québec. The funding for Member Interest Groups (MIGs) serves two roles, it encourages projects enhancing family medicine areas while supporting CFPC's mission and MIGs' strategic plan.
Author information
Authors and Affiliations
Contributions
Study conception and design: MI, VK. Data collection: MI, ML. Analysis and interpretation of results: MI, ML, VK, IV. Draft manuscript preparation: MI, MB. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to declare.
All co-authors have seen and agree with the contents of the manuscript and there is no financial interest to report. We certify that the submission is original work and is not under review at any other publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ilali, M., Le Berre, M., Vedel, I. et al. Telemedicine in the primary care of older adults: a systematic mixed studies review. BMC Prim. Care 24, 152 (2023). https://doi.org/10.1186/s12875-023-02085-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-023-02085-7