
Abstract
Background
Prior studies establish that Black neighborhoods and older persons experience higher rates of COVID-19 death than white neighborhoods and younger persons. However, such works point to the effect of age on COVID-19 mortality and the racial and ethnic inequalities present in COVID-19 deaths as independent vectors of inequality, neglecting to consider the multiplicative impact of structural conditions.
Methods
Using weekly ZIP code counts of deaths from March 2020 through July 2021 from the Chicago Department of Public Health (n = 4168) and measures of structural characteristics derived from the 5-year estimates of the 2019 American Community Survey, the current study examined how place, racial composition, and the age structure of communities act in tandem to shape the number of deaths due to COVID-19. We used STATA to estimate negative binomial models predictive of COVID-19 mortality.
Results
Findings from our statistical analysis revealed that in predominately Black neighborhoods, racial composition amplified the association of age structure (65 +) on COVID-19 mortality by 40%. Neighborhoods that were not predominately black did not show this multiplicative risk of death. Our findings underscore that the elevated risk of death in in older Black communities is attributed to historic and contemporary structural inequality.
Conclusions
Although society typically frames pandemics as natural disasters, doing such undermines dimensions of marginalization that amplify vulnerability among select populations. To begin eliminating such inequalities, the USA must deal with the entrenched limitations of institutions that render unequal attention and care to sectors of its population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Conventionally, pandemics are seen as unfortunate, seemingly unavoidable acts of nature that pose threats to human life. The COVID-19 pandemic is no exception. From March 2020 through November 1, 2021, the US population experienced almost 46 million infections and more than 745,000 deaths attributed to the coronavirus [1]. While framing disaster events as unavoidable acts of nature may be politically and institutionally beneficial, doing such inhibits a holistic understanding of how different populations experience them [2]. In other words, applying the conventional natural disaster paradigm undermines the political, institutional, and sociological dimensions of responses to such events that increase vulnerability in marginalized populations. For example, across the USA, data indicate that elderly and Black persons were substantially more likely to die as a result of COVID-19 infection than other racial and ethnic groups [3]. Within the city of Chicago, the nation’s third largest by population, Black persons account for roughly 41% of all COVID-19 deaths, and those aged 60 and over account for 79% of all COVID-19 deaths [4]. Pandemics, then, are events that exemplify the large racial disparities in mortality that characterize the USA [5].
The current pandemic is not the first disaster to demonstrate disparate health outcomes for older Black people. For example, in 1995, extremely hot weather engulfed much of the Midwestern USA, resulting in 739 heat-related deaths in the city of Chicago over a 7-day period [6]. The ratio of Black to white heat-related death rates was 1.5 for those aged 75–84 and 1.9 for those aged 85 and over, indicating that elderly Black residents had an elevated risk of mortality relative to white residents. Likewise, in 2005, Hurricane Katrina led to the deaths of about 1000 individuals across multiple southern states [7]. Again, the elderly and Black persons were more likely to die as a result of the storm than white persons. Such disparate death rates in the face of natural disaster are due to legacies of structural racism, which render Black communities socially, economically, and politically disadvantaged relative to white communities. In this sense, structural racism can be defined as the development and conceptual use of race as a mechanism by which to unevenly distribute resources via institutions, practices, and ideologies that adversely impact the health of Black communities [8, 9].
Predominately Black urban communities endure high levels of disadvantage that precipitate poor health outcomes and increased vulnerability to COVID-19 [10, 11]. The average Chicago ZIP code hot spot of COVID-19 infection rates has a population that is 83% non-Latinx Black, with 31% of residents living in poverty [12]. Further compounding the above deleterious conditions is that disenfranchised Black neighborhoods lack the political economy to advocate for better resources from local governments [13]. Amid the COVID-19 pandemic, racialized dynamics of labor and wealth collided to the detriment of Black neighborhoods because a large proportion of the non-medical essential workers are members of racially marginalized populations [14,15,16]. Those same populations were required to work without the personal protective equipment or regular screening afforded to those in the medical sector. In addition, disadvantaged communities are more reliant on public transit to commute to work [17]. Thus, the concentration of essential workers in impoverished Black communities is another lever that increases their exposure to COVID-19. Differential mortality rates by community racial makeup, thus, reflect the ways the pandemic inflamed existing health and socioeconomic inequalities.
The weathering hypothesis suggests that the Black lived experience increases one’s biological age beyond that of comparable adults of other ethnoracial groups [18]. Due to experiences with structural racism (e.g. residing in disadvantaged neighborhoods, experiencing housing discrimination, and general chronic strains), Black peoples’ bodies can be as much as 15 years older (biologically) than their chronological age [19, 20]. Thus, a Black person aged 70 may possess physiological conditions seen in white persons aged 85 and older. Additionally, racialized experiences in the aftermath of disaster events can yield stressors that result in aging. For example, in their study of Hurricane Katrina survivors, Adams and colleagues reported that the storm aged respondents through the accumulation of mental and physical ailments [21].
Not only do disaster events exploit the already vulnerable position of marginalized urban Black communities and increase the risk of death, but in periods of disaster, racism as a structural element is so pervasive that it intensifies other known risk factors of mortality. In the context of COVID-19, multiple studies descriptively demonstrate that both older and predominantly Black populations are at an elevated risk of death [14, 22, 23]. However, our work indicates that in older Black neighborhoods, the impact of advanced age on COVID-19 related death is amplified compared to predominantly white neighborhoods.
Variation in neighborhood COVID-19 mortality is not random, but dictated by centuries of structural inequality; thus, space is an important axis in the study of health inequality. Multiple studies demonstrate that the risk of COVID-19 transmission is unevenly distributed across geographies [24,25,26]. For this reason, we situate our research within the social ecological model which recognizes the importance of assessing contextual or neighborhood level conditions in the production of individual level health outcomes [27]. Such contextual conditions are predictive of place-based variation in health outcomes, including COVID-19 prevalence across neighborhoods [28]. An advantage of applying the social ecological model is that it allows for a more comprehensive understanding of the determinants of COVID-19 mortality. That is, our research inquiry is grounded in an interdisciplinary lens that incorporates public health, urban studies, sociology, and demography scholarship. In this study, we used ZIP code-level data from the Chicago Department of Public Health to examine how racial composition works in tandem with the local age structure to shape the number of COVID-19 deaths experienced in predominately Black communities. Our findings indicate that predominately Black neighborhoods experienced higher rates of COVID-19 mortality than their white counterparts, and that the composition of persons aged 65 and older exacerbated the number of deaths due to COVID-19 in predominately Black neighborhoods.
Methods
Data
We obtained mortality data from the COVID-19 Daily Cases, Deaths, and Hospitalizations database maintained by the Chicago Department of Public Health [4]. The dataset details weekly counts of deaths attributed to COVID-19 aggregated to the ZIP code level. The data span from March 1, 2020 through July 31, 2021 for a total of 74 weeks and are aggregated such that the week begins on Sunday and end on Saturday. The dependent variable for our analysis was the weekly count of COVID-19 deaths by ZIP code for each week. In total, our dataset included 4168 ZIP code-week observations.
We derived two other independent variables using the Chicago Department of Public Health data [4]. The ZIP code-week proportion of COVID-19 tests yielding positive results was included to control for the prevalence of the virus among the local population. We also included the cumulative proportion of completed COVID-19 vaccinations for ZIP codes by week. In our dataset, vaccination counts began the week of December 20, 2020.
To account for structural characteristics, we accessed sociodemographic data from the 5-year estimates of the American Community (ACS) for 2019 at the ZIP code tabulation area (ZCTA) level. We created a structural disadvantage index informed by Peterson and Krivo’s neighborhood-level sociological research, allowing us to account for the myriad ways by which structural racism facilitates health inequities across places [29]. Poverty is associated with negative health outcomes [30]. Furthermore, employment losses—often a precursor to poverty—during the pandemic were concentrated among Black/African American workers [31]. Considering that healthcare is partially covered in many occupations, the loss of employment elevated the risk of COVID-19 health complications in segregated Black neighborhoods. And of individuals that maintained employment through the pandemic, their risk of COVID-19 exposure may have been amplified if they worked in occupations where social distancing and/or remote work were options [32]. Both matters of poverty and employment are compounded in single-parent households where economic and child-rearing responsibilities rest solely on one adult [33]. Considering this knowledge, our additive index of structural disadvantage included the following z-scored proportion measures: unemployment, employment in professional (includes management and related) jobs, employment in secondary sector jobs,Footnote 1 college graduates, presence of single female-headed households with children under 18 years, and individuals living in poverty (Cronbach’s α = 0.935) [29]. We preferred this measure over others because it incorporates measures of employment industry, which is associated with COVID-19 infection.
We employed the classification scheme developed by Peterson and Krivo to racially characterize spaces [29]. Using dummy variables, we categorized ZIP codes as predominately Black (n = 13), non-Latinx white (n = 8), or LatinxFootnote 2 (n = 3) if 70% of residents identify as any of those racial/ethnic groups. Minority ZIP codes described ZIP codes where non-Latinx Black and Latinx white residents composed at least 70% of the population, without neither group alone composing more than 70% of the population (n = 7). We categorized all remaining ZIP codes as integrated (n = 28). Using this operationalization scheme, we estimated the impact of high levels of segregation on COVID-19 deaths.
Considering that age is a risk factor for mortality, we included the proportion of the population aged at least 65 years and the proportion of the population aged 75 and over as predictors [41]. Our measure of time ranged from zero to 73, where each unit increase represented a 1-week shift from the start date of the analysis.
Analysis
We estimated weekly COVID-19 ZIP code death rates, the dependent variable, using count panel models to account for correlated weekly death counts within spatial units, but also to adjust for the temporal ordering of observations [42]. Panel models account for time, but we also controlled for time in the model with a predictor that measured time in weeks. Examination of our outcome measure indicated that most ZIP code-weeks demonstrated comparatively low death counts, while a small cohort of observations included notably more death counts. Although Poisson regression can model rare phenomenon, the strict assumption of equidispersion renders it inapplicable here. Due to the overdispersed distribution of COVID-19 deaths (mean = 1.646, variance = 7.524), we utilized a series of negative binomial models. All predictors except for time and the ethnoracial composition variables were standardized to give a common scale such that we could assess the relative effects.
Because spatial autocorrelation can bias model estimates, we ran separate global Moran’s I analyses on ZIP code COVID-19 death rates for each week in the study period [43]. The average I value was 0.12, indicating weak yet positive spatial autocorrelation. In 30 out of 74 weeks, the level of clustering surpassed the odds of chance according to the P < 0.05 threshold. In response, we calculated the spatially lagged rate of COVID-19 mortality by week and entered that measure as a predictor in all inferential models [44]. This is the average mortality rate for each ZIP code’s adjacent ZIP codes, by week. We determined the adjacency of ZIP codes by using a first-order queen contiguity spatial weights matrix, whereby features are considered contiguous if they share a side or a vertex. We opted against distance-based weights because they require the use of an arbitrary threshold distance by which to determine adjacency, and due to substantial variation in ZIP code area (mean = 3.80 square miles, standard deviation = 3.02 square miles). While the smallest ZIP codes are less than 1 square mile, the largest three are greater than 10 square miles. Both the Moran’s I analysis and the spatial lag measure procedures were conducted using GeoDa spatial statistics software.
Results
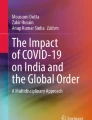
Figure 1 displays a map of Chicago ZIP codes by racial/ethnic categorization. The major sections of the city are indicated by blue planning district boundaries, provided by the Department of Planning and Development [35]. Chicago is the 3rd largest city in the USA with a population of 2,699,347 as of 2020. Thirty-three percent of residents identify as non-Latinx white, 29% as Black or African American, and 25% as Hispanic or Latinx [36]. According to the Othering & Belonging Institute at the University of California Berkeley, Chicago ranks as the 4th most segregated city in the country [37]. Fig. 1 aligns with that finding, as predominately White ZIP codes are clustered in the Northwest, North, and within and near the Central (Downtown) planning districts. Predominately Black ZIP codes are concentrated in the Southeast, Far South, and West planning districts. Health scholars have consistently noted that such segregation patterns are linked to health disparities in Black neighborhoods such as limited access to COVID-19 testing [38], elevated risk of COVID-19 infection [39], and increased likelihood of COVID-19-related death [40].

Racial/ethnic composition of Chicago ZIP codes
Table 1 includes unstandardized descriptive statistics of variables stratified by the racial characterization of the ZIP code. Recall, ZIP codes were classified as predominately Black, predominately Latinx, predominately white, minority, and integrated. The mean death rate ranged from 1.9 per 100,000 (predominately white neighborhoods) to 3.4 per 100,000 (predominately Black and Latinx neighborhoods). In addition, this table includes means for the positivity rate, completed vaccination rate, proportion of the ZIP code at least 65 years old, and the ethnoracial composition. In general, predominately Black ZIP codes had a lower proportion of completed vaccinations and were older compared to other types of ZIP codes; however, the mean proportion of positive cases COVID-19 was relatively low. Thus, despite their low mean positivity rate, their mean death rate was high.
Table 2 presents the results of negative binominal panel models predicting ZIP code-week COVID-19 mortality. In model 1, the spatial lag effect indicates that each unit increase in the averaged death counts of each ZIP code’s adjacent ZIP codes is associated with a 50% increase in focal ZIP code death rates (IRR = 1.503, P = 0.000). Additionally, there is a significant and positive effect of the proportion of positive COVID-19 tests on deaths (IRR = 1.288, P = 0.000). Thus, in line with existing epidemiological knowledge, the greater the prevalence of the virus in the population, the greater the local weekly death rate. Age structure also predicted death. Specifically, for each unit increase in the proportion of residents aged 65 and older, death counts increased by about 17% (IRR = 1.165, P = 0.001). On the other hand, each unit increase in the proportion of completed vaccinations was associated with a 39% reduction in COVID-19 deaths in the average ZIP code, in the average week of the time series. Structural disadvantage, on the other hand, was predictive of increased mortality (IRR = 1.132, P = 0.01).
In model 2, we included measures that characterize the racial makeup of the ZIP codes. While these measures were not significant and the coefficient for structural disadvantage was no longer statistically significant, the coefficient for age composition remained significant and increased (from IRR = 1.165 to IRR = 1.217, P = 0.000). In model 3, we introduced one interaction term that reveals that the impact of living in racially segregated areas on mortality was conditioned by local age composition in predominately Black areas. The interaction between predominately Black ZIP codes and retirement aged populations (65 +) amplified the influence of ZIP code age composition (% of residents 65 and older) on mortality by 40% (IRR = 1.369, P = 0.014). This association remained even when controlling for time, nearby mortality, the rate of vaccinations, and structural disadvantage. In addition, structural disadvantage was significant in this model, predictive of increased mortality (IRR = 1.275; P = 0.016).
Figure 2 displays the predicted margins of this interaction effect. Graphically, it reveals that there is a slight positive impact of aging on COVID-19 death counts in white ZIP codes. But in Black ZIP codes, the impact of aging on mortality is positive and curvilinear. While the purpose of displaying this figure is to point to the different trends broadly, it is also worth noting that when the proportion of residents aged 65 and over is less than 15%, Black ZIP codes appear to have a slightly lower death rate. While we do not want to extrapolate too much because this figure is based on predictive values, one possible explanation involves social cohesion (strength of relationships and unity among members of the neighborhood) and institutional support [45]. Perhaps, when the 65 + population is low enough, the social cohesion present in Black ZIP codes is enough for the predicted deaths to be lower. However, once the threshold is crossed, social cohesion alone is not enough, and this is where we see the importance of institutional support and access to resources.

Interaction effect of race * age composition
We considered whether the relationship between age and racial composition was robust by trying a different age ceiling. In model 4, we included the interaction effect of predominately Black ZIP codes with the proportion of residents aged 75 and older. The effect was consistent in magnitude and significance (Black * percentage aged 75 + IRR = 1.403, P = 0.011). In models not shown, we explored if such a relationship existed in spaces that were not predominately Black. Our findings indicate that the racial composition and age composition interaction that amplifies mortality is one that is exclusive to predominately Black ZIP codes.
Discussion and Conclusion
The novel finding of the study is that in predominately Black neighborhoods, the insidious environment created by segregation is unique and amplified the effect of age composition on COVID-19 mortality. Theoretically, these findings can be interpreted in light of Klinenberg’s research finding that structural inequality is exacerbated in times of disaster [2]. Considering his earlier studies of the Chicago heat wave, the differential survival rates for structurally disadvantaged, older Black communities compared to white communities are not only unsurprising, but predictable.
Sociological studies have long documented that urban Black communities endure levels of disadvantage that far exceed that of white communities, and that they are more racially segregated than Latinx communities. Furthermore, Black persons are more likely to be hourly wage essential workers; Black communities endure social and environmental threats and continually deal with the failures of social institutions (e.g., reduced access to homeownership, quality education, familial stability, and concentrated poverty). Given this high level of concentrated disadvantage, one might posit that there must be a point when increased inequality does not matter. However, the entrance of the COVID-19 pandemic lowered the life expectancy of the non-Latinx Black population by 2.7 years based on estimates between January and June 2020, while the white population’s life expectancy declined by 0.8 years [46]. The disproportionate impact is undeniable.
In addition, the Black lived experience—characterized in part by structural and institutional racial discrimination—is physiologically consequential. This occurs through the biological aging of Black persons beyond their physical age in response to racism. As a result, elderly Black persons represent a vulnerable group that concentrates health conditions associated with COVID-19 mortality more so than similarly situated white communities. Therefore, the barriers that elderly Black communities face occur in addition to those that are conventionally associated with aging. Matters of physical mobility, social isolation, and fear are likely compounded for elderly Black persons that reside in communities with defunct or absent social institutions. Thus, the findings here speak to the potential harm posed by accelerated aging or weathering experienced by Blacks born prior to 1966, whose parents and grandparents came of age when sharecrop** and Jim Crow were still fixtures in the south. Even as the twentieth century came to a close, there remained ample evidence that systemic racism enabled the continued oppression of Blacks via space [47].
Our findings also highlight the diffuse spatial effects of COVID-19 mortality. That is, the mere location of a ZIP code adjacent to a high mortality ZIP code is associated with increased COVID-19 deaths, and prior research confirms that high COVID-19 mortality communities in Chicago are overwhelmingly composed of Black residents [12]. This suggests that Black residents not only endure a high risk of exposure within their own communities, but that the spatially clustered nature of segregated Black communities ensures that such risk remains high when traversing through neighboring communities as well. Differences in spatial isolation and the concentration of disadvantage may account for why predominately Latinx and minority ZIP codes did not demonstrate elevated levels of mortality associated with Black ZIP codes [29]. Simply put, predominately Latinx neighborhoods are not as racially segregated, nor do they possess the levels of concentrated structural disadvantage documented in Black neighborhoods [2]. These differential structural conditions may account for why Latinx persons are less likely than Black persons to die of COVID-19 [48].
Pandemics, by definition, require global actions. They also require the health infrastructure within a nation to deal with shortcomings that leave some populations without any protections. Our findings indicate that predominately Black communities with high proportions of elderly persons experienced significantly more deaths than other communities. Although attitudes towards receiving the vaccine have changed in the Black population, the neighborhoods of racially marginalized populations are less likely to receive the vaccine due to “vaccine deserts,” hesitancy towards a medical treatment that has no liability due to its emergency nature, and distrust of medical institutions in part due to the long history of abuse, discrimination, and unethical practices of such populations in the research and practice of medicine [34, 49]. This is an uphill battle, but it is not a new one. The medical community has yet to give the Black population, particularly older Black persons, the respect and attention needed to mend the distrust warranted towards it. Reaching out to predominately Black neighborhoods and finding a space to answer residents’ questions regarding the virus and the vaccination have led to increased awareness of ways to protect one’s self, friends, and family from acquiring COVID-19 and led to more vaccinations [46, 50, 51]. If members of the medical community do respectfully listen and respond in empathic ways not typical to doctor-patient interactions in the Black community, the trust built may extend beyond the pandemic. In sum, the pandemic provides an opportunity to construct positive relationships between medical institutions and the Black population.
However, the results of this study implicate institutions beyond medicine and point to the social structure of society that permit racism to permeate via our social institutions. At the beginning of 2021, COVID-19 continued to disproportionately, adversely affect the Black population. The president of the NAACP noted that protests at state capitals and other cities around the country demanding that life resume to normal from largely white crowds did not happen until the “less affected” white people learned of the difference in COVID-19 mortality by race and ethnicity [51]. Indeed, the timing of such protests did coincide with this information. Such racial data, though, is important because the US is a racialized country, and knowledge of such disparities theoretically helps scholars, physicians, and policy-makers to target efforts to ameliorate inequality. Yet, the public knowledge of the differential impact of COVID-19 on marginalized groups also reflected the racism still very much present in the USA. It exposed how much work remains for not only the institutions including medicine, education, labor, and housing, but also for the people inhabiting the nation.
This study has some limitations. First, due to the modifiable areal unit problem, the use of aggregate ZIP code data may have shrouded variation in COVID-19 fatalities that occurred at smaller spatial units. Nonetheless, previous COVID-19 studies have recognized ZIP codes as a suitable unit of analysis [52]. Furthermore, such variation does not negate the context of segregated spaces, where Black segregated spaces experience a lack of resources compared to non-Latinx white and Latinx spaces [34]. Second, we utilized test positivity rates to give a sense of the level of COVID-19 infection in spaces. However, our data do not allow us to distinguish between symptomatic and routine testing. Some spaces, such as university settings, required students and employees to test regularly, and this is different than voluntary testing or testing that took place in hospital settings. Additionally, our data do not include institutionalized populations. The COVID-19 pandemic certainly affected persons housed in jails or prisons differently given the limited amount of protective resources and the inability to socially distance and quarantine individuals infected with COVID-19. Nevertheless, such limitations do not take away the value of the core finding — the COVID-19 death rate curve for predominately Black communities is curvilinear and positive, reflecting the political, institutional, and social shortcomings within US society.
Given the level of disadvantage experienced by Black people, who largely live in segregated neighborhoods, it will take sustained and substantial investment to begin to make a difference. Those investments, however, must contend with the momentum of hundreds of years of structural racism. That the racial makeup of neighborhoods wields statistical influence on the general relationship between mortality and aging, a well-established risk factor for multiple health outcomes, speaks to the pervasiveness of racism in American society. However, it also demonstrates how older Black communities are disadvantaged on so many fronts encapsulated by racism, which ultimately increases their likelihood of death due to exposure and contraction of COVID-19. COVID-19, then, is not a special situation; rather, it provides yet another opportunity to expose the pervasiveness of racism in the USA.
Notes
Proportion of the employed population working in health care support, food preparation and serving-related occupations, building and grounds cleaning and maintenance, personal care and service, farming, fishing, moving, and material moving jobs.
Latinx does not include Latinix Black. Latinx Black are included in the Black racial group.
References
Johns Hopkins University & Medicine. Coronavirus Resource Center. 2021 [cited 2021 October 10]; Available from: https://coronavirus.jhu.edu.
Klinenberg E. Denaturalizing disaster: a social autopsy of the 1995 Chicago heat wave. Theory Soc. 1999;28:239–95.
Thebault, R., A.B. Tran, and V. Williams, The coronavirus is infecting and killing Black Americans at an alarmingly high rate, in The Washington Post. 2020: Washington, DC.
Chicago Data Portal. COVID-19 daily cases, deaths, and hospitalizations. 2021 [cited 2021 February 10]; Available from: https://data.cityofchicago.org/Health-Human-Services/COVID-19-Daily-Cases-Deaths-and-Hospitalizations/naz8-j4nc.
National Center for Health Statistics, Health, United States. 2019, U.S. Department of Health and Human Services: Hyattsville, MD.
Whitman S, et al. Mortality in Chicago attributed to the July 1995 heat wave. Am J Public Health. 1997;87(9):1515–8.
Brunkard J, Namulanda G, Ratard R. Hurricane Katrina deaths, Louisiana, 2005. Disaster Med Public Health Prep. 2008;2(4):215–23.
Gee GC, Ford CL. Structural racism and health inequities: old issues, new directions. Du Bois Rev. 2011;8(1):115–32.
Ray V. A theory of racialized organizations. Am Sociol Rev. 2019;84(1):26–53.
Williams DR, Collins C. Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Rep. 2001;116:404–16.
Kim SJ, Bostwick W. Social vulnerability and racial inequality in COVID-19 deaths in Chicago. Health Educ Behav. 2020;47(4):509–13.
Maroko AR, Nash D, Pavilonis BT. COVID-19 and inequity: a comparative spatial analysis of New York City and Chicago hot spots. J Urban Health. 2020;97:461–70.
Nandi A, et al. What explains the association between neighborhood-level income inequality and the risk of fatal overdose in New York City? Soc Sci Med. 2006;63(3):662–74.
Lee IJ, Ahmed NU. The devastating cost of racial and ethnic health inequality in the COVID-19 pandemic. J Natl Med Assoc. 2021;113(1):14–117.
Zimring, C.A., Clean and white: a history of environmental racism in the United States. 2015: New York University Press.
Rogers TN, et al. Racial disparities in COVID-19 mortality among essential workers in the United States. World Med Health Policy. 2020;12(3):311–27.
Pathak R, Wyczalkowski CK, Huang X. Public transit access and the changing spatial distribution of poverty. Reg Sci Urban Econ. 2017;66:198–212.
Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis. 1992;2(3):207–21.
Simons, R.L., et al., The effects of social adversity, discrimination, and health risk behaviors on the accelerated aging of African Americans: further support for the weathering hypothesis. Social Science & Medicine, 2021. 282.
Geronimus AT, et al. Do U.S. Black women experience stress-related accelerated biological aging? Human Nat. 2010;21:19–38.
Adams V, et al. Aging Disaster: Mortality, vulnerability, and long-term recovery among Katrina survivors. Med Anthropol. 2011;30(3):247–70.
Yadaw AS, et al. Clinical features of COVID-19 mortality: development and validation of a clinical prediction model. Lancet Digital Health. 2020;2(10):e516–25.
McLaughlin JM, et al. County-level predictors of coronavirus disease 2019 (COVID-19) cases and deaths in the United States: what happened, and where do we go from here? Clin Infect Dis. 2021;73(7):e1814–21.
Han Y, et al. Spatial distribution characteristics of the COVID-19 pandemic in Bei**g and its relationship with environmental factors. Sci Total Environ. 2021;761:144257.
Martellucci CA, et al. Changes in the spatial distribution of COVID-19 incidence in Italy using GIS-based maps. Ann Clin Microbiol Antimicrob. 2020;19(1):30.
Elson R, et al. The spatio-temporal distribution of COVID-19 infection in England between January and June 2020. Epidemiol Infect. 2021;149:e73.
Skokols D. Translating social ecological theory into guidelines for community health promotion. Am J Health Promot. 1996;10(4):282–98.
Vitale M. The social ecology of COVID-19 prevalence and risk in Montreal, QC. Can Health Place. 2022;78:102919.
Peterson RD, Krivo LJ, Divergent social worlds: neighborhood crime and the racial-spatial divide. Rose Series in Sociology. New York. NY: Sage; 2010.
Keith-Jennings B, Llobrera J, Dean S. Links of the supplemental nutrition assistance program with food insecurity, poverty, and health: evidence and potential. Am J Public Health. 2019;109(12):1631–77.
Gemelas J, et al. Inequities in employment by race, ethnicity, and sector during COVID-19. J Racial Ethn Health Disparities. 2022;9(1):350–5.
Baker, M., T.K. Peckham, and N.S. Seixas, Estimating the burden of United States workers exposed to infection or disease: a key factor in containing risk of COVID-19 infection. PLOS One, 2020. 15(4).
Hertz R, Mattes J, Shook A. When paid work invades the family: Single mothers in the COVID-19 pandemic. J Fam Issues. 2021;42(9):2019–45.
Satcher LA. Multiply-deserted areas: environmental racism and food, pharmacy, and greenspace access in the urban South. Environ Sociol. 2022;8(3):279–91.
Chicago Data Portal. Boundaries - planning regions. 2022 [cited 2022 October 5]; Available from: https://data.cityofchicago.org/Community-Economic-Development/Boundaries-Planning-Regions/spyv-p8fk.
U.S. Census Bureau. 2020 5-year American Community Survey. 2021.
Othering & Belonging Institute. Most to least segregated cities. 2022 [cited 2022 October 1]; Available from: https://belonging.berkeley.edu/most-least-segregated-cities.
Asabor EN, Warren JL, Cohen T. Racial/ethnic segregation and access to COVID-19 testing: spatial distribution of COVID-19 testing sites in the four largest highly segregated citieS in the United States. Am J Public Health. 2022;112(3):518–26.
Tung EL, et al. Association of neighborhood disadvantage with racial disparities in COVID-19 positivity in Chicago. Health Aff. 2021;40(11):1787–91.
Pierce JB, et al. Racial/ethnic minority and neighborhood disadvantage leads to disproportionate mortality burden and years of potential life lost due to COVID-19 in Chicago. Illinois Health & Place. 2021;68:102540.
Centers for Disease Control and Prevention. Older adults at greater risk of requiring hospitalization or dying if diagnosed with COVID-19. 2020 December 13, 2020 [cited 2021 February 8]; Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html.
Hilbe, J.M., Negative binomial regression. 2nd ed. 2011, Cambridge, UK: Cambridge University Press.
Jennings JM, et al. Neighborhood alcohol outlets and the association with violent crime in one Mid-Atlantic city: the implications for zoning policy. J Urban Health. 2014;91(1):62–71.
Marotta P. Assessing spatial relationships between rates of crime and rates of gonorrhea and chlamydia in Chicago, 2012. J Urban Health. 2017;94:276–88.
Kawachi I, Berkman L. Social cohesion, social capital and health. Soc Epidemiol. 2000;174(7):290–319.
Arias, E., B. Tejada-Vera, and F. Ahmad, Provisional life expectancy estimates for January through June 2020, N.C.f.H. Statistics, Editor. 2021, Centers for Disease Control and Prevention.
Massey DS, Categorically unequal: the American stratification system. New York. NY: Russell Sage Foundation; 2007.
Renelus BD, et al. Racial disparities in COVID-19 hospitalization and in-hospital mortality at the height of the New York City pandemic. J Racial Ethn Health Disparities. 2021;8(5):1161–7.
Sharkey, P. and F. Elwert, The legacy of disadvantage: multigenerational neighborhood effects on cognitive ability. American Journal of Sociology, 2011. 116(6).
Massey, D.S. N.A. Denton, American Apartheid: segregation and the making of the underclass. Cambridge. MA: Harvard University Press; 1993.
Johnson, D. When it comes to Covid-19, another case of white flight. CNN 2020 May 11; Available from: https://www.cnn.com/2020/05/11/opinions/covid-19-case-white-flight-johnson/index.html.
Bilal U, et al. Spatial inequities in COVID-19 testing, positivity, confirmed cases, and mortality in 3 US cities: an ecological study. Ann Intern Med. 2021;174(7):936–44.
Author information
Authors and Affiliations
Contributions
The authors contributed equally to the manuscript. All the authors contributed to the study conception and design. Material preparation, data assembly, and analysis were performed by Lallen Johnson. The first draft of the manuscript was written by Evelyn Patterson, and all the authors commented on previous versions of the manuscript.
Corresponding author
Ethics declarations
Ethics Approval
Because the analysis involved the use of existing, publicly available data, it was exempt from IRB review as it does not fall under research involving human subjects.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Patterson, E.J., Johnson, L.T. Structural Inequality and COVID-19 Mortality in Chicago: An Ecological Analysis. J. Racial and Ethnic Health Disparities 10, 2620–2629 (2023). https://doi.org/10.1007/s40615-022-01440-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-022-01440-1