
Abstract
Obesity and depression are two common medical problems that pregnant women present with in antenatal care. Overweight and obesity at the beginning of the pregnancy, and excessive weight gain during pregnancy, are independent explanatory variables for fetal birthweight and independent risk factors for giving birth to a large for gestational age (LGA) infant. However, the effect of co-morbid depression has received little attention. This study set out to investigate if maternal body mass index (BMI) in early pregnancy moderates antenatal depression effects on infant birthweight. 3965 pregnant women participated in this longitudinal cohort study, where cases (n = 178) had Edinburgh Postnatal Depression Scale (EPDS) score ≥ 17 in gestational week 17 or 32, and remaining women (n = 3787) were used as controls. The influence of maternal BMI and antenatal depressive symptoms on standardized birthweight was evaluated by analysis of covariance, with adjustment for relevant confounders. Depressed women with BMI 25.0 kg/m2 or more gave birth to infants with significantly greater standardized birthweight than non-depressed overweight women, whereas the opposite pattern was noted in normal weight women (BMI by antenatal depressive symptoms interaction; F(1,3839) = 6.32; p = 0.012. The increased birthweight in women with co-prevalent overweight and depressive symptoms was not explained by increased weight gain during the pregnancy. Maternal BMI at the beginning of pregnancy seems to influence the association between antenatal depressive symptoms and infant birthweight, but in opposite directions depending on whether the pregnant women is normal weight or overweight. Further studies are needed to confirm our finding.
Similar content being viewed by others


Introduction
Obesity and depression are two common medical problems that pregnant women often present with in antenatal care. In the general population, these two conditions are often encountered in the same individuals, with approximately one in four obese women also being depressed1. In pregnancy, overweight and obesity are associated with a number of adverse obstetric and perinatal outcomes including preterm birth, preeclampsia and gestational diabetes2,3. In addition, overweight and obesity, as well as excessive weight gain during pregnancy, are independent explanatory variables for fetal birthweight and independent risk factors for giving birth to large for gestational age (LGA) infants4,5.
Depression during pregnancy, on the other hand, has also been associated with a number of adverse neonatal outcomes, including preterm birth and low birthweight6. Similarly, antenatal anxiety disorders and anxiety symptoms seem to increase the risk of spontaneous preterm birth and low birthweight7, and this finding has also been demonstrated in women with comorbid anxiety and depression8,9,10. Some studies also suggest that antenatal anxiety confers a stronger risk for low birthweight than antenatal depression11,12. These complications may partly be explained by the fact that antenatal mental health problems are associated with a number of characteristics that increases the risk for low birthweight such as low socioeconomic status, smoking, and drug abuse13,14,15. Indeed, a recent meta-analysis pointed to a multifaceted picture, where socioeconomic status also influenced the relationship between antenatal depression and birthweight6. At the same time, an increasing number of reports suggest that obesity is common among women with antenatal depression16,17, and two reports have suggested that antenatal depression also may lead to increased birthweight18,19.
Thus, in light of the increasing prevalence of overweight and obesity in the pregnant population, and in view of the conflicting and limited information6,20, this study aimed to investigate if maternal body mass index (BMI) in early pregnancy moderates antenatal depression effects on infant birthweight. A secondary aim was to assess if the relationship between antenatal depressive symptoms and birthweight is mediated by gestational weight gain.
Material and Methods
Primary study population
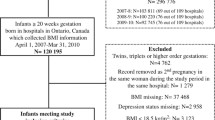
The BASIC project (Biology, Affect, Stress, Imaging, Cognition in the Puerperium) is a population-based, longitudinal study of psychological well-being during pregnancy and the postpartum period in Uppsala County, Sweden. The invitation to the BASIC study is sent out together with the invitation for the ultrasound examination around 17 weeks of gestation, and women included in this nested case-control study were included between September 2009 and January 2016. Exclusion criteria for the BASIC study are (1) inability to adequately communicate in Swedish, (2) women with confidential personal data, (3) women with pathologic pregnancies as diagnosed by routine ultrasound (miscarriages and congenital malformations), and (4) women younger than 18 years. Participation rate in the BASIC study is approximately 22%. By June 2016, 4623 participants in the BASIC project had given birth at Uppsala University Hospital. Of these, we excluded 67 twin pregnancies, 39 cases with missing infant birthweight, 297 (6.4%) women with no information on BMI at the first antenatal booking, and 255 women who entered the study after gestational week 32. Thus, the final sample size consisted of 3965 pregnant women. The proportion of women with missing information on BMI was similar to the overall Swedish population, Table 1.
The study participants completed web-based, self-administrated structured questionnaires containing questions on demographic variables, smoking, prior psychiatric history, ongoing medication, and the Swedish validated version of the Edinburgh Postnatal Depression Scale (EPDS) in gestational weeks 17 and 32.
Information on maternal BMI and maternal weight gain was obtained from the standardized antenatal medical records. Weight measurements are taken at first antenatal booking (gestational week 12), in gestational week 32, and in gestational week 36. Weight gain in gestational week 32 was defined as difference between weight in gestational week 32 and weight at first antenatal booking, and this information was available in 3731 (94.1%) women. Weight gain in gestational week 36 was available in 2252 (56.8%) women.
Women were considered to suffer from antenatal depression if they reported EPDS scores ≥ 17, either in gestational week 17 or in gestational week 32. The EPDS is an internationally used 10-item self-reported questionnaire, designed to identify depressive symptoms in the peripartum period21. While the sensitivity of the EPDS is relatively low, between 0.47–0.71, the specificity as regards depressive disorders is excellent (pooled specificity 0.94–0.98)22. The chosen cut-off was based on a recent report from the Postpartum Depression: Action Towards Causes and Treatment (PACT) Consortium, suggesting EPDS scores ≥ 17 being indicative of moderate to severe depression23. Further, a previous meta-analysis on neonatal outcomes in women with antenatal depression suggested that the relationship between birthweight and depression was stronger in women with a clinical diagnosis of depression6.
Information on maternal clinical variables, pregnancy complications, and perinatal outcomes was derived from the standardized antenatal, obstetric, and pediatric medical records. Obstetric diagnoses according to the International Classification of Diseases 10 (ICD 10) are recorded in the obstetric medical records.
Ethical approval
All participating women give written informed consent, and the BASIC study has been approved by the Independent Ethical Review Board of Uppsala, Sweden (Dnr 2009/171, approval July 1, 2009), and is conducted in accordance with the declaration of Helsinki.
Outcome
Standardized birthweight scores (SDS) according to the gestational age and sex-specific Swedish birthweight curves24 were calculated and used in the analyses. Small for gestational age (SGA) and large for gestational age (LGA) were defined as a birthweight of more than two standard deviations below or above the mean weight for gestational age according to the national reference curve, respectively24.
Comparison with the general population
The BASIC project, which is used for this nested case-control study, has a relatively low response rate (22%), and is thus susceptible to selection bias. For that reason, we wanted to present the prevalence of maternal characteristics, common obstetric complications, and the outcomes of interest (birthweight and LGA) in the primary study population, in the entire population of women giving birth in Uppsala County, and in the general Swedish population.
For this part, we used information from the Swedish Medical Birth Register, which is hosted by The Swedish National Board of Health and Welfare. In addition, information on educational level and origin of birth was provided by Statistics Sweden, with data from the Education Register and the Register of the Total Population, respectively. Individual record linkage between the registries was possible by use of unique personal registration numbers, which are assigned to Swedish residents at birth or upon immigration.
The Medical Birth Register contains data on 98% of all births in Sweden and includes prospectively collected data from the standardized antenatal, obstetric, and pediatric medical records, including reproductive history, smoking status, complications that occur during pregnancy, delivery, and the neonatal period. Complications during pregnancy and delivery are classified according to ICD 10, as noted by the responsible obstetrician at discharge from the hospital. For comparison with the BASIC study population, all mothers with singleton pregnancies, giving birth between January 1, 2009 and December 31, 2014, in Uppsala County (n = 23352) and remaining Sweden (n = 625118) were included in the two control study populations.
Statistics
Comparisons between depressed and non-depressed women in the BASIC cohort were performed by independent t-tests and Chi-square tests. Correlations were performed by Spearman Rank correlation, as self-rated depression scores failed to meet the assumption of normal distribution.
The influence of maternal BMI and antenatal depression on standardized birthweight (continuous, and large for gestational age (yes/no)) was evaluated by analysis of covariance (ANCOVA) or logistic regression. In both analyses BMI (categorized as BMI < 25.0 kg/m2 vs. BMI ≥ 25.0 kg/m2) and depression status (case vs. control) were entered as fixed factors, evaluating the main effects of BMI and depressive symptoms as well as the interaction between these two factors. The BMI cut-off was chosen to capture overweight and obesity, and was chosen to yield relatively comparable group sizes. The ANCOVA and logistic regression model were adjusted for age (continuous), parity (nulliparous vs. parous), maternal height (continuous), maternal education (more or less than 12 years of education), maternal origin of birth (Nordic vs. non-Nordic), and smoking (yes/no), and in a second step also with BMI as a continuous variable. These covariates were chosen based on the findings in the bivariate analyses, whereas smoking and parity were forced into the model based on previous literature13.
Follow-up linear regression models were performed using dummy variables corresponding to (1) normal weight non-depressed women (reference) (2) normal weight women with depressive symptoms, (3) non-depressed overweight women, and (4) overweight women with depressive symptoms. This regression model was performed in two steps; model 1 incorporating potential confounders as described above, and model 2 incorporating weight gain in gestational week 32 as a potential mediator.
Results
Study population
While the BASIC study population differed from Uppsala County and remaining Sweden in some aspects, most notably the higher educational level and lower rate of women with non-Nordic origin, maternal BMI, birthweight, and prevalence of LGA infants were similar to the general population, Table 1.
Overall, 178 (4.5%) women were classified as depressed, whereas remaining women were used as controls (n = 3787). Women who were classified as depressed were younger, significantly less often cohabiting, had a lower educational level, and were less often of Nordic origin, Table 2. They had a similar BMI distribution, and had similar rates of common pre-pregnancy conditions and obstetric complications as the controls. Further, women with antenatal depressive symptoms gave birth to offspring with lower birthweight; however, the standardized birthweight did not differ from the controls, Table 2.
Infant birthweight in relation to covariates
Standardized birthweight was in significant positive correlation with first trimester BMI, maternal height, gestational weight gain, and self-rated depression scores in gestational week 17, Table 3. Standardized birthweight was also significantly associated with parity, non-Nordic origin, and educational level, Supplementary Table 1.
Infant birthweight in relation to depressive symptoms and BMI
The interaction between antenatal depressive symptoms, maternal BMI and standardized birthweight was investigated by ANCOVA. Following adjustment for confounders a significant interaction between BMI and depression case-control status was noted, F(1,3840) = 6.82; p = 0.009, Fig. 1. This interaction remained unchanged when BMI, as a continuous variable, was entered as an additional covariable in the model, F(1,3839) = 6.32; p = 0.012. The interaction was primarily driven by depressed women with BMI 25 or more who gave birth to infants with greater birthweight than non-depressed overweight women, whereas the opposite pattern was noted in normal weight women, Table 4 (Model 1). When using LGA as outcome, a significant interaction between antenatal depressive symptoms and maternal BMI was also noted; AOR 3.73, 95% CI (1.62–8.51). However, this interaction did not remain following adjustment for BMI as a continuous variable; AOR 2.09, 95% CI (0.98–4.98).

Interaction between maternal BMI and antenatal depression on standardized birthweight.
The effect on birthweight is not mediated by greater weight gain in depressed women
Self-rated depression scores in gestational week 17 and 32 were in weak, but positive, correlation with maternal weight gain, both at gestational week 32 and 36, Table 3. The interaction between antenatal depressive symptoms, maternal weight gain (dichotomized at the median) and standardized birthweight was investigated by ANCOVA. Following adjustment for confounders a significant main effect of weight gain and birthweight was noted F(1,3613) = 19.62; p < 0.001, however, we found no interaction between weight gain and depression case-control status, F(1,3613) = 0.032; p = 0.857.
Further, when weight gain was entered in the linear regression analysis on BMI and depressive symptoms’ influence on standardized birthweight, the estimates were only marginally changed, Table 4 (Model 2). Thus, we pursued no path analyses on the mediating effect of weight gain.
Discussion
Our results suggest that women who are both overweight and have symptoms of moderate to severe depression during pregnancy give birth to infants with greater birthweight than non-depressed overweight women. The opposite pattern was noted in normal weight women, although the difference between depressed and healthy normal-weight women was not significant.
Most previous studies on depression and birthweight have suggested an association with lower birth weight6, although there are some exceptions. For instance, Andersson et al. found a borderline-significant association between antenatal depressive disorder and birthweight of 4000 grams or more, although the association was lost when adjusted for maternal BMI18. Similarly, results from a large Canadian study suggested that the prevalence of macrosomia (>4500 g) and LGA infants were highest among the overweight or obese women with comorbid depression19. The significant interaction between depressive symptoms and maternal BMI noted in our study may help explain the discrepancies between our and prior results. First, as many other studies we find lower birth weight in the women who were classified as depressed, but importantly, no difference in standardized birthweight. Secondly, according to the interaction analysis, overweight women with antenatal depressive symptoms tend to give birth to children with higher birthweight, whereas the opposite pattern was seen in normal weight women with antenatal depressive symptoms, who instead tended to give birth to children with lower birthweight. Potentially, in populations with a greater proportion of normal weight or underweight women, the tendency towards lower birthweight, as noted in this study, is amplified. This is in line with the meta-analysis by Grote and co-workers where the association between antenatal depression and low birthweight was stronger in studies including women from develo** countries or women with low socioeconomic status in the U.S6. The low birthweight noted in some studies may be the result of undeveloped or unequal maternal health care, whereas optimized maternal surveillance is able to counteract the depressogenic effects leading to low birthweight. Also, previous studies have not always addressed birthweight in relation to gestational length, why low birthweight simply may be the result of a depression-induced increased prevalence of preterm birth6. Finally, risk factors for low birthweight, such as smoking and low educational level, were less prevalent in our women than in the general pregnant population. Thus, the study population may be selected towards socioeconomic factors that drive the association in the opposite direction.
The increased birthweight in women with co-prevalent overweight and depressive symptoms was not explained by increased weight gain. Thus, the mechanism behind the influence of maternal BMI and antenatal depression on birthweight can only be speculated upon. Fetal growth is directly related to maternal nutrient availability and the ability of the placenta to transport these nutrients from maternal circulation to the fetus. In order to sustain appropriate fetal development the mother has to provide glucose, amino acids, and fatty acids to the fetus via the placenta25. Normal pregnancy is associated with insulin resistance and enhanced maternal hepatic glucose production26, both of which lead to increased glucose shunting to the fetus, fetal hyperinsulinemia, and enhanced fetal growth. We have recently demonstrated that placental gene expression in LGA infants born to non-diabetic mothers affects networks important for lipid metabolism, with insulin-like growth factor binding protein 1 being one of the top up-regulated genes, and leptin being a top down-regulated gene27. Leptin levels are as of yet unstudied in antenatal depression, but leptin levels at delivery are negatively associated with self-reported postpartum depressive symptoms28. Further, in non-pregnant women many factors, both peripheral and central, concerned with cell-mediated immunity, inflammation and oxidative and nitrosative stress, are related to the onset of depressive symptomes29. While the information on inflammatory response in women with antenatal depression is limited and inconsistent thus far30, we have recently provided evidence for an misadaptive switch to the anti-inflammatory milieu of the third trimester in women with antenatal depression31. Finally, the hypothalamus-pituitary-adrenal (HPA) axis is yet another potential link between maternal overweight, antenatal depression and neonatal complications32. In depressed pregnant women the HPA alterations seem to be regulated differently than in healthy pregnant women32,33,34,35,36. We and others have demonstrated that the cortisol to cortisone ratio, potentially a marker of maternal and placental 11β-hydroxy steroid dehydrogenase 2 activity, is positively associated with birthweight in women with psychiatric morbidity36,37. By this mechanism, psychiatric morbidity seems to increase fetal exposure to cortisol, which ultimately will influence fetal growth.
Our study has a number of limitations that should be mentioned. First, the study population consists of women with higher education level and lower rate of non-Nordic women than the general population, and therefore can we assume that our study group has a higher socio-economic status than average, and a healthy selection bias. However, for the outcomes of interest we note a numerically similar birthweight and a similar prevalence of LGA infants as in the general population. We used EPDS, a self-reported screening for antenatal depression, and not a psychiatric interview for establishment of depression diagnoses based on DSM-5 criteria. We tried to compensate for this by using to cut-off of 17 or more in the EPDS for our cases, which yielded a prevalence of antenatal depression within the range reported in the literature38. Further, given the established relationship between anxiety and birthweight, and especially comorbid anxiety and depression influence on birth weight, further insight could have been gained if antenatal anxiety had been captured in this study as well.
In conclusion, our study has revealed that first trimester maternal body mass index seems to modulate the association between antenatal depressive symptoms and birthweight. It remains to determine if our results can be conveyed to other populations or settings, and further insight is needed on the potential mechanisms underlying our findings. Nevertheless, this result emphasizes the importance of prevention, diagnosis and treatment of women with overweight and depression during pregnancy to minimize the complications for both the mother and the infant. Mental health problems are common comorbidities in obese women, and clinicians should actively ask about depressive and anxiety symptoms at the first antenatal booking. Further, these women should be counselled on physical activity and life style interventions during pregnancy, as this may limit the adverse outcomes for both mother and child.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Carey, M. et al. Prevalence of comorbid depression and obesity in general practice: a cross-sectional survey. The British journal of general practice: the journal of the Royal College of General Practitioners 64, e122–127 (2014).
Catalano, P. M. & Shankar, K. Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ (Clinical research ed.) 356, j1 (2017).
Persson, M. et al. Risk of major congenital malformations in relation to maternal overweight and obesity severity: cohort study of 1.2 million singletons. BMJ (Clinical research ed.) 357, j2563 (2017).
Kim, S. Y., Sharma, A. J., Sappenfield, W., Wilson, H. G. & Salihu, H. M. Association of maternal body mass index, excessive weight gain, and gestational diabetes mellitus with large-for-gestational-age births. Obstetrics and gynecology 123, 737–744 (2014).
Yu, Z. et al. Pre-pregnancy body mass index in relation to infant birth weight and offspring overweight/obesity: a systematic review and meta-analysis. PloS one 8, e61627 (2013).
Grote, N. K. et al. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Archives of general psychiatry 67, 1012–1024 (2010).
Grigoriadis, S. et al. Maternal Anxiety During Pregnancy and the Association With Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis. The Journal of clinical psychiatry 79 (2018).
Betts, K. S., Williams, G. M., Najman, J. M., Scott, J. & Alati, R. The association between lower birth weight and comorbid generalised anxiety and major depressive disorder. Journal of affective disorders 146, 231–237 (2013).
Field, T. et al. Comorbid depression and anxiety effects on pregnancy and neonatal outcome. Infant behavior & development 33, 23–29 (2010).
Yang, S. et al. Symptoms of anxiety and depression during pregnancy and their association with low birth weight in Chinese women: a nested case control study. Archives of women’s mental health 20, 283–290 (2017).
Uguz, F. et al. The effects of maternal major depression, generalized anxiety disorder, and panic disorder on birth weight and gestational age: a comparative study. Journal of psychosomatic research 75, 87–89 (2013).
Pinto, T. M., Caldas, F., Nogueira-Silva, C. & Figueiredo, B. Maternal depression and anxiety and fetal-neonatal growth. Jornal de pediatria 93, 452–459 (2017).
Cnattingius, S. The epidemiology of smoking during pregnancy: smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine & tobacco research: official journal of the Society for Research on Nicotine and Tobacco 6(Suppl 2), S125–140 (2004).
Kramer, M. S. Determinants of low birth weight: methodological assessment and meta-analysis. Bulletin of the World Health Organization 65, 663–737 (1987).
Thompson, J. M. et al. Risk factors for small-for-gestational-age babies: The Auckland Birthweight Collaborative Study. Journal of paediatrics and child health 37, 369–375 (2001).
Andersson, L., Sundstrom-Poromaa, I., Wulff, M., Astrom, M. & Bixo, M. Implications of antenatal depression and anxiety for obstetric outcome. Obstetrics and gynecology 104, 467–476 (2004).
Molyneaux, E., Poston, L., Ashurst-Williams, S. & Howard, L. M. Pre-pregnancy obesity and mental disorders during pregnancy and postpartum: A systematic review and meta-analysis. Pregnancy hypertension 4, 236 (2014).
Andersson, L., Sundstrom-Poromaa, I., Wulff, M., Astrom, M. & Bixo, M. Neonatal outcome following maternal antenatal depression and anxiety: a population-based study. Am J Epidemiol 159, 872–881 (2004).
McDonald, S. D. et al. The combined effects of maternal depression and excess weight on neonatal outcomes. International journal of obesity 39, 1033–1040 (2015).
Lutsiv, O. et al. Pregnancy complications associated with the co-prevalence of excess maternal weight and depression. International journal of obesity (2005) 39, 1710–1716 (2015).
Cox, J. L., Holden, J. M. & Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. The British journal of psychiatry: the journal of mental science 150, 782–786 (1987).
National Collaborating Centre for Mental, H. National Institute for Health and Clinical Excellence: Guidance. In Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance: Updated edition (British Psychological Society, Leicester (UK), 2014).
Putnam, K. T. et al. Clinical phenotypes of perinatal depression and time of symptom onset: analysis of data from an international consortium. The lancet. Psychiatry 4, 477–485 (2017).
Marsal, K. et al. Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta paediatrica (Oslo, Norway: 1992) 85, 843–848 (1996).
Brett, K. E., Ferraro, Z. M., Yockell-Lelievre, J., Gruslin, A. & Adamo, K. B. Maternal-fetal nutrient transport in pregnancy pathologies: the role of the placenta. International journal of molecular sciences 15, 16153–16185 (2014).
Hodson, K. et al. Mechanism of insulin resistance in normal pregnancy. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme 45, 567–571 (2013).
Ahlsson, F., Akerud, H., Schijven, D., Olivier, J. & Sundstrom-Poromaa, I. Gene Expression in Placentas From Nondiabetic Women Giving Birth to Large for Gestational Age Infants. Reproductive sciences (Thousand Oaks, Calif.) 22, 1281–1288 (2015).
Skalkidou, A. et al. Risk of postpartum depression in association with serum leptin and interleukin-6 levels at delivery: a nested case-control study within the UPPSAT cohort. Psychoneuroendocrinology 34, 1329–1337 (2009).
Leonard, B. & Maes, M. Mechanistic explanations how cell-mediated immune activation, inflammation and oxidative and nitrosative stress pathways and their sequels and concomitants play a role in the pathophysiology of unipolar depression. Neuroscience and biobehavioral reviews 36, 764–785 (2012).
Osborne, L. M. & Monk, C. Perinatal depression–the fourth inflammatory morbidity of pregnancy?: Theory and literature review. Psychoneuroendocrinology 38, 1929–1952 (2013).
Edvinsson, A. et al. Lower inflammatory markers in women with antenatal depression brings the M1/M2 balance into focus from a new direction. Psychoneuroendocrinology 80, 15–25 (2017).
Horowitz, M. A., Zunszain, P. A., Anacker, C., Musaelyan, K. & Pariante, C. M. Glucocorticoids and inflammation: a double-headed sword in depression? How do neuroendocrine and inflammatory pathways interact during stress to contribute to the pathogenesis of depression? Modern trends in pharmacopsychiatry 28, 127–143 (2013).
Iliadis, S. I. et al. Prenatal and Postpartum Evening Salivary Cortisol Levels in Association with Peripartum Depressive Symptoms. PloS one 10, e0135471 (2015).
Hannerfors, A. K. et al. Treatment with serotonin reuptake inhibitors during pregnancy is associated with elevated corticotropin-releasing hormone levels. Psychoneuroendocrinology 58, 104–113 (2015).
Hellgren, C., Akerud, H., Skalkidou, A. & Sundstrom-Poromaa, I. Cortisol awakening response in late pregnancy in women with previous or ongoing depression. Psychoneuroendocrinology 38, 3150–3154 (2013).
Hellgren, C. et al. Tandem mass spectrometry determined maternal cortisone to cortisol ratio and psychiatric morbidity during pregnancy-interaction with birth weight. Psychoneuroendocrinology 69, 142–149 (2016).
Wilson, M. & Thayer, Z. Maternal salivary cortisone to cortisol ratio in late pregnancy: An improved method for predicting offspring birth weight. Psychoneuroendocrinology 78, 10–13 (2017).
Andersson, L. et al. Point prevalence of psychiatric disorders during the second trimester of pregnancy: a population-based study. American journal of obstetrics and gynecology 189, 148–154 (2003).
Author information
Authors and Affiliations
Contributions
Authors A.S., K.E., A.M.-L., A.-K.W. and I.S.P. conceived and designed the study. Authors H.P.M., A.S. and I.S.P. performed the statistical analyses, and a first draft of the manuscript was written by H.P.M. All authors contributed to the interpretation, and the writing of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Petursdottir Maack, H., Skalkidou, A., Sjöholm, A. et al. Maternal body mass index moderates antenatal depression effects on infant birthweight. Sci Rep 9, 6213 (2019). https://doi.org/10.1038/s41598-019-42360-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-42360-1
- Springer Nature Limited