
Abstract
Background
With the ageing population worldwide, falls are becoming a severe and growing health problem. Interprofessional multifactorial fall prevention interventions (FPIs) have effectively prevented falls in community-dwelling older adults. However, the implementation of FPIs often fails due to a lack of interprofessional collaboration. Therefore, gaining insight into the influencing factors of interprofessional collaboration in multifactorial FPI’s for older adults living in the community is essential. Consequently, our aim was to provide an overview of factors influencing interprofessional collaboration in multifactorial FPIs for community-dwelling older adults.
Methods
This qualitative systematic literature research was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Pubmed, CINAHL, and Embase electronic databases have been systematically searched for eligible articles, with a qualitative design. The quality was appraised using the Checklist for Qualitative Research by the Joann Briggs Institute. The findings were inductively synthesized using a meta-aggregative approach. Confidence in the synthesized findings was established using the ConQual methodology.
Results
Five articles were included. Analysis of the included studies resulted in 31 influencing factors for interprofessional collaboration, which were labelled as findings. These findings were summarized in ten categories and combined into five synthesized findings. Results showed that communication, role clarity, information sharing, organization, and interprofessional aim influence interprofessional collaboration in multifactorial FPIs.
Conclusions
This review provides a comprehensive summary of findings on interprofessional collaboration, specifically in the context of multifactorial FPIs. Knowledge in this area is considerably relevant given the multifactorial nature of falls, which demands an integrated, multidomain approach, including both health and social care. The results can be utilized as a fundament for develo** effective implementation strategies aiming to improve interprofessional collaboration between health and social care professionals working in multifactorial FPIs in the community.
Similar content being viewed by others


Background
According to the World Health Organization, falls are the second leading cause of unintentional injury deaths worldwide, with persons over 60 years old having the highest number of falls [1]. In 29 per cent of community-dwelling older adults, falls occur at least once a year, with rising numbers with increasing age [2, 3]. Falls frequently result in hip or other severe fractures [4]. Moreover, falls often have a negative impact on activities in daily living, independence, fear, and overall health outcomes [5,6,7]. Given the increasing older population worldwide and the growing prevalence of multimorbidity, and frailty [8], fall rates and medical expenditures are likely to increase [9, 10].
The causus of falls among older adults are multifactorial, and several risk factors have been identified [11]. These risk factors contain a combination of intrinsic factors (e.g. impaired balance, strength and gait) and extrinsic risk factors (e.g. home hazards and poor footwear) [12,13,14,15]. Given the multifactorial nature of falls, multifactorial fall prevention interventions (FPIs) appear to be the most appropriate in reducing falls [16,17,18,19,20]. Multifactorial FPIs target present and modifiable risk factors for falling and consist of two or more intervention components across two or more domains, such as environmental modification, medication review, and they should at least include physical exercise therapy [21, 22]. Since a single discipline will never be able to identify and manage all multifactorial risk factors for falls fully, interprofessional collaboration is essential [19, 23, 24]. Interprofessional collaboration is defined as “collaborative practice which happens when multiple health workers from different professional backgrounds work together with patients, families, caregivers and communities to deliver the highest quality of care” [25]. It has been identified that good collaboration improves collaborative care, action continuity, relationship improvement, saves time, and promotes lifelong learning [26]. To achieve interprofessional collaboration care must be organized and coordinated across different settings and among various providers to address the present risk factors. However, due to the lack of interprofessional collaboration, applying multifactorial FPIs in current practice appears challenging [27].
The influencing factors of interprofessional collaboration in primary health care have been analyzed in several literature reviews [26, 28,29,30]. These include improved team communication, professional roles and duties clarity, a shared vision, effective teamwork, and action plan coordination [30, 31]. Despite the critical necessity for interprofessional collaboration in multifactorial FPIs, influencing factors have not yet been assessed within this area [32]. To develop strategies that enhance interprofessional collaboration in FPIs, it is essential to comprehend the factors that influence interprofessional collaboration. Therefore, this study aimed to provide an overview of influencing factors of interprofessional collaboration in multifactorial FPIs for community-dwelling older adults living.
Methods
Design
A qualitative systematic literature research was conducted using a meta-aggregation approach to identify influencing factors of interprofessional collaboration in FPIs for community-dwelling older adults. The meta-aggregative approach aims to provide generalizable statements as recommendations to advise practitioners and policymakers [33]. The review was undertaken according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [34]. This review is part of the Dutch implementation research project FRIEND (Fall pRevention ImplEmentatioN stuDy).The goal of the FRIEND project is to identify successful strategies for the effective, local, and integral implementation of fall prevention in the community.
Search method
A systematic literature search in the electronic databases Pubmed, CINAHL, and Embase was conducted in March 2022. The databases were searched for articles that included terms related to the main concepts, combined with Boolean operators: ‘fall prevention’, ‘interprofessional collaboration’, ‘facilitators and barriers’ and ‘community-dwelling older adults’. The search syntax was adapted to each database (Appendix A).
Inclusion criteria
Articles were eligible for this review if they described influencing factors of interprofessional collaboration in multifactorial FPIs for community-dwelling older adults. Articles were included if: 1) the FPI consisted of a multifactorial approach, including a physical exercise program (mobility, muscle strength and/or balance); 2) at least two different professions/disciplines in the community were involved in the FPI; 3) the FPIs were provided to community-dwelling older adults aged 65 years and older; 4) influencing factors that affect interprofessional collaboration were described; 5) the design of the articles was qualitative (e.g. qualitative study, review, meta-analysis, meta-ethnography, case study); 6) the article was written in Dutch or English and 7) the article was available in full text. Articles were excluded if they described interprofessional collaboration within the setting of a hospital or nursing home.
Study selection
All search results were uploaded to Mendeley Reference Manager for deduplication. After deduplication, two reviewers (JSCM, and one independent researcher) independently screened the titles and abstracts on eligibility after uploading the unique articles to a web application, Rayyan [35]. This was followed by an independent full-text examination of potentially eligible articles. When conflicts occurred, a third researcher (RZ) was approached to reach a consensus.
Data extraction
The data of all included articles were extracted by one researcher (JSCM) into a standardized extraction sheet by manually documenting the requested components. This included: authors, publication year, country, the study aims, the profession of the study participants, setting, study design, data collection method, data analysis method, and identified influencing factors of interprofessional collaboration. By reviewing random extraction sheet components, one unaffiliated researcher verified the extraction.
Methodological quality
A quality appraisal was conducted to assess the methodological quality of the included articles. Two researchers (JSCM, and one independent researcher) independently assessed the included articles using the Checklist for Qualitative Research by the Joann Briggs Institute (JBI) [36]. This checklist consists of ten questions appraising several quality aspects of a qualitative study (Table 2), such as: “Is there congruity between the stated philosophical perspective and the research methodology?” and “Are participants, and their voices, adequately represented?”. Disagreements between researchers were discussed until a consensus was reached.
Synthesis
The synthesis aimed to summarize all identified influencing factors of interprofessional collaboration in multifactorial FPIs in the community. The influencing factors were inductively synthesized in three steps in accordance with the JBI Manual for Evidence Synthesis using a meta-aggregative approach [37].
First, all influencing factors were extracted from the studies and labelled as findings. Second, for the sufficiently similar findings, categories were developed. Third, synthesized findings based on two or more compiled categories were developed. One researcher (JSCM) performed the analysis and discussed it with a supervising researcher (RZ). Interview quotes were obtained from the included articles and were reported according to related categories and synthesized findings.
Then, following the ConQual method, all relevant findings from the articles were rated (JSCM) to express the degree to which the researchers’ interpretation was credible [38]. The level of credibility of each finding is rated using the following ranking scale:
-
• Unequivocal (findings accompanied by an illustration beyond reasonable doubt and therefore not open to challenge).
-
• Equivocal (findings accompanied by an illustration lacking clear association with it and therefore open to challenge).
-
• Unsupported (the data do not support findings).
Confidence in the synthesized findings
In order to rate the confidence of the synthesized findings in the current review study, the ConQual methodology was used [37]. Within this methodology, the dependability of the included studies’ individual findings and the credibility of the synthesized findings in the current review study were ranked and combined. This resulted in a rating of confidence in the synthesized findings, into confidence levels of High, Moderate, Low, and Very low, according to the principles of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group. The following five questions from the JBI Checklist for Qualitative Research were used to rank the dependability of the findings in each individual study:
-
1. Is there congruity between the research methodology and the research question or objectives?
-
2. Is there congruity between the research methodology and the methods used to collect data?
-
3. Is there congruity between the research methodology and the representation and analysis of data?
-
4. Is there a statement locating the researcher culturally or theoretically?
-
5. Is the researcher’s influence on the research, and vice-versa, addressed?
All individual findings across the included studies started at the highest level. If four to five of the answers to these questions were ‘Yes’ for an individual finding, the level of dependability of that finding remained at the highest level. If two to three responses were ‘Yes’, the dependability level of the individual finding was downgraded by one level. In all other cases, the individual finding was downgraded by two levels, resultingin a level of downgrading the dependability.
Next, the credibility of the synthesized findings in the current study was ranked. Downgrading the credibility was based on the aggregate level of dependability from across the individual findings. Downgrading for credibility occurred when not all findings within a synthesized finding were considered unequivocal. The synthesised finding was downgraded one level for a mix of unequivocal/equivocal findings.For equivocal findings, the synthesised finding was downgraded two levels. For equivocal/unsupported findings, it was downgraded three levels, and for unsupported findings only, it was downgraded four levels. This resulted in a level of downgrading the credibility.
A combination of the level of downgrading the dependability and credibility led to a ConQual score (High, Moderate, Low, Very Low).
Results
Study selection
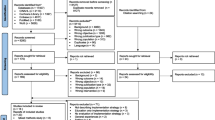
A total of 1.059 articles were found in a comprehensive literature search. After removing duplicates, 834 articles were assessed for relevance by title and abstract. Reasons for exclusion were, among others, that the article focused exclusively on risk assessment/screening instead of FPI, or the setting did not comply with the in- and exclusion criteria (e.g. hospital setting). This resulted in 26 potentially eligible articles. These eligible articles were sought for retrieval, of which one report was not retrieved [39]. After full-text screening, 20 articles were excluded. Six articles did not meet the inclusion criteria based on the study design [24, 40,41,42,43,44]. Four articles did not contain the collaboration aspect [45,46,47,48]. Four articles were not focused on community-dwelling older adults [49,50,51,52]. Three articles did not contain an exercise program [53,54,55]. Three articles did not include a multifactorial FPI [56,57,58]. This resulted in a total of five included articles [23, 59,60,61,62]. Figure 1 depicts the flow chart for the article selection process.

Flowchart of included articles
Study characteristics and influencing factors of interprofessional collaboration
Table 1 lists the included articles' characteristics and identified influencing factors of interprofessional collaboration. A qualitative design was used in four of the five articles [23, 59, 61, 62]. The other article described a mixed-method design containing a qualitative aspect [60]. Semi-structured or in-depth interviews were performed in four of the articles [59,60,61,62], while the other article conducted focus groups as part of the data collection [23]. Professionals from multiple health-related disciplines were included in all included articles [23, 59,60,61,62]. Physical therapists were included in all articles [23, 59,60,61,62], and the other participating professions were nurses, occupational therapists, dieticians, case managers, general practitioners, podiatrists, exercise physiologists and rehabilitation assistants. The sample size in the articles ranged from eight to fifteen participants.
Methodological quality
A detailed assessment and understanding of each study’s quality was provided (Table 2). Four studies [23, 59,60,61] were scored positively on all items, except for item 6 and item 7. Only one study was scored positively on these two items; Killingback et al. (2021) authors stated that the researchers were experienced physical therapists who held views and assumptions about falls rehabilitation which may have influenced the research process [62]. The study by Middlebrook et al. (2012) was the only study to be scored negatively on the item on the adequate representation of voices of the participants due to a lack of provided illustrations from the data [59].
Synthesized findings
Analysis of the included studies resulted in 31 findings covering the identified influencing factors for interprofessional collaboration, which were summarized in ten categories (Table 3). The categories were further synthesized into five synthesized findings (Table 4). The rating of the credibility of the findings is described in Table 3. The five synthesized findings were: communication, role clarity, information sharing, organization and interprofessional aim.
-
Synthesized finding 1: Communication
This theme is composed of six findings and two categories (communication barriers; Facilitators to communication). It relates to the way communication influences interprofessional collaboration. When communication was limited, it was found to be a barrier to collaboration.
“It was really difficult for us to keep up with talking about each and every one of them [clients] every month.” [23].
Specific ways of interpersonal communication, such as face-to-face, through e-mails or telephone calls, were perceived facilitators. Also, when knowledge and expertise were shared through discussions, it was recognized as facilitating interprofessional collaboration.
“If I’ve been seeing somebody for a couple of weeks… I’m struggling with how to get the patient to progress…then I’ll bring that patient to the meeting (…) there’s a wealth of knowledge and expertise.” [62].
-
Synthesized finding 2: Role clarity
This theme was created from seven findings and two categories (Understanding roles; Overlap** skills), identifying how role clarity influences interprofessional collaboration. Understanding each others’ role well within a team, was recognized to be a facilitator.
“What I am enjoying about this group is that I am learning about all the different disciplines (…) And then physio, OT, and nutrition when they collaborate together. I learn more about what they actually do, especially with their different testings.” [23].
The fact that areas of skill in this profession overlap may have prompted reservations about interprofessional collaboration.
“Consulting in general is very important to us HCNs. We always perform a medical diagnostic screening and look also for these things. (…) … and consulting (regarding facility). (We say): “You have this carpet”, then we solve this(problem) or search for solutions.” [60].
-
Synthesized finding 3: Information sharing
This theme was created based on eight findings and two categories (Barriers to information sharing; Facilitators to information sharing). It corresponds to how professionals share information within the team and how that relates to collaboration, and it can act both as a barrier and a facilitator. Barriers were excessive paperwork or meetings, or when the shared reports were unclear.
“It was put about that GPs are informed, but however, our GPs did not really have a clue.” [60].
However, whenever the way sharing and gathering data were satisfactory, this was perceived as a facilitator to interprofessional collaboration.
“With this particular gentleman, he does not want all these questions. I mean for all four of us to be asking him questions, so we talked last week maybe just having one or two of us to ask or maybe just one of us having to ask those questions.” [23].
-
Synthesized finding 4: Organization
Five findings and two categories (Work environment; Reimbursement) formed the basis for this theme. It relates to the way an organization can influence interprofessional collaboration. The work environment plays a part in interprofessional collaboration. This was a perceived facilitator when participants felt free to address issues, developed personal relationships, and received organizational support.
“Our professional leaders are at least always sort of checking in with us to make sure everything is going okay and we have any issues that need to be taken to the working committee. Very supportive.” [23].
Whenever the way of reimbursement was unclear, this could play a part between professionals, and hinder collaboration.
“I still haven’t quite got my head around how it all works, the intricacies of all these new systems they have in place.” [61].
-
Synthesized finding 5: Interprofessional aim
This theme was composed of five findings and two categories (Working with a clear aim; Value of teamwork) and relates to having a common interprofessional aim of the professionals participating in the multifactorial FPIs and how this influences the collaboration. Participants described that working with a clear aim has an impact on the collaboration.
Also, the way professionals valued the interprofessional collaboration seemed to have an impact. When professionals appreciated the team members’ addition, this was found to have a positive impact on collaboration.
“…it’s mostly physios who send people through because they know that these people need to be motivated in another way and just giving them exercises is not enough.” [61].
Confidence levels of synthesized findings
Table 5 shows the results of the confidence levels of the synthesized findings. The synthesized finding “Communication” had the highest confidence level, which was determined as “Low”. The confidence level of the other synthesized findings appeared to be “Extremely Low”. The main reasons for the extremely low confidence levels were the credibility of the findings.
Discussion
This review aimed to provide an overview of the influencing factors of interprofessional collaboration in multifactorial FPIs. This literature review resulted in 31 findings, ten categories, and five synthesized findings: communication, role clarity, information sharing, organization and interprofessional aim.
To our knowledge, this review is the first to provide a comprehensive summary of findings on this topic specifically in the context of multifactorial FPIs. Knowledge in this area is considerably relevant given the multifactorial nature of falls which demands an integrated, multidomain approach including both health and social care [63]. This integrated approach to health issues in general is essential since a growing number of older adults are living with complex and comprehensive healthcare needs [25, 32, 64, 65]. In order to offer high-quality care within this integrated approach to health care, effective interprofessional collaboration is essential [66]. However, numerous health systems worldwide need to be more cohesive and able to manage unmet health needs [25]. For that reason, interprofessional collaboration has been the main research topic of many studies in the field of health and social care. Research identifying challenges of and facilitators to interprofessional collaboration within various scopes of integrated care (e.g. chronic care, primary care, social care, community care, inpatient care) have been continued to accumulate [64, 65, 67,68,69].
Given the relatively similar focus within integrated care compared to multifactorial falls-related care, corresponding results on interprofessional collaboration have been found between the current review and other studies. This emphasizes that some aspects of interprofessional collaboration are essential to consider within any health and social care setting. For example, results in the current review show that effective communication between professionals involved in multifactorial FPIs is an essential factor in enhancing interprofessional collaboration. Also, defining roles and responsibilities (i.e. role clarity) within an interprofessional team is important. The need for effective communication and role clarity has been supported by a broad base of literature examining influencing factors for interprofessional collaboration in different healthcare settings [32, 65, 70, 71]. A recent review indicated that a ‘lack of clear role boundaries and responsibilities’ and ‘poor communication’ were amongst the most frequently identified barriers across different types of collaborations in primary care [32]. Additionally, effective communication have been shown to be a crucial competency for well-functioning interprofessional collaboration, since it increases awareness of each other’s skills and roles [72]. Effective communication encompasses a wide range of goals, strategies and purposes, such as good formal and information communication, skilful negotiation to overcome differences in viewpoints and the ability to adjust the language to the target audience [73]. Concerning role clarity, explicitly defining the function of each member in the interprofessional collaboration and his/her contribution to the collaboration may lead to a more smooth functioning between professionals [74].
Furthermore, regarding information sharing, professionals in the included articles expressed the need to share and receiving clear client reports in interprofessional collaboration. This has been highlighted in previous research as well; failing to pass along required information to be enabled to provide optimal care reduced collaboration, since it leads to individual team members to collect information from other sources themselves [75, 76]. Transferring information between team members could be provided during regular team meetings, which enables professionals to discuss issues that arise [75, 76]. However, when the information-sharing process is excessive, e.g. too many meetings are scheduled, this could become a barrier [32]. This particular finding was also identified in the included articles in this review, where professionals mentioned that excessive paperwork and meetings were perceived barriers to interprofessional collaboration.
Additionally, in the current review, professionals described the necessity of having a clear interprofessional aim, including shared vision, common team goals, and valuation of each members’ contribution. This may enable teams to set clear directions, which may lead to teams being action-oriented. Also, the process of setting clear goals could contribute to enhancing role clarity, as team members need to indicate what their specific part is in achieving the goals [75]. Making the time to develop a clear interprofessional aim and facilitating interprofessional collaboration in general requires time, support, effective personal relationships and an open atmosphere. Therefore, reimbursements and sufficient funding are essential [32]. However, with organizations having different financial structures, policies and funding, it is often difficult to initiate collaborative efforts when other organizations have few resources to invest in the relationship [77].
There are some limitations to this review. First, we only included five articles, which may have consequences for generalizing findings to different settings. However, the scarce evidence in this area underlines the importance of conducting this review. Second, as with all reviews, we risk missing relevant research due to interchangeable terminology, such as interdisciplinary collaboration, interprofessional collaborative practices, multi-professional cooperation and interaction within health care teams [78]. However, we attempted to identify all relevant studies by using various terms related to the main concepts of ‘interprofessional teamwork’, ‘influencing factors’, ‘fall prevention’, and ‘older individuals’. Consensus on terminology usage may result in definitions that can be used in education, research, and practice and could improve communication between sectors, settings and providers [78]. Third, the confidence level of the synthesized findings according to the ConQual methodology were low or extremely low. This could affect the implications of this review. Nevertheless, the findings of this research overlap significantly with other studies that investigated the influencing factors of interprofessional collaboration in the healthcare domain [64, 65, 67,68,69, 75,76,77], suggesting that these results are still valuable.
The main strength of this review is that factors which influence interprofessional collaboration in the context of multifactorial FPIs were thoroughly examined using rigor methodology. The JBI is a well-known institute, having a widely-used checklist for critically appraising the trustworthiness, relevance and results of included articles [37]. The ConQual methodology is also widely-used approach to establish confidence in the evidence produced by qualitative systematic reviews [38]. This resulted in a comprehensive summary of the findings. Another strength was the specificity of the aim (i.e. interprofessional collaboration within the scope of multifactorial FPIs). This focus enables the transfer of findings to professionals working collaboratively within the context of falls prevention in community-dwelling older adults. Furthermore, the inductive approach to analyzing the barriers and facilitators that arose from the included studies, allowed findings to emerge from frequent, inherent, raw data into summarized, significant themes [79]. Understanding factors that may hinder or enable interprofessional collaboration in this particular context of fall prevention allows us to then design effective implementation strategies to guide further implementation efforts. The current reviews’ results suggest that in a next step of designing implementation strategies, we should focus on the results of the synthesized findings. Future research should pay attention to designing clearly defined strategies, with the goal to ensure long-term, sustainable outcomes. Next, it is necessary to evaluate these strategies for effectiveness and specify the strategies' working mechanisms. This will increase the likelihood that the strategies will eventually lead to desired implementation outcomes, aiming at improving interprofessional collaboration in fall prevention practices [80].
Conclusion
In conclusion, multiple barriers and facilitators influence interprofessional collaboration in multifactorial FPIs in community-dwelling older adults. These can be summarized into five overarching themes: communication, role clarity, information sharing, organization and interprofessional aim. This review fills an important gap in the literature by providing a comprehensive overview of synthesized findings, which can be used to develop effective implementation strategies. Applying these implementation strategies will help to improve interprofessional collaboration between health and social care professionals working in multifactorial FPIs in the community.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FPI:
-
Fall prevention interventions
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- JBI:
-
Joann Briggs Institute
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
References
World Health Organization. Factsheet Falls. Ageing and Health. 2021 [cited 2022 Mar 29]. Available from: https://www.who.int/news-room/fact-sheets/detail/falls.
Bergen G, Stevens MR, Burns ER. Falls and fall injuries among adults aged ≥65 years — United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65(37):993–8.
Berg RL, Cassels JS, (eds). The second fifty years: promoting health and preventing disability. Washington, DC: National Academy Press; 1990.
Hartholt KA, Van Beeck EF, Polinder S, Van Der Velde N, Van Lieshout EMM, Panneman MJM, et al. Societal consequences of falls in the older population: injuries, healthcare costs, and long-term reduced quality of life. Journal of Trauma - Injury, Infection and Critical Care. 2011;71(3):748–53.
Kannus P, Sievänen H, Palvanen M, Järvinen T, Parkkari J. Prevention of falls and consequent injuries in elderly people. Lancet. 2005;366:1885–93.
Soriano TA, DeCherrie LV, Thomas DC. Falls in the community-dwelling older adult: a review for primary-care providers. Clin Interv Aging. 2007;2:545–54.
Bailey C, Jones D, Goodall D. What is the evidence of the experience of having a fall across the life course? A qualitative synthesis Disabil Health J. 2014;7(3):273–84.
James SL, Lucchesi LR, Bisignano C, Castle CD, Dingels ZV, Fox JT, et al. The global burden of falls: Global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study. Inj Prev. 2017;2019:3–11.
Wiener JM, Tilly J. Population ageing in the United States of America: implications for public programmes. Int J Epidemiol. 2002;31(4):776–81.
Houry D, Florence C, Baldwin G, Stevens J, McClure R. The CDC injury center’s response to the growing public health problem of falls among older adults. Am J Lifestyle Med. 2016;10(1):74–7.
Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology. 2010;21:658–68.
Lord SR, Sherrington C, Menz HB, Close JCT. Falls in older people: Risk factors and strategies for prevention, second edition. Cambridge University Press; 2007. https://doi.org/10.1017/CBO9780511722233.
Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: a review of the literature. Maturitas. 2013;75(1):51–61.
Rubenstein LZ, Powers CM, MacLean CH. Quality indicators for the management and prevention of falls and mobility problems in vulnerable elders. Ann Intern Med. 2001;135(8 I):686–93.
Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35 Suppl 2:ii37-41.
Lee SH, Yu S. Effectiveness of multifactorial interventions in preventing falls among older adults in the community: a systematic review and meta-analysis. Int J Nurs Stud. 2020;106:103564.
Lee HC, Chang KC, Tsauo JY, Hung JW, Huang YC, Lin SI. Effects of a multifactorial fall prevention program on fall incidence and physical function in community-dwelling older adults with risk of falls. Arch Phys Med Rehabil. 2013;94(4):606–15, 615.e1.
Hopewell S, Copsey B, Nicolson P, Adedire B, Boniface G, Lamb S. Multifactorial interventions for preventing falls in older people living in the community: A systematic review and meta-analysis of 41 trials and almost 20 000 participants. Br J Sports Med. 2020;54(22):1340–50.
Speechley M. Knowledge translation for falls prevention: the view from Canada. J Safety Res. 2011;42(6):453–9.
Tan PJ, Khoo EM, Chinna K, Saedon NI, Zakaria MI, Zahedi AZA, et al. Individually-tailored multifactorial intervention to reduce falls in the Malaysian Falls Assessment and Intervention Trial (MyFAIT): a randomized controlled trial. PLoS One. 2018;13(8):e0199219.
Lamb SE, Becker C, Gillespie LD, Smith JL, Finnegan S, Potter R, et al. Reporting of complex interventions in clinical trials: development of a taxonomy to classify and describe fall-prevention interventions. Trials. 2011;12(1):125–32.
Montero-Odasso M, van der Velde N, Martin FC, Petrovic M, Tan MP, Ryg J, et al. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. 2022;51(9):afac205.
Baxter P, Markle-Reid M. An interprofessional team approach to fall prevention for older home care clients “at risk” of falling: health care providers share their experiences. Int J Integr Care. 2009;9: e15.
McKenzie G, Lasater K, Delander GE, Neal MB, Morgove M, Eckstrom E. Falls prevention education: Interprofessional training to enhance collaborative practice. Gerontol Geriatr Educ. 2017;38(2):232–43.
World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice. Practice. 2010.
Sangaleti C, Schveitzer MC, Peduzzi M, Zoboli ELCP, Soares CB. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review. JBI Database System Rev Implement Rep. 2017;15:2723–88.
Markle-Reid MF, Dykeman CS, Reimer HD, Boratto LJ, Goodall CE, McGugan JL. Engaging community organizations in falls prevention for older adults: moving from research to action. Can J Public Health. 2015;106(5):e189–96.
Van Schaik SM, O’Brien BC, Almeida SA, Adler SR. Perceptions of interprofessional teamwork in low-acuity settings: a qualitative analysis. Med Educ. 2014;48(6):583–92.
Bentley M, Freeman T, Baum F, Javanparast S. Interprofessional teamwork in comprehensive primary healthcare services: findings from a mixed methods study. J Interprof Care. 2018;32(3):274–83.
Xyrichis A, Lowton K. What fosters or prevents interprofessional teamworking in primary and community care? a literature review. Int J Nurs Stud. 2008;45(1):140–53.
Bokhour BG. Communication in interdisciplinary team meetings: what are we talking about? J Interprof Care. 2006;20(4):349–63.
Rawlinson C, Carron T, Cohidon C, Arditi C, Hong QN, Pluye P, et al. An overview of reviews on interprofessional collaboration in primary care: barriers and facilitators. Int J Integr Care. 2021;21(2):32.
Hannes K, Lockwood C. Pragmatism as the philosophical foundation for the Joanna Briggs meta-aggregative approach to qualitative evidence synthesis. J Adv Nurs. 2011;67(7):1632–42.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015: Elaboration and explanation. BMJ (Online). 2015;350:g7647.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. 2015;13(3):179–87.
Aromataris E, Munn Z, editors. JBI manual for evidence synthesis. JBI. 2020. Available from https://synthesismanual.jbi.global, https://doi.org/10.46658/JBIMES-20-01.
Munn Z, Porritt K, Lockwood C, Aromataris E, Pearson A. Establishing confidence in the output of qualitative research synthesis: the ConQual approach. BMC Med Res Methodol. 2014;14(1):108.
Gristwood J. Seeing the benefits of teamwork in falls prevention programmes. Nurs Times. 2004;100(26):39.
Nyrop KA, Zimmerman S, Sloane PD, Bangdiwala S. Fall prevention and monitoring of assisted living patients: an exploratory study of physician perspectives. J Am Med Dir Assoc. 2012;13(5):429–33.
Baumann I, Glässel A, Volken T, Rüesch P, Dratva J, Wieber F. Interprofessional collaboration in fall prevention. Eur J Public Health. 2017;27(3).
Leysens G, Vlaeyen E, Vanaken D, Janssens E, Dejaeger E, Cambier D, et al. The use of fall prevention strategies in home care: a survey in Flanders. Tijdschr Gerontol Geriatr. 2017;48(3):121–33.
Coogle CL, Zimmerman KM, Waters L, Ansello EF, Parsons P, Hogue B. Reduction in falls following an interprofessional Geriatric workforce enhancement program on evidence-based falls management and prevention. J Am Geriatr Soc. 2018;66:S75.
Bursiek AA, Hopkins MR, Breitkopf DM, Grubbs PL, Joswiak ME, Klipfel JM, et al. Use of high-fidelity simulation to enhance interdisciplinary collaboration and reduce patient falls. J Patient Saf. 2020;16(3):245–50.
Eckstrom E, Lasater K, Cotrell V, Simonson W, Neal M, Harvath T. Interprofessional, evidence-based education to reduce falls. J Am Geriatr Soc. 2012;60:S159.
Lannering C, Ernsth Bravell M, Johansson L. Prevention of falls, malnutrition and pressure ulcers among older persons - nursing staff’s experiences of a structured preventive care process. Health Soc Care Community. 2017;25(3):1011–20.
Burgon C, Darby J, Pollock K, Van Der Wardt V, Peach T, Beck L, et al. Perspectives of healthcare professionals in England on falls interventions for people with dementia: a qualitative interview study. BMJ Open. 2019;9(2):e025702.
Hamm J, Money AG, Atwal A, Ghinea G. Mobile three-dimensional visualisation technologies for clinician-led fall prevention assessments. Health Informatics J. 2019;25(3):788–810.
Whitney J, Skinner L, Brown H, Hurley M. Service users and providers perspectives of an exercise-based falls prevention programme for people with cognitive impairment. Physiotherapy (United Kingdom). 2011;97:1342–3.
Hill AM, Waldron N, Francis-Coad J, Haines T, Etherton-Beer C, Flicker L, et al. It promoted a positive culture around falls prevention’: staff response to a patient education programme-a qualitative evaluation. BMJ Open. 2016;6(12):e013414.
Redley B, Raggatt M. Use of standard risk screening and assessment forms to prevent harm to older people in Australian hospitals: a mixed methods study. BMJ Qual Saf. 2017;26(9):704–13.
Xue TM, Colón-Emeric CS, Herndon L, Hecker EJ, Berry SD, Little MO, et al. Strengthening resident, proxy, and staff engagement in injury prevention in skilled nursing facilities. Gerontologist. 2022;62(8):1112–23.
Dykeman CS, Markle-Reid MF, Boratto LJ, Bowes C, Gagné H, McGugan JL, et al. Community service provider perceptions of implementing older adult fall prevention in Ontario, Canada: a qualitative study. BMC Geriatr. 2018;18(1):34.
Yang K, Colorito KM, Bowles KH, Woomer GR, Murtaugh CM. Home care providers’ experience of translating evidence-based fall prevention programs into practice. Home Health Care Serv Q. 2019;38(3):182–93.
Markle-Reid M, Dykeman C, Ploeg J, Kelly Stradiotto C, Andrews A, Bonomo S, et al. Collaborative leadership and the implementation of community-based fall prevention initiatives: a multiple case study of public health practice within community groups. BMC Health Serv Res. 2017;17(1):141.
Grant A, Mackenzie L, Clemson L. How do general practitioners engage with allied health practitioners to prevent falls in older people? an exploratory qualitative study. Australas J Ageing. 2015;34(3):149–54.
Zimmerman KM, Davis K, Finucane S, Coogle CL, Grunden K, Marrs SA. Evaluation of an interprofessional, evidence-based falls training. Gerontol Geriatr Educ. 2021;42(2):207–23.
Jacobsohn GC, Leaf M, Liao F, Maru AP, Engstrom CJ, Salwei ME, et al. Collaborative design and implementation of a clinical decision support system for automated fall-risk identification and referrals in emergency departments. Healthcare. 2022;10(1):100598.
Middlebrook S, Mackenzie L. The enhanced primary care program and falls prevention: perceptions of private occupational therapists and physiotherapists. Australas J Ageing. 2012;31(2):72–7.
Amacher AE, Nast I, Zindel B, Schmid L, Krafft V, Niedermann K. Experiences of general practitioners, home care nurses, physiotherapists and seniors involved in a multidisciplinary home-based fall prevention programme: a mixed method study. BMC Health Serv Res. 2016;5(16):1–11.
Liddle J, Lovarini M, Clemson L, Mackenzie L, Tan A, Pit SW, et al. Making fall prevention routine in primary care practice: perspectives of allied health professionals. BMC Health Serv Res. 2018;18(1):598.
Killingback C, Chipperfield S, Clark C, Williams J. Transitions from health care to self-care: an exploratory study following structured falls interventions. Physiotherapy (United Kingdom). 2021;113: e9.
Hopewell S, Adedire O, Copsey BJ, Boniface GJ, Sherrington C, Clemson L, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;(7):CD012221. https://doi.org/10.1002/14651858.CD012221.pub2.
Bångsbo A, Dunér A, Dahlin-Ivanoff S, Lidén E. Barriers for inter-organisational collaboration: what matters for an integrated care programme? Int J Integr Care. 2022;22(2):1–10.
Kuluski K, Ho JW, Hans PK, La Nelson M. Community care for people with complex care needs: bridging the gap between health and social care. Int J Integr Care. 2017;17(4):1–11.
D’Amour D, Ferrada-Videla M, San Martin Rodriguez L, Beaulieu MD. The conceptual basis for interprofessional collaboration: core concepts and theoretical frameworks. J Interprof Care. 2005;19(SUPPL. 1):116–31.
Reeves S, Lewin S, Espin S, Zwarenstein M. Interprofessional teamwork for health and social care. 2010.
Körner M, Bütof S, Müller C, Zimmermann L, Becker S, Bengel J. Interprofessional teamwork and team interventions in chronic care: a systematic review. J Interprof Care. 2016;30(1):15–28.
D’Amour D, Goulet L, Labadie JF, Martín-Rodriguez LS, Pineault R. A model and typology of collaboration between professionals in healthcare organizations. BMC Health Serv Res. 2008;8:1–14.
Körner M. Interprofessional teamwork in medical rehabilitation: a comparison of multidisciplinary and interdisciplinary team approach. Clin Rehabil. 2010;24(8):745–55.
Montano AR, Cornell PY, Gravenstein S. Barriers and facilitators to interprofessional collaborative practice for community-dwelling older adults: an integrative review. J Clin Nurs. 2021. https://doi.org/10.1111/jocn.15991.
Busari JO, Moll FM, Duits AJ. Understanding the impact of interprofessional collaboration on the quality of care: a case report from a small-scale resource limited health care environment. J Multidiscip Healthc. 2017;10:227–34.
Suter E, Arndt J, Arthur N, Parboosingh J, Taylor E, Deutschlander S. Role understanding and effective communication as core competencies for collaborative practice. J Interprof Care. 2009;23(1):41–51.
Baumann I, Wieber F, Volken T, Rüesch P, Glässel A. Interprofessional collaboration in fall prevention: insights from a qualitative study. Int J Environ Res Public Health. 2022;19(17):10477.
Johnson JM, Hermosura BJ, Price SL, Gougeon L. Factors influencing interprofessional team collaboration when delivering care to community-dwelling seniors: a metasynthesis of Canadian interventions. J Interprof Care. 2021;35(3):376–82.
Schot E, Tummers L, Noordegraaf M. Working on working together. a systematic review on how healthcare professionals contribute to interprofessional collaboration. J Interprof Care. 2020;34(3):332–42.
Green BN, Johnson CD. Interprofessional collaboration in research, education, and clinical practice: working together for a better future. J Chiropr Educ. 2015;29(1):1–10.
Chamberlain-Salaun J, Mills J, Usher K. Terminology used to describe health care teams: an integrative review of the literature. J Multidiscip Healthc. 2013;6:65–74.
Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–46.
Springer MV, Sales AE, Islam N, McBride AC, Landis-Lewis Z, Tupper M, et al. A step toward understanding the mechanism of action of audit and feedback: a qualitative study of implementation strategies. Implement Sci. 2021;16(1):1–13.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JSCM and RZ contributed to the conception and design of the study. JSCM analyzed the data. JSCM and RZ contributed to the interpretation of results. JSCM drafted the manuscript and RZ, MS and SV critically reviewed and substantially revised the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An ethics statement is not applicable because this study is based exclusively on published literature.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Muusse, J.S.C., Zuidema, R., van Scherpenseel, M.C. et al. Influencing factors of interprofessional collaboration in multifactorial fall prevention interventions: a qualitative systematic review. BMC Prim. Care 24, 116 (2023). https://doi.org/10.1186/s12875-023-02066-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-023-02066-w