
Abstract
Blood pressure (BP) variability and nocturnal decline in blood pressure are associated with cardiovascular outcomes. However, little is known about whether these indexes are associated with white-coat and masked hypertension. We performed a cross-sectional analysis of 1047 community-dwelling individuals aged ⩾60 years in Spain in 2012. Three observer-measured home BPs and 24-h ambulatory blood pressure monitoring (ABPM) were performed under standardized conditions. BP variability was defined as BP s.d. and coefficient of variation. Differences in BP variability and nocturnal BP decrease between groups were adjusted for sociodemographic and clinical covariates using generalized linear models. Of the cohort, 21.7% had white-coat hypertension, 7.0% had masked hypertension, 21.4% had sustained hypertension, and 49.9% were normotensive. Twenty-four hour, daytime and night-time systolic BP s.d. and coefficients of variation were significantly higher in subjects with white-coat hypertension than those with normotension (P<0.05) and were similar to subjects with sustained hypertension. In untreated subjects, 24-h but not daytime or night-time BP variability indexes were significantly higher in subjects with white-coat hypertension than in those with normotension (P<0.05). Percentage decrease in nocturnal systolic and diastolic BP was greatest in the white-coat hypertension group and lowest in the masked hypertension group in all patients and untreated patients (P<0.05). Lack of nocturnal decline in systolic blood pressure was observed in 70.2% of subjects with normotension, 57.8% of subjects with white-coat hypertension, 78.1% of subjects with masked hypertension, and 72.2% of subjects with sustained hypertension (P<0.001). In conclusion, 24-h BP variability was higher in subjects with white-coat hypertension and blunted nocturnal BP decrease was observed more frequently in subjects with masked hypertension. These findings may help to explain the reports of increased cardiovascular risk in patients with white-coat hypertension and poor prognosis in those with masked hypertension, highlighting the importance of ABPM.
Similar content being viewed by others


Introduction
Conventional measurement of blood pressure (BP) in a medical office is the standard method for the diagnosis and management of hypertension. However, there are several limitations to this approach, including apparently innocent elevations of BP that only occur in the clinic (white-coat hypertension) or the observation of normal readings when, in fact, the patient is hypertensive (masked hypertension).1, 2 Numerous reports of a wide variety of conditions and populations have demonstrated that ambulatory BP monitoring (ABPM) is superior to office-based measurement with respect to cardiovascular risk assessment.3, 4
BP not only exhibits large circadian variations in terms of changes between day and night but also changes from minute-to-minute and hour-to-hour in both hypertensive and normotensive patients.5 Thus, non-invasive 24-h ABPM is a robust method to assess short-term BP variability within 24 h.6
Most studies have found that high 24-h BP variability is associated with organ damage and may contribute to cardiovascular risk prediction, over and beyond mean BP.7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17 However, the degree to which variability improves the prediction of cardiovascular risk is controversial.18, 19, 20 Previous studies have shown that night-time BP is generally a better predictor of cardiovascular outcomes than daytime BP in patients with hypertension, and diminished nocturnal decline in BP is associated with or predictive of organ damage and cardiovascular events.21, 22, 23, 24, 25, 26
Only a few studies have analyzed whether different phenotypes on the hypertension spectrum such as normotension, white-coat hypertension, masked hypertension, and sustained hypertension are associated with BP variability independent of mean BP.27, 28 As far as we know, there are no reports about circadian variability and BP variability in daytime and night-time periods across the various BP phenotypes. It is possible that the reported increases in cardiovascular risk in patients with white-coat hypertension or masked hypertension2 could be attributed, at least in part, to BP variability and nocturnal decline in BP. The objective of this study was to describe the relationships between mean daytime and night-time ambulatory BP, BP variability and nocturnal decline in BP with subjects with normotension and white-coat, masked and sustained hypertension in a cross-sectional analysis of older adults in Spain.29
Methods
Study design and population
Data are taken from the Seniors-ENRICA cohort, and the methods have been previously reported.29, 30 In brief, this cohort was established in 2008-2010 with 2614 individuals selected through stratified random sampling from the population of individuals in Spain aged ⩾60 years.29 Baseline information on sociodemographic variables, lifestyle, health status, and morbidity was collected by telephone interview. In addition, a home visit was conducted to collect blood samples, and another home visit was conducted to perform a physical examination and to record dietary habits and prescribed medications. Participants were followed until 2012, when a second wave of data collection was performed. At this time point, of the 2519 surviving subjects, 2037 provided updated information for the telephone interview, physical examination, diet, and medication. ABPM was offered to 1698 individuals in this second wave for cost and logistical reasons, and the analysis was performed in 1328 subjects (response rate, 78.2%). The subjects who underwent ABPM had similar characteristics to those who did not in terms of age, sex, education level, obesity, diabetes, current smoking and previous history of cardiovascular disease.
Personnel involved in data collection received specific training in the study procedures. Study participants gave written informed consent. The study was approved by the Clinical Research Ethics Committee of the ‘La Paz’ University Hospital in Madrid.
Study variables
Study participants reported their age, sex and smoking status. Weight and height were measured in each subject under standardized conditions. Body mass index (BMI) was calculated as weight in kilograms divided by the square of the height in meters. Study subjects reported whether they had been previously diagnosed with hypercholesterolemia or cardiovascular disease (myocardial infarction, stroke and heart failure). Diabetes mellitus was identified as fasting serum glucose ⩾126 mg dl−1 or treatment with oral antidiabetic drugs or insulin. Medication use was assessed by a face-to-face interview and verified against drug packaging during the home visits.
Blood pressure measurement
BP was measured using standardized procedures and conditions, with validated automatic devices (Omron M6) and appropriate-sized cuffs. Trained observers measured each participant’s BP during a home visit: three measurements were taken at two-minute intervals after resting for five minutes in a seated position. In the analyses, BP was calculated as the mean of the last two of the three readings. Thereafter, 24-h ABPM was performed using a validated automated non-invasive oscillometric device (Microlife WatchBPO3 monitor),31 programmed to measure BP at 20-min intervals during the day and at 30-min intervals during the night for a 24-h period. Appropriate cuff sizes were used. The majority of measurements were performed on working days, and the patients were instructed to maintain their usual activities but keep the arm extended and immobile at the time of cuff inflation. Valid ABPM measurements had to fulfill several pre-established criteria, including 24-h duration and at least 70% of systolic BP (SBP) and diastolic BP (DBP) successful recordings during the daytime and night-time periods.1, 2, 32 Daytime and night-time periods were defined individually according to the patient’s self-reported time of going to bed and waking up. On the basis of international guidelines,1, 2, 32 white-coat hypertension was defined as conventional BP ⩾140/90 mm Hg and 24-h ABPM <130/80 mm Hg; masked hypertension was defined as conventional BP <140/90 mm Hg and 24-h ABPM ⩾130/80 mm Hg; sustained hypertension was defined as conventional BP ⩾140/90 mm Hg and 24-h ABPM ⩾130/80 mm Hg; normotension was defined as conventional BP <140/90 mm Hg and 24-h ABPM <130/80 mm Hg. We have used these terms for the sake of simplicity. However, among untreated patients, the terms normotension, white-coat hypertension, masked hypertension, and sustained hypertension would be more correct, and among treated patients, the terms controlled hypertension, white-coat uncontrolled hypertension, masked uncontrolled hypertension, and uncontrolled hypertension would be appropriate. Short-term variability was assessed by the s.d. and the coefficient of variation (CV) [s.d./mean × 100%] of SBP and DBP in 24 h, daytime and night-time periods. Nocturnal decrease in SBP and DBP was measured in both absolute terms (mm Hg) and relative terms and as BP dip** (non-dip** was defined as nocturnal BP decrease <10% of daytime BP).1, 2, 32
Statistical analyses
For descriptive analysis, we used the mean and s.d. for continuous variables and the percentage distribution of frequencies for categorical variables. To compare means between groups, we used Student’s t-test and analysis of variance. For comparison of percentages, the χ2-test was used.
Mean ambulatory BPs, BP variability indexes and nocturnal decrease in BP were compared between BP phenotypes using generalized linear model analyses, adjusting for age, sex, BMI, smoking, diabetes, dyslipidemia, previous cardiovascular diseases, antihypertensive treatment (yes/no) and mean ambulatory SBP or DBP according to the time period, as appropriate. We also performed a separate analysis of mean ambulatory BPs and BP variability indexes in untreated subjects. Lastly, we analyzed the percentage reduction of nocturnal BP according to treatment status and adjusted for the covariates listed above. The Bonferroni correction was used for post hoc multiple comparisons. Statistical significance was established at P<0.05. The Statistical Package for Social Sciences (SPSS) for Windows version 19.0 software (SPSS, IBM, Armonk, NY, USA) was used for statistical analysis.
Results
A total of 1047 individuals (mean age 71.7 years, 50.8% men) with ⩾70% valid ABPM readings and complete information on the study variables were used for analysis (80% of all individuals with available ABPM). The mean conventional SBP/DBP was 137.8/74.0 mm Hg, and the mean BMI was 27.8 kg m−2; 49.5% of subjects had hypercholesterolemia, 14.9% had diabetes, 5.7% had cardiovascular disease, and 42.9% were treated with an antihypertensive medication (Table 1). After ABPM, the global distribution of subjects was as follows: 49.9% had normotension (or controlled hypertension in treated subjects), 21.7% had white-coat hypertension (or white-coat uncontrolled hypertension in treated subjects), 7.0% had masked hypertension (or masked uncontrolled hypertension in treated subjects) and 21.4% had sustained hypertension (or uncontrolled hypertension in treated subjects; Table 1).
After adjusting for demographic and clinical covariates (including mean ambulatory BP and antihypertensive treatment), systolic and diastolic 24-h BP variability indexes were significantly higher in individuals with white-coat hypertension than in those with normotension (Table 2). As expected, mean systolic and diastolic 24-h BPs were higher in subjects with masked hypertension relative to subjects with white-coat hypertension. We did not observe any differences between 24-h BP variability indexes in subjects with masked vs. white-coat hypertension or between subjects with sustained vs. masked hypertension. During the daytime, systolic BP variability indexes were higher in individuals with white-coat hypertension than in those with normotension. No differences between diurnal BP variability indexes were observed between subjects with masked vs. white-coat hypertension or sustained vs. masked hypertension. During the night, systolic BP variability indexes were higher in individuals with white-coat hypertension relative to those with normotension. We observed no differences in systolic and diastolic BP variability indexes in subjects with sustained vs. masked hypertension or masked vs. white-coat hypertension. Furthermore, no differences were observed in night-time mean systolic and diastolic BP in subjects with sustained vs. masked hypertension. Table 3 shows mean systolic and diastolic 24-h pressures, day and night mean BPs, and BP variability indexes in untreated subjects. Notably, we observed a significant difference in mean 24-h BPs and 24-h variability indexes in subjects with white-coat hypertension vs. normotension, similar to our observations in the cohort as a whole. However, we did not observe any differences in day and night BP variability indexes between subjects with different hypertension phenotypes.
The proportion of systolic non-dip** was 70.2% (95% confidence interval (CI): 66.0–74.0%) in subjects with normotension, 57.8% (95% CI: 51.6–63.8%) in subjects with white-coat hypertension, 78.1% (95% CI: 66.6–86.5%) in subjects with masked hypertension, and 72.2% (95% CI: 66.1–77.6%) in subjects with sustained hypertension (P<0.001). The proportion of diastolic non-dip** was 51.0% (95% CI: 46.6–55.4%) in subjects with normotension, 35.7% (95% CI: 30.0–41.8%) in subjects with white-coat hypertension, 64.1% (95% CI: 51.8–74.7%) in subjects with masked hypertension, and 50.0% (95% CI: 43.6–56.3%) in subjects with sustained hypertension (P<0.001). These differences were maintained in untreated subjects but not in treated subjects (data not shown).
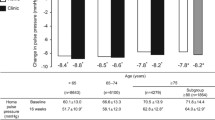
Table 4 shows the percentage decrease in nocturnal systolic and diastolic BP according to antihypertensive treatment status and adjusted for demographic and clinical covariates. In the whole cohort, as well as untreated patients, the relative reduction in systolic and diastolic BP was greatest in subjects with white-coat hypertension and lowest in those with masked hypertension. Significant differences were observed in subjects with white-coat hypertension vs. normotension, masked vs. white-coat hypertension and sustained vs. masked hypertension (P<0.05).
Discussion
This study performed in a cohort of community-dwellers in Spain aged ⩾60 years found the following: (i) a higher ambulatory 24-h BP variability in individuals with white-coat hypertension than in those with normotension (and similar to that in those with sustained hypertension), and (ii) diminished rates of night-time BP dip** and a higher proportion of non-dip** in subjects with masked hypertension than those with normotension, independent of important sociodemographic and clinical covariates. These results were only maintained when untreated patients were considered. These findings may be pertinent to the reports that patients with white-coat hypertension have higher cardiovascular risk than those with normotension.33, 34, 35 Furthermore, the observation that those patients with masked hypertension have a worse prognosis than those with white-coat hypertension could be partly explained by both the higher mean ambulatory BPs at all time periods (including slee**) and the diminished nocturnal BP dip. This reinforces the importance of ABPM as a helpful tool to establish the diagnosis and prognosis of BP phenotypes. To the best of our knowledge, no previous studies have focused on these relationships including overnight examination.
The reported frequency of white-coat and masked hypertension ranges from 10 to 50%36 depending on the cut-offs used for normal ambulatory BP and the study population. Thus, the apparent low frequency of white-coat and masked hypertension in our study (21.7% and 7.0%, respectively) is noteworthy in comparison to other studies that included thresholds of 140/90 mm Hg for clinic BP and 135/85 mm Hg in daytime BP36 but that ignored the night-time period. Such an omission may lead to overestimation of the frequency of white-coat and masked hypertension. We have used 140/90 mm Hg as a threshold for observer-measured home BP and 130/80 mm Hg in 24-h ambulatory BP that included nocturnal BP values and could thus be considered a relatively exigent scenario. Although any time interval suffices to diagnose masked hypertension, as proposed in current guidelines, full 24-h recordings remain standard in clinical practice.37 The higher 24-h BP variability in subjects with white-coat hypertension may help to explain the higher rates of cardiovascular risk that have been reported in previous studies of these patients.33, 34, 35 BP variability depends on sympathetic vascular modulation and changes in arterial distensibility. Higher short-term BP variability in subjects with white-coat hypertension than in those with normotension has been reported in a few other studies38, 39 and may be intrinsic or an enhanced stress response to external stimuli. Alternatively, it may reflect a diffuse atherosclerotic process induced by aging and hypertension that leads to increased stiffness of the large elastic arteries and/or depressed baroreflex functions causing impaired cardiovascular control mechanisms.5 In addition, we postulate that mechanisms other than sympathetic activity are operating in white-coat hypertension, since this activity correlates with the level and s.d. of BP, but not with the coefficient of variation, a measure of variability that is less dependent on the level of BP than the s.d.40 It is noteworthy that in patients with antihypertensive treatment, we did not observe any differences in BP variability indexes. So, it is possible that antihypertensive treatment controls BP variability independent of mean BP. This may be a future target for controlling BP.
There is strong evidence that patients with masked hypertension are at increased risk of target organ damage and cardiovascular morbidity,2, 41, 42 with an overall cardiovascular risk approaching that of patients with sustained hypertension.43 In our study, the higher level of mean night-time BP in patients with masked hypertension (vs. those with white-coat hypertension or normotension and no difference when compared to those with sustained hypertension) may also explain the poorer prognosis of patients with masked hypertension in comparison with those with white-coat hypertension. This is in line with several observational and longitudinal analyses demonstrating the superior value of nocturnal BP compared with daytime BP in predicting cardiovascular events and all-cause mortality.19, 24, 43 Nocturnal BP at resting conditions is the minimum BP needed for adequate organ perfusion, and high BP at night could overload the cardiovascular system and lead to negative effects on the heart and vascular structures.44 Mentally stressful situations have been associated with masked hypertension and high BP variability.45
In this study, the high frequency of systolic and diastolic non-dip** and the significant decrease in nocturnal BP decline in patients with masked hypertension after adjusting for ambulatory BP levels, antihypertensive drug treatment, and other covariates could help to explain why patients with masked hypertension have a poor prognosis. It has been reported that non-dip** and diminished decline in nocturnal BP is associated with organ damage and poor cardiovascular outcomes both in population studies and in hypertensive patients.46, 47, 48, 49 It is noteworthy that in patients with pharmacological treatment, we did not observe any differences in nocturnal BP declines between groups. So, it is possible that antihypertensive treatment may affect nocturnal BP decline independent of mean BP. This may be a target for future BP control.
Night-time masked hypertension is observed in various conditions that produce non-dip** status, including high salt intake, renal dysfunction, obesity, sleep apnea, and autonomic failure.50 In particular, investigation of nocturnal BP and decline in nocturnal BP using ABPM suggest that this process is salt sensitive, which is associated with increased sympathetic activity and increased cardiovascular risk.51 Non-dip** could reflect an inadequacy of the mechanisms regulating BP; it could be the result of baroreflex or autonomic dysfunction, relative nocturnal volume overload, or abnormal sodium handling. ABPM can refine the prognostic assessment in hypertension not only by providing an accurate BP value that is the average of a large number of BP measurements but also by assessing circadian variability, a parameter which requires ABPM.44
Given that this study was not strictly representative of the general older population of Spain, extrapolations should be interpreted with caution. Nevertheless, the baseline sociodemographic and clinical characteristics of the participants were similar to those who did not participate. It should be noted that in this study, conventional BP was not measured in the office or clinic but in subjects’ homes as in other studies,52 thereby decreasing the effect of anxiety and giving more realistic estimates. Nevertheless, we used the 140/90 mm Hg target for the primary analysis of conventional BP, since BP was measured on only one occasion and involved a technique similar to that used for office BP measurements. Furthermore, although white-coat and masked hypertension are not entirely accurate terms and ‘isolated home BP elevation’ or ‘isolated ambulatory BP elevation,’ are more appropriate and descriptive terms, we have maintained the terms ‘white coat’ and ‘masked’ hypertension for the sake of clarity and comparison with other studies. Lastly, determination of antihypertensive therapy was based on the participant’s self-report and may, therefore, be inaccurate; however, medications were checked against prescription containers. Finally, the cross-sectional design prevents us from assessing causal relationships between the associations we report.
In conclusion, we found that 24-h BP variability was higher in subjects with white-coat hypertension than in normotensive individuals and that non-dip** was higher, with diminished decline in nocturnal BPs, in subjects with masked hypertension. These findings may help to explain the reports of higher cardiovascular risk in patients with white-coat hypertension and the poor prognosis observed in patients with masked hypertension, highlighting the clinical diagnostic and prognostic utility of ABPM. Future research should evaluate the causal relationship between ambulatory BP variability and white-coat hypertension and between diminished nocturnal decreases in BP and masked hypertension.
References
Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F . ESH/ESC Guidelines for the management of arterial hypertension. The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013; 31: 1281–1357.
O'Brien E, Parati G, Stergiou G, Asmar R, Beilin L, Bilo G, Clement D, de laSierra A, de Leeuw P, Dolan E, Fagard R, Graves J, Head GA, Imai Y, Kario K, Lurbe E, Mallion JM, Mancia G, Mengden T, Myers M, Ogedegbe G, Ohkubo T, Omboni S, Palatini P, Redon J, Ruilope LM, Shennan A, Staessen JA, vanMontfrans G, Verdecchia P, Waeber B, Wang J, Zanchetti A, Zhang Y, European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens 2013; 31: 1731–1768.
Verdecchia P . Prognostic value of ambulatory blood pressure: current evidence and clinical implications. Hypertension 2000; 35: 844–851.
Conen D, Bamberg F . Noninvasive 24-h ambulatory blood pressure and cardiovascular disease: a systematic review and meta-analysis. J Hypertens 2008; 26: 1290–1299.
Mancia G . Short and long-term blood pressure variability: present and future. Hypertension 2012; 60: 512–517.
Stergiou GS, Parati G, Vlachopoulos C, Achimastos A, Andreadis E, Asmar R, Avolio A, Benetos A, Bilo G, Boubouchairopoulou N, Boutouyrie P, Castiglioni P, de la Sierra A, Dolan E, Head G, Imai Y, Kario K, Kollias A, Kotsis V, Manios E, McManus R, Mengden T, Mihailidou A, Myers M, Niiranen T, Ochoa JE, Ohkubo T, Omboni S, Padfield P, Palatini P, Papaioannou TG, Protogerou A, Redon J, Verdecchia P, Wang J, Zanchetti A, Mancia G, O'Brien E . Methodology and technology for peripheral and central blood pressure and blood pressure variability measurement: current status and future directions – Position statement of the European Society of Hypertension Working Group on blood pressure monitoring and cardiovascular variability. J Hypertens 2016; 34: 1665–1677.
Frattola A, Parati G, Cuspidi C, Albini F, Mancia G . Prognostic value of 24-hour blood pressure variability. J Hypertens 1993; 11: 1133–1137.
Sander D, Kukla C, Klingelhöfer J, Winbeck K, Conrad B . Relationship between circadian blood pressure patterns and progression of early carotid atherosclerosis: a 3-year follow-up study. Circulation 2000; 102: 1536–1541.
Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G . Relationship of 24-hour blood pressure mean and variability to severity of target-organ damage in hypertension. J Hypertens 1987; 5: 93–98.
Pierdomenico SD, Di Nicola M, Esposito AL, Di Mascio R, Ballone E, Lapenna D, Cuccurullo F . Prognostic value of different indices of blood pressure variability in hypertensive patients. Am J Hypertens 2009; 22: 842–847.
Kikuya M, Hozawa A, Ohkubo T, Tsuji I, Michimata, Matsubara M, Ota M, Nagai K, Araki T, Satoh H, Ito S, Hisamichi S, Imai Y . Prognostic significance of blood pressure and heart rate variabilities: the Ohasama Study. Hypertension 2000; 36: 901–906.
Mancia G, Parati G, Hennig M, Flatau B, Omboni S, Glavina F, Costa B, Scherz R, Bond G, Zanchetti A, ELSA Investigators. Relation between blood pressure variability and carotid artery damage in hypertension: baseline data from the European Lacidipine Study on Atherosclerosis (ELSA). J Hypertens 2001; 19: 1981–1989.
Pringle E, Phillips C, Thijs L, Davidson C, Staessen JA, de Leeuw PW, Jaaskivi M, Nachev C, Parati G, O’Brien ET, Tuomilehto J, Webster J, Bulpitt CJ, Fagard RH, Syst-Eur Investigators. Systolic blood pressure variability as a risk factor for stroke and cardiovascular mortality in the elderly hypertensive population. J Hypertens 2003; 21: 2251–2257.
Dawson SL, Manktelow BN, Robinson TG, Panerai RB, Potter JF . Which parameters of beat-to-beat blood pressure and variability best predict early outcome after acute ischemic stroke? Stroke 2000; 31: 463–468.
Verdecchia P, Angeli F, Gattobigio R, Rapicetta C, Reboldi G . Impact of blood pressure variability on cardiac and cerebrovascular complications in hypertension. Am J Hypertens 2007; 20: 154–161.
Mancia G, Bombelli M, Facchetti R, Madotto F, Corrao G, Trevano FQ, Grassi G, Sega R . Long-term prognostic value of blood pressure variability in the general population: results of the Pressioni Arteriose Monitorate e Loro Associazioni Study. Hypertension 2007; 49: 1265–1270.
Palatini P, Reboldi G, Beilin LJ, Casiglia E, Eguchi K, Imai Y, Kario K, Ohkubo T, Pierdomenico SD, Schwartz JE, Wing L, Verdecchia P . Added predictive value of night-time blood pressure variability for cardiovascular events and mortality: the Ambulatory Blood Pressure-International Study. Hypertension 2014; 64: 487–493.
Hansen TW, Thijs L, Li Y, Boggia J, Kikuya M, Björklund-Bodegård K, Richart T, Ohkubo T, Jeppesen J, Torp-Pedersen C, Dolan E, Kuznetsova T, Stolarz-Skrzypek K, Tikhonoff V, Malyutina S, Casiglia E, Nikitin Y, Lind L, Sandoya E, Kawecka-Jaszcz K, Imai Y, Wang J, Ibsen H, O'Brien E, Staessen JA, International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes Investigators. Prognostic value of reading-to-reading blood pressure variability over 24 hours in 8938 subjects from 11 populations. Hypertension 2010; 55: 1049–1057.
Kario K . Prognosis in relation to blood pressure variability: pro side of the argument. Hypertension 2015; 65: 1163–1169.
Asayama K, Wei FF, Hara A, Hansen TW, Li Y, Staessen JA . Prognosis in relation to blood pressure variability: con side of the argument. Hypertension 2015; 65: 1170–1179.
Ohkubo T, Hozawa A, Yamaguchi J, Kikuya M, Ohmori K, Michimata M, Matsubara M, Hashimoto J, Hoshi H, Araki T, Tsuji I, Satoh H, Hisamichi S, Imai Y . Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: the Ohasama study. J Hypertens 2002; 20: 2183–2189.
ABC-H Investigators ABC-H Investigators Roush GC ABC-H Investigators Fagard RH ABC-H Investigators Salles GF ABC-H Investigators Pierdomenico SD ABC-H Investigators Reboldi G ABC-H Investigators Verdecchia P ABC-H Investigators Eguchi K ABC-H Investigators Kario K ABC-H Investigators Hoshide S ABC-H Investigators Polonia J ABC-H Investigators de la Sierra A ABC-H Investigators Hermida RC ABC-H Investigators Dolan E ABC-H Investigators Zamalloa H . Prognostic impact from clinic, daytime, and night-time systolic blood pressure in nine cohorts of 13,844 patients with hypertension. J Hypertens 2014; 32: 2332–2340.
Fagard RH, Celis H, Thijs L, Staessen JA, Clement DL, De Buyzere ML, De Bacquer DA . Daytime and nighttime blood pressure as predictors of death and cause-specific cardiovascular events in hypertension. Hypertension 2008; 51: 55–61.
Boggia J, Li Y, Thijs L, Hansen TW, Kikuya M, Bjorklund-Bodegard K, Richart T, Ohkubo T, Kuznetsova T, Torp-Pedersen C, Lind L, Ibsen H, Imai Y, Wang J, Sandoya E, O’Brien E, Staessen JA . Prognostic accuracy of day versus night ambulatory blood pressure: a cohort study. Lancet 2007; 370: 1219–1229.
Ohkubo T, Imai Y, Tsuji I, Nagai K, Watanabe N, Minami N, Kato J, Kikuchi N, Nishiyama A, Aihara A, Sekino M, Satoh H, Hisamichi S . Relation between nocturnal decline in blood pressure and mortality: the Ohasama Study. Am J Hypertens 1997; 10: 1201–1207.
de la Sierra A, Redon J, Banegas JR, Segura J, Parati G, Gorostidi M, de la Cruz JJ, Sobrino J, Llisterri JL, Alonso J, Vinyoles E, Pallarés V, Sarria A, Aranda P, Ruilope LM Spanish Society of Hypertension Ambulatory Blood Pressure Monitoring Registry Investigators. Prevalence and factors associated with circadian blood pressure patterns in hypertensive patients. Hypertension 2009; 53: 466–472.
Cacciolati C, Tzourio C, Hanon O . Blood pressure variability in elderly persons with white-coat and masked hypertension compared to those with normotension and sustained hypertension. Am J Hypertens 2013; 26: 367–372.
Cahan A, Ben-Dov IZ, Mekler J, Bursztyn M . The role of blood pressure variability in misdiagnosed clinic hypertension. Hypertens Res 2011; 34: 187–192.
Rodríguez-Artalejo F, Graciani A, Guallar-Castillón P, León-Muñoz LM, Zuluaga MC, López-García E, Gutiérrez-Fisac JL, Taboada JM, Aguilera MT, Regidor E, Villar-Álvarez F, Banegas JR . Rationale and methods of the study on nutrition and cardiovascular risk in Spain (ENRICA). Rev Esp Cardiol 2011; 64: 876–882.
Banegas JR, de la Cruz JJ, Graciani A, López-García E, Gijón-Conde T, Ruilope LM, Rodriguez-Artalejo F . Impact of Ambulatory Blood Pressure Monitoring on reclassification of hypertension prevalence and control in older people in Spain. J Clin Hypertens (Greenwich) 2015; 17: 453–461.
Ragazzo F, Saladini F, Palatini P . Validation of the Microlife WatchBP O3 device for clinic, home, and ambulatory blood pressure measurement, according to the International Protocol. Blood Press Monit 2010; 15: 59–62.
Parati G, Stergiou G, O'Brien E, Asmar R, Beilin L, Bilo G, Clement D, de la Sierra A, de Leeuw P, Dolan E, Fagard R, Graves J, Head GA, Imai Y, Kario K, Lurbe E, Mallion JM, Mancia G, Mengden T, Myers M, Ogedegbe G, Ohkubo T, Omboni S, Palatini P, Redon J, Ruilope LM, Shennan A, Staessen JA, van Montfrans G, Verdecchia P, Waeber B, Wang J, Zanchetti A, Zhang Y European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. European Society of Hypertension practice guidelines for ambulatory blood pressure monitoring. J Hypertens 2014; 32: 1359–1366.
Mancia G, Facchetti R, Grassi G, Bombelli M . Adverse prognostic value of persistent office blood pressure elevation in white coat hypertension. Hypertension 2015; 66: 437–444.
Fagard RH, Cornelissen VA . Incidence of cardiovascular events in white-coat masked and sustained hypertension versus true normotension: a meta-analysis. J Hypertens 2007; 25: 2193–2198.
Briasoulis A, Androulakis E, Palla M, Papageorgiou N, Tousoulis D . White-coat hypertension and cardiovascular events: a meta-analysis. J Hypertens 2016; 34: 593–599.
Gorostidi M, Vinyoles E, Banegas JR, de la Sierra A . Prevalence of white-coat and masked hypertension in national and international registries. Hypertens Res 2015; 38: 1–7.
Asayama K, Thijs L, Li Y, Gu YM, Hara A, Liu YP, Zhang Z, Wei FF, Lujambio I, Mena LJ, Boggia J, Hansen TW, Björklund-Bodegård K, Nomura K, Ohkubo T, Jeppesen J, Torp-Pedersen C, Dolan E, Stolarz-Skrzypek K, Malyutina S, Casiglia E, NikitinY, Lind L, Luzardo L, Kawecka-Jaszcz K, Sandoya E, Filipovský J, Maestre GE, Wang J, Imai Y, Franklin SS, O'Brien E, Staessen JA International Database onAmbulatory Blood Pressure in Relation to Cardiovascular Outcomes (IDACO)Investigators. Setting thresholds to varying blood pressure monitoring intervals differentially affects risk estimates associated with white-coat and masked hypertension in the population. Hypertension 2014; 64: 935–942.
Polónia J, Carvalho N, Barbosa L, Silva JA . Blood pressure on arising, morning blood pressure surge and blood pressure variability in white coat hypertensives and in matched normotensives and sustained hypertensives. Rev Port Cardiol 2006; 25: 693–704.
Kang IS, Pyun WB, Shin J, Ihm SH, Kim JH, Park S, Kim KI, Kim WS, Kim SG, Shin GJ . Higher blood pressure variability in white coat hypertension; from the Korean Ambulatory Blood Pressure Monitoring Registry. Korean Circ J 2016; 46: 365–373.
Clement DL, Mussche MM, Vanhoutte G, Pannier R . Is blood pressure variability related to activity of the sympathetic system? Clin Sci (Lond) 1979; 57: 217s–219s.
Hänninen MR, Niiranen TJ, Puukka PJ, Kesäniemi YA, Kähönen M, Jula AM . Target organ damage and masked hypertension in the general population:the Finn-Home study. J Hypertens 2013; 31: 1136–1143.
Pierdomenico SD, Cuccurullo F . Prognostic value of white-coat and masked hypertension diagnosed by ambulatory monitoring in initially untreated subjects: an updated meta-analysis. Am J Hypertens 2011; 24: 52–58.
Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, Den Hond E, McCormack P, Staessen JA, O'Brien E . Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study. Hypertension 2005; 46: 156–161.
Redon J, Lurbe E . Nocturnal blood pressure versus non dip** pattern: what do they mean? Hypertension 2008; 51: 41–42.
Kayano H, Koba S, Matsui T, Fukuoka H, Kaneko K, Shoji M, Toshida T, Watanabe N, Geshi E, Kobayashi Y . Impact of depression on masked hypertension and variability in home blood pressure in treated hypertensive patients. Hypertens Res 2015; 38: 751–757.
Mancia G, Facchetti R, Bombelli M, Grassi G, Sega R . Long-term risk of mortality associated with selective and combined elevation in office, home, and ambulatory blood pressure. Hypertension 2006; 47: 846–853.
Fan HQ, Li Y, Thijs L, Hansen TW, Boggia J, Kikuya M, Björklund-Bodegård K, Richart T, Ohkubo T, Jeppesen J, Torp-Pedersen C, Dolan E, Kuznetsova T, Stolarz-Skrzypek K, Tikhonoff V, Malyutina S, Casiglia E, Nikitin Y, Lind L, Sandoya E, Kawecka-Jaszcz K, Imai Y, Ibsen H, O'Brien E, Wang J, Staessen JA International Database on Ambulatory Blood Pressure In Relation to Cardiovascular Outcomes Investigators. Prognostic value of isolated nocturnal hypertension on ambulatory measurement in 8711 individuals from 10 populations. J Hypertens 2010; 28: 2036–2045.
Verdecchia P, Schillaci G, Guerrieri M, Gatteschi C, Benemio G, Boldrini F, Porcellati C . Circadian blood pressure changes and left ventricular hypertrophy in essential hypertension. Circulation 1990; 81: 528–536.
Salles GF, Reboldi G, Fagard RH, Cardoso CR, Pierdomenico SD, Verdecchia P, Eguchi K, Kario K, Hoshide S, Polonia J, de la Sierra A, Hermida RC, Dolan E, O'Brien E, Roush GC ABC-H Investigators. Prognostic effect of the nocturnal blood pressure fall in hypertensive patients: the ambulatory blood pressure collaboration in patients with hypertension (ABC-H) meta-analysis. Hypertension 2016; 67: 693–700.
Kawano Y, Horio T, Matayoshi T, Kamide K . Masked hypertension: subtypes and target organ damage. Clin Exp Hypertens 2008; 30: 289–296.
Castiglioni P, Parati G, Brambilla L, Brambilla V, Gualerzi M, Di Rienzo M, Coruzzi P . Detecting sodium-sensitivity in hypertensive patients: information from 24-hour ambulatory blood pressure monitoring. Hypertension 2011; 57: 180–185.
Schutte R, Thijs L, Liu YP, Asayama K, ** Y, Odili A, Gu YM, Kuznetsova T, Jacobs L, Staessen JA . Within-subject blood pressure level—not variability—predicts fatal and nonfatal outcomes in a general population. Hypertension 2012; 60: 1138–1147.
Acknowledgements
This study is partially funded by FIS grants PI13/02321 and PI16/01460 (Instituto de Salud Carlos III and FEDER/FSE) and CIBERESP.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Gijón-Conde, T., Graciani, A., López-García, E. et al. Short-term variability and nocturnal decline in ambulatory blood pressure in normotension, white-coat hypertension, masked hypertension and sustained hypertension: a population-based study of older individuals in Spain. Hypertens Res 40, 613–619 (2017). https://doi.org/10.1038/hr.2017.9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2017.9
- Springer Nature Singapore Pte Ltd.
Keywords
This article is cited by
-
Baroreflex failure and beat-to-beat blood pressure variation
Hypertension Research (2018)
-
Extent of, and variables associated with, blood pressure variability among older subjects
Aging Clinical and Experimental Research (2018)
-
Visit-to-visit blood pressure variability in children and adolescents with renal disease
Clinical and Experimental Nephrology (2018)