
Abstract
Purpose
To find out what is known from literature about Long COVID until January 30, 2021.
Methods
We undertook a four-step search with no language restriction. A preliminary search was made to identify the keywords. A search strategy of all electronic databases resulted in 66 eligible studies. A forward and backward search of the references and citations resulted in additional 54 publications. Non-English language articles were translated using Google Translate. We conducted our sco** review based on the PRISMA-ScR Checklist.
Results
Of 120 papers, we found only one randomized clinical trial. Of the 67 original studies, 22 were cohort, and 28 were cross-sectional studies. Of the total 120 publications, 49.1% focused on signs and symptoms, 23.3% on management, and 10.8% on pathophysiology. Ten publications focused on imaging studies. The results are also presented extensively in a narrative synthesis in separated sections (nomenclature, diagnosis, pathophysiology, risk factors, signs/symptoms, management).
Conclusions
The controversies in its definition have impaired proper recognition and management. The predominant symptoms were: fatigue, breathlessness, arthralgia, sleep difficulties, and chest pain. Recent reports also point to the risk of long-term sequela with cutaneous, respiratory, cardiovascular, musculoskeletal, mental health, neurologic, and renal involvement in those who survive the acute phase of the illness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Descriptions of long-lasting symptoms after influenza-like illnesses can be traced back to 1892 when Josephine Butler, a women’s right campaigner, wrote to her son complaining of unresolved fatigue after being infected with the Russian Influenza. In 1895, politicians in the United Kingdom, including the prime minister, who were infected with the Russian Influenza reflected in their periodicals and diaries about the long-lasting fatigue and insomnia [1]. More recent viral infections such as Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-1) and the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) have also been associated with unabating post-acute phase lingering symptoms. In a systematic review of prolonged symptoms of SARS-CoV-1 and MERS-CoV by Ahmed et al., approximately one-third of the patients suffered from prolonged anxiety, depression, and post-traumatic stress disorder (PTSD) up to 6 months after complete recovery from the acute illness [2]. Moreover, they found that 11–45% of the patients had diminished DLCO (diffusing capacity of the lungs for carbon monoxide) at one-year follow-up [2].
SARS-CoV-1 survivors have been reported to suffer from long-term pulmonary complications, such as impaired exercise capacity, reduced DLCO, and interstitial lung abnormalities [3]. Additionally, in long-term follow-up of 121 SARS-CoV-1 survivors, cardiovascular complications were quite common: hypotension (50.4%), tachycardia (71.9%), bradycardia (14.9%), and cardiomegaly (10.7%) [4]. Other long-term abnormalities associated with SARS-CoV-1 were persistent hyperlipidemia and derangements in glucose hemostasis [5]. While acute renal impairment [6], acute gastrointestinal effects [7], acute viral hepatitis [8], and acute diabetes mellitus from the binding of the virus to its receptors on pancreatic islets cells [9] were reported, the long term consequences were not mentioned. Moreover, hematologic abnormalities, such as lymphopenia, leukopenia, thrombocytopenia, prolonged activated partial thromboplastin time (aPTT), coagulopathy (elevated D-dimer) and disseminated intravascular coagulation (DIC), and a pro-thrombotic state at micro- and macro- vasculature involving both veins and arteries with thromboembolic complications have been observed in the acute phase of these viral infections with potential long term consequences [10, 11]. In regard to psychosocial manifestations, a considerable number of SARS-CoV-1 patients suffered from chronic widespread musculoskeletal pain, fatigue, psychological stress, and disturbed sleep, hindering their return to productive work for up to 2 years after acute illness [12, 13]. In their 1-year follow-up of the survivors, Tansey et al., reported that more than half of the patients still experienced fatigue and sleep disturbance [14]. The subject of post-acute COVID-19 was recently reviewed by Amenta et al. [15].
Similarly, in a study of recovered patients from MERS-CoV, abnormal chest radiographs with ground-glass opacities and pleural thickening, indicative of pulmonary fibrosis, were still present at a median of 43 days after discharge from the hospital [16]. Although both SARS-CoV-1 and MERS-CoV have been associated with neurologic sequela, the latter is believed to be more neuro-invasive, causing complications such as paralysis, ischemic stroke, Guillain–Barre syndrome, and neuropathy [10, 17].
Despite considerable concerns about the long-lasting symptoms of COVID-19, our collective understanding and approach to its management are still in their infancy. This sco** review elaborates upon the up-to-date knowledge regarding this so-called “Long COVID” and attempts to shed light on future needs in this area. Due to the diversity and yet relative paucity of evidence, conducting a conventional systematic review would be less beneficial; thus, we conducted a systematic sco** study on this topic to highlight the currently available literature and to identify gaps in our knowledge. We hope our effort would reveal areas that need immediate attention and guide future research efforts.
Our focus here is to synthesize what is known from literature about the persistent COVID-19, its signs and symptoms, its pathophysiology, and the current management recommendations. We also wish to highlight the gaps in our knowledge regarding ‘long COVID’ syndrome.
Method
Since the review question is comprehensive, we found the systematic sco** review as the most suitable methodology to answer the question. To achieve clarity and transparency and to avoid poor reporting, we used Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Sco** Reviews (PRISMA-ScR) [18].
Review question
What is known from literature about the long COVID-19, its nomenclature, diagnosis, risk factors, signs/symptoms, pathophysiology, and the currently recommended management, and what are the gaps in this issue?
Inclusion criteria
-
Those related to long COVID, post-acute COVID, and long haulers of COVID-19
-
Those related to nomenclature, diagnosis criteria, pathophysiology, signs and symptoms, and managements
-
All types of reports were included: original studies (cohort, RCT, case–control, case-report, case series, and qualitative), reviews and editorials, viewpoints, guidelines, letter to editors and commentaries.
-
The articles should have been published in a peer-reviewed journal or be an organizational report
-
No language restriction was considered.
Exclusion criteria
-
Those irrelevant to COVID-19
-
Those related to acute COVID-19
-
Preprints
-
Unavailable full texts
Search strategy
We followed a four-step search strategy. First, on January 20, 2021 a limited preliminary search was done in multiple databases such as Google Scholar and PubMed for identifying the appropriate keywords. Next, on January 30, 2021 we adopted a search strategy including electronic databases of the following sources: Cochrane Library, PsycINFO, PubMed, Embase, Scopus, and the Web of Sciences. The results were reviewed using Endnote 20. After duplicate publications were removed, two authors separately checked the titles and abstracts and removed irrelevant studies according to the inclusion and exclusion criteria. Discrepancies about the inclusion/exclusion of any paper were resolved through discussion. Third, the two authors separately checked the included papers’ reference lists for identifying more relevant studies. In the fourth step, we glimpsed at google scholar for articles’ citing and current publications, maximizing our efforts to collect all relevant studies. Again, discrepancies were discussed for final approval in the third and fourth steps. We used the following keywords for our literature search: "long COVID" or "long haulers," or "post-acute COVID" or "chronic COVID syndrome" or "late sequela COVID" or "persistent COVID”. Table 1 shows our search strategy on all databases. As we had chosen no language restriction, we used Google to translate non-English papers and checked their eligibility.
Data extraction and synthesis
The following items were extracted from included papers: first author, country of the first author (also region and income level of the country), date of publication, date of submission, type of study (also the methodology in case of an original study), study category (diagnosis, nomenclature, pathophysiology, risk factors, signs/symptoms, or management), main topics in the categories (rehabilitation, pharmacologic options, thromboembolism, etc.), and the number of patients studied in the original investigations, their countries’ population and income level.
Moreover, for the original investigations, we extracted the following data from the articles: methodological approach, number of patients, the country and the geographic region where patients were investigated, based on World Bank report (2020–2021 fiscal year) [19]. A data extraction form was designed in Excel, and 3 independent authors extracted the data. Discrepancies were resolved through discussion. In the discussion section, we have synthesized the core themes of the study. The discussion section is divided into 6 categories where we present perspectives around nomenclature, diagnosis, pathophysiology, signs and symptoms, risk factors, and management of long COVID. Finally, we address the gaps and propose suggestions in the conclusion section.
Results
We retrieved 290 publications from our search (Fig. 1). After removing duplicates, publications were screened for the relevance of the title and abstract, resulting in the exclusion of 33 more publications. Then, 86 publications were evaluated for full-text eligibility. Of those, 20 articles were excluded (14 articles were not related to the Long COVID subject, and 6 were not available in full text). We were left with 66 articles for data synthesis. We then performed forward and backward screening of these papers' references and citations to identify as many relevant studies as possible. We found 54 additional relevant publications, that made a total of 120 publications as the basis for our analysis (see Online appendix 1).

PRISMA flow chart, the process of study selection. WOS Web of Science
Types of included papers
The first published papers date back to March 2020. The number of publications significantly increased over time. The distribution of the publications, based on the type of publication, is shown in Fig. 2. Of the 120 publications (Table 2), 67 (55.9%) presented original data as follows: 43 (35.9%) were original articles/papers [20,21,22,23,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62]. Fifteen (12.5%) publications were short articles with original data, as follows: 7 brief communications/reports [63,64,65,66,67,68,69] (5 cohort and 1 cross-sectional studies, and 1 case series), 1 commentary [70] (cross-sectional study), 6 letters to editors [71,72,73,74,75,76] (4 cross-sectional and 1 cohort studies, and 1 case series), and 1 short communication [77]. Fifty-four (45%) articles did not present original data. Among them were 33 (27.5%) short articles (shown in Fig. 2 as “non-original short communications”) as follows: 5 commentaries [78,79,80,81,82], 3 letters to the editors [83,84,85], 1 short communication [86], 1 “piece of mind” [87], 4 “news” [88,89,90,91], 1 perspective [1], 15 editorials [92,93,94,95,96,97,98,99,100,101,102,103,104,105,106], 1 special article [107], and 2 viewpoints [108, 109]. The other articles in this category were: 9 case reports/case series [110,111,112,113,114,115,116,117,118], 10 narrative reviews [10, 15, 119,120,121,122,123,124,125,126], 1 systematic review on the respiratory system [127], 4 guideline papers, 3 clinical updates, 1 “report”, and 1 consensus statement [128]. There was only 1 systematic review that elaborated on the pulmonary aftermaths of Long COVID [127]. There were 3 qualitative studies [26, 47, 57], only in 2 of them [26, 57], the study populations were well described. That was of significant concern since in qualitative studies the populations’ cultural and contextual aspects should be vividly mentioned.

Distribution of included papers based on types of publication
We found only one randomized clinical trial in our search [60]. Of all documents, 67 (55.9%) were studies with original data. Of those with original data, cross-sectional and cohort studies were the most common methodologies comprising 28 and 22 manuscripts, respectively. We found 3 qualitative studies; 2 from the UK and another 1 that did not explicitly mention the population region. More details are shown in Fig. 3. In our classification, we distinguished papers with original information from those that did not present empiric information. For instance, we divided the letter to the editors into two separate groups, those that contained original data and mentioned specific methodology, and those that did not do so.

Distribution of included papers based on their methodology. RCT Randomized Clinical Trial
Categories of included papers
As shown in Fig. 4, 13 (10.8%) articles, mainly editorials and commentaries, discussed a mixture of the following categories: nomenclature, signs/symptoms, pathophysiology, management, diagnosis, and risk factors. Fifty-nine (49.2%) articles presented signs and symptoms of Long COVID. Twenty-three (19.2%) articles reported on the generalized signs/symptoms (21 adults, 2 pediatrics), and the remaining 36 (30%) articles focused on specific organs/systems (9 focused on thromboembolism [29, 30, 36, 50, 66, 69, 114, 117, 118], 8 respiratory [23, 27, 37, 41, 44, 67, 75, 127], 4 neurology [46, 61, 102, 116], 2 musculoskeletal [53, 72], 5 cardiovascular [39, 49, 54, 112, 120], 3 mental health [21, 58, 108], 2 Multisystem Inflammatory Syndrome [MIS] [43, 113] (one about pediatrics MIS [43] and one on adults MIS [113]), 1 skin manifestations [70], 2 were exclusively about post-acute infectious fatigue [33, 122].

Categories and main topics of included papers; Inner doughnut illustrates the categorization of documents, and the outer doughnut illustrates the main topics of each category. MIS Multisystem Inflammatory Response
Thirteen (10.8%) articles evaluated the pathophysiology of Long COVID, including 8 neurologic [20, 32, 40, 73, 93, 104, 109, 126], 2 cardiovascular [77, 92], 1 fatigue [124], and 1 MIS in pediatric [121]. One paper was concerning the pathophysiology of multiple systems called in Fig. 4 by “multi-system” [31].
Twenty-eight (23.3%) articles were regarding management options: 13 rehabilitation care [22, 28, 45, 59, 60, 71, 94, 115, 119, 123, 129,130,131], 5 general care [26, 47, 57, 105, 132], 1 designed and validated a psychometric tool for assessing mental health consequences of Long COVID [42], and 1 was about “how to return back to the pre-morbidity activity level” [63], and 8 articles were on more comprehensive “multidisciplinary-care” of long COVID patients [84, 90, 98, 107, 128, 133,134,135].
Among the articles that are included in our report is an editorial from The Lancet that discusses historically the persistent symptoms after Russian influenza up to the current COVID-19 [1]. We also included a letter that proposed criteria for the definition of Long COVID [82].
There were several articles concerning the imaging features of Long COVID; but only 10 had focused explicitly and precisely on the radiologic features (3 MRI of the brain and olfactory nerves [20, 32, 40], 5 cardiovascular system including MRI, PET/CT and Echocardiography [39, 49, 54, 63, 77], 2 lung CT scan [44, 75]).
There were several articles that discussed the risk factors and predictors of develo** Long COVID. However, only 1 article focused on the risk factors for develo** mental health problems post-COVID [125]. Also, 1 article was about develo** a psychometric tool to assess the mental health consequences of long COVID [42].
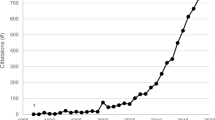
Date of submission and publication
There has been an increasing interest in literature on Long COVID. Our search was limited to the end of Jan 2021 (search in databases) and early February 2021 (backward and forward search). In our forward and backward search, we found three articles with a “first-online” in February 2021. Our analysis tried to evaluate the submission date, but we could not find the submission date for 53 articles. We report both dates of submission and publication to be more informative (Fig. 5).

Number of articles according to dates of submission and publication
Countries and regions
To overview the global spread of the works done on long COVID, we chose the first authors’ countries for the authors' representativeness. For each country, geographical region and level of income were included in our analysis as well.
In regard to the countries and geographic regions of the first authors, 74 (62%) authors were from 4 countries: 31 from UK, 19 from USA, 14 from Italy, and 10 from China. In regard to geographic regions, 61 (58%) authors were from Europe and Central Asia, 21 (17.6%) from North America, 12 from East Asia and Pacific, 6 from South Asia, 5 from the Middle East and North Africa, 2 from Sub-Saharan Africa, and 1 from Latin America and the Caribbean. According to the World Bank categorization of countries in 2020–2021 fiscal year, we categorized these regions to High, Upper-middle, lower-middle, and low-income countries [19]. Ninety-three (78.2%) first authors were from high-income countries, and only one author was from a low-income country.
There were 7 original studies on rehabilitation as the cornerstone management of Long COVID: 3 from Italy [28, 45, 71], 2 from China [59, 60], 1 from Austria [22], and 1 from Malawi [115].
Number of patients
As shown in Table 3, we report the number of patients based on the methodology of studies, level of income, and the regions of the investigated populations.
Language of the papers
Also, as the study was done without any language restriction, we screened title/abstract as well as the main text of non-English papers. Finally, we included one non-English paper in the Spanish language [137].
Discussion
Our study retrieved 120 papers based on inclusion and exclusion criteria. Hereby, we present them in five separate sections: “debates on nomenclature”, “pathophysiology”, “sign and symptoms”, “management”, and “concluding comments and suggestions”.
Debates on nomenclature
A standardized nomenclature is a gateway to adequate service provision and proper management of an illness. Thus, the lack of a standardized universally accepted definition and nomenclature for this disorder makes its appropriate diagnosis and management quite challenging. Many healthcare professionals and researchers are worried about attributing all symptoms to a single diagnosis. This could lead to a binary or even a quadripartite view that the symptoms such patients experience could be the result of up to four different syndromes (Permanent damage to vital organs; Post-intensive-care syndrome; Post-viral fatigue syndrome; and continued COVID-19 syndrome) [89]. This confusion has led to many patients with ongoing symptoms being ignored or not taken seriously. The hashtag "#Long COVID" has been frequently used in social media [86]. However, we found in our search that it lacks a universal definition. For example, National Institute for Health and Care Excellence (NICE) defined the "Long COVID" as "signs and symptoms that develop during/after the COVID-19 infection persisting for more than 4 weeks and could not be explained by any other diagnosis". In this categorization, the Long COVID consists of two categories, "Ongoing symptomatic COVID-19″, which indicates the symptoms lasting for 4–12 weeks; and "Post-COVID-19 syndrome", which means symptom persistence beyond 12 weeks [134].
Sivan et al., concur with our viewpoint that the definition presented by NICE is based on an obscure "by exclusion" diagnostic criteria. And that this categorization is not inclusive enough for all the post-acute complications of SARS-COV-2 under a single unified definition. It is suggested that the definition be changed to "continuing signs/symptoms beyond 4 weeks that can be attributed to COVID-19 infection" [103].
Baig has suggested using the term "Chronic COVID syndrome (CCS)" as opposed to “Long-COVID” or “Long-Haulers”. He also presented an organ-based staging of the illness to prioritize immediate care needs [78]. However, in a publication in the journal Nature, Marshall proposed the term "Coronavirus Long-Haulers" for those suffering from this condition [88]. Moreover, Greenhalgh et al., has proposed the term "post-infectious COVID-19" for those who continued with symptoms beyond 3 weeks after the onset of the disease. In this definition, the pre-requisition of a definite positive test for diagnosis was not considered since many patients are not tested, and false negatives are common [134]. In agreement with prior classification, Amenta et al., suggested that for COVID-19 patients hospitalized for 3 weeks, the onset of the post-infectious state could be delayed to the time of discharge from inpatient acute care services [15]. More recently, Anthony Fauci, MD director of the National Institute of Allergy and Infectious Diseases (NIAID), suggested the name “post-acute sequelae of SARS-CoV-2 infection” (PASC) [138].
Reaching an agreement on a definite terminology is vital. Using terms such as "post", "chronic", or "syndrome" carries assumptions about the underlying pathophysiology, which is unclear yet [97]. In our third and fourth phase of the search (looking at references and citations) we found almost a similar number of publications as our initial search (66 vs. 54 publications) of the databases. The authors believe that the lack of a standardized nomenclature resulted in poor homogeneity of the titles. This suggests that the WHO and other related organizations should make relevant unified terms to homogenize the literature. Besides, we suggest that other investigators use similar multi-step search strategies not to miss any relevant studies.
Diagnosis
In addition to debates on the nomenclature, there is also uncertainty on diagnostic criteria. There is the scarcity of discussion and proposals for such diagnostic criteria. We found only 1 article focused on the diagnostic criteria. Raveendran’s proposed criteria for Long COVID-19 consisted of 3 sectors: essential criteria, clinical criteria, and duration criteria [82]. Symptomatic and asymptomatic cases (during the acute phase) were separated, and each group based on RT-PCR, serologic testing, characteristic radiologic findings, and being in a high- or low- prevalence community was categorized into four subgroups: confirmed, probable, possible, or doubtful. In regard to duration criteria for such diagnosis the author proposed: beyond 2 weeks for mild disease, beyond 4 weeks for moderate to severe illness, and beyond 6 weeks for the critically ill in the acute phase. For those with asymptomatic acute phase: appearance of symptoms 1 week after antibody positivity or 2 weeks after having a positive RT-PCR or positive radiologic finding or contact with a suspected or positive COVID-19 case. Doubtful cases in the acute phase would fulfill the duration criteria of long COVID once they develop symptoms [26].
A few other reports have merely suggested a duration-criteria for long COVID, as persistence of symptoms beyond 3 weeks of the disease onset. The above-mentioned article is the only one that proposed a full-spectrum diagnostic-criteria. This lack of well-defined criteria to define Long COVID-19 emphasizes the need for international-health-organizations, such as, WHO to address this issue.
Pathophysiology
SARS-COV-2 virus invades many tissues and has a multiorgan and multisystem impact [130]. It is not unexpected, given that the Angiotensin-Converting Enzyme 2 (ACE2) receptor is expressed in many tissues [95]. Regarding the pathophysiology and underlying mechanism(s) involved in Long COVID, Baig suggested that oxidative stress and inflammation leads to weak immunologic response and incomplete virus eradication [109]. In addition, virus residuals and antigen remnants cause the ongoing inflammatory response and a vicious cycle leading to a chronic phase known as long COVID [109]. Meanwhile, the persistence of viremia and insufficient antibody generation [139], as well as, psychological factors like post-traumatic stress disorder (PTSD) may contribute to the development of the long COVID [42, 58]. The reason that some individuals are more prone to develop long COVID possibly lies in their genetic profile primarily related to the immune system, such as human leukocyte antigen (HLA). Future whole genomic studies may shed more light on this [109].
It has been shown that RNA of SARS-COV-2 may remain in the central nervous system after the acute phase and may result in the neuronal loss [140]. The considerable systemic inflammation in COVID-19, causes generalized endothelitis and disruption of the blood–brain barrier (BBB) [141, 142]. Moreover, it is known that systemic hyper-inflammation is a leading cause of neurodegeneration and cognitive decline [143, 144]. The latter requires longitudinal follow-up and studies on the pathogenesis and preventive measures, considering the already significant burden of neurodegenerative ailments such as Alzheimer's and Parkinson's disease, to prevent a delayed pandemic of new neurodegenerative conditions [10, 137].
It is thought that the direct invasion of the virus is responsible for persistent neuropsychiatric features of SARS-COV-2 [145]. Another suggested mechanism for the persistent syndrome is dysregulated immunologic response and virus-induced cytokine storm. Moreover, the production of pro-inflammatory cytokines such as IL-7 and IFNγ (interferon-gamma) can result in post-stroke depression, which is highly similar to pathobiology of SARS-COV-2 [93]. The COVID-19 patients have a higher level of NLRP3 inflammasome activation that in combination with interleukin-18 and interleukin-1β have been shown to adversely impact cerebral function [22]. Also, NLRP3 inflammasome-mediated systemic inflammation can lead to pathological accumulation of the peptides/proteins such as fibrillar amyloid-β resulting in the induction and aggravation of neurodegenerative illnesses such as Alzheimer's disease [146, 147]. It has been suggested that SARS-COV-2 infection may impair cognitive function that would lead to brain fog via selective targeting of the mitochondria of the neurons [104].
Dani et al., described long COVID symptoms, such as tachycardia, palpitation, orthostatic intolerance, breathlessness, and chest pain as the consequences of autonomic nervous system instability caused by deconditioning, hypovolemia or immune- or virus-mediated autonomic nervous system destruction [110]. In a case report of a COVID-19 patient with anti-microbial resistant Pseudomonas Aeruginosa infection, it was documented that 6 weeks after clearing of the viral infection, a significant number of activated T-cells and T-cells-specific for unrelated antigens were present, suggesting "a significant amount of by stander activation" which might contribute to recurring anti-bacterial-resistant infections [148]. A study measuring 96 immune response-associated proteins showed that even 40 days post-COVID-19 viral infection high levels of biomarkers related to innate anti-inflammatory and stress response were present [31].
The risk factors for develo** long COVID
Currently, the healthcare systems of all countries are overwhelmed with providing care for acutely ill COVID-19 patients. Soon, the health care systems will also be overwhelmed with providing long-term care for the survivors of the acute phase of the illness who are suffering from post-acute-phase signs and symptoms, i.e., long COVID. That made it of paramount importance for the authors to search for the existing literature on the risk factors for develo** long COVID after surviving the acute phase. Having reliable criteria to identify such vulnerable individuals would help the healthcare authorities to prepare for early screening and diagnosis, and providing proper facilities to care for their special needs.
In a prospective cohort study of confirmed COVID-19 infected adults, anosmia-dysgeusia was associated with younger age (< 65 years old), and in cases with severe pneumonia only opacities of lung surface on X-rays > 50% and higher heart rate at admission were independent predictors of Long COVID symptoms [50]. Estimated glomerular filtrate (eGFR) ≤ 60 mL/min/m2 and male sex were predictors of lingering abnormalities on spirometry. Moreover, a higher imaging score during the acute phase of illness was associated with the persistence of radiologic lung involvement, as expected [34]. Another prospective cohort study showed that the duration of oxygen supplementation in the acute phase of the disease was strongly associated with predicted DLCO % and total CT scores 12 weeks after symptom onset. Also, a significant association was found between dyspnea severity score on 12-week follow-up and predicted DLCO% [67]. Moreover, in a report of 52 cases of COVID pneumonia with at least 2 chest CT scans of around 3 months apart, a higher initial CT severity score, ICU admission, longer hospitalization, underlying medical conditions, higher initial WBC count, and development of leukocytosis during hospitalization were predictors of persistent pulmonary abnormalities on the second CT scan [23].
Long COVID patients are claimed to be susceptible to post-viral conditions similar to chronic fatigue syndrome and myalgic encephalomyelitis [83]. It was also reported that those with more than 5 symptoms in the first week of the acute illness were 4 times more susceptible to develop Long COVID; fatigue, headache, shortness of breath, hoarse voice, and myalgia were the most predictive symptoms; and the illness was more prevalent among women, older people, and those with obesity [136]. In another study, nearly two-thirds of adults with non-critical COVID-19 had complaints, including anosmia, dyspnea, and asthenia, up to 2 months following symptom onset. These prolonged symptoms were associated with age 40–60 years, hospital admission at symptom initiation, severe COVID-19, and dyspnea or abnormal chest auscultation [48].
The long-term effects of SARS-CoV-2-associated myocarditis are not known, however, based on the experience with other viral myocarditis, it is anticipated that those with a moderate to severe decrease in left ventricular ejection fraction, almost half would recover in the next 6–12 months, 25% would develop chronic systolic dysfunction, and 25% would require advanced therapies such as heart transplantation [92]. In addition, as post-viral myocarditis and other post-viral cardiac complications can result in a variety of cardiac sequela ranging from atrial and ventricular arrhythmias to sudden cardiac death, cardiac monitoring is recommended in such COVID-19 patients for 2–6 months post-recovery [120].
When it comes to long-term mental health problems, there are multifold risk factors. In regard to PTSD and chronic psychological distress after the acute phase of COVID-19, the greater exposure to the illness was associated with a higher incidence of subsequent PTSD. Loss of a loved one, hospitalization, containment measures such as isolation and quarantine, being in low-income regions, financial stressors, having disabilities, female gender, and older age were the most common mental health risk factors reported by preliminary studies [125]. Another study revealed that previous psychiatric diagnoses and higher systemic immune-inflammatory index are associated with higher post-COVID psychiatric problems. Systemic immune-inflammatory index (SII) is an objective marker of the balance between host systemic inflammation and immune response status considering together peripheral neutrophil, platelet, and lymphocyte counts. In this study, the authors explained that hospitalization duration was inversely correlated with mental health consequences because less in center healthcare support would increase self-isolation and loneliness [21]. It has also been reported that young people, women, and those with responsibilities and concern for others are more prone to develop posttraumatic symptomatology (PTS) following COVID-19 exposure, and hence, they deserve more attention [58].
Defining the factors that predict the development of Long COVID require more cohort and longitudinal studies. Since it is anticipated that there will be an enormous number of long COVID patients in the near future, identifying such predictors could help the Long COVID-specified clinics to prioritize the most vulnerable people and provide care to those in need.
Signs and symptoms
Multisystem studies and those related to general signs and symptoms
The persistent symptoms have been frequently reported. Huang et al., studied 1733 patients (nearly half men, median age of 57) in a clinical cohort follow-up in Wuhan, China. With a median follow-up of 186 days, 76% of the patients reported at least one persistent symptom, especially in women. The most reported symptoms were muscle weakness and fatigue (63%), followed by sleep difficulty (26%), and anxiety/depression (23%). More than half of them still had abnormalities in their chest computed tomography (CT) scan, that was independently associated with their pulmonary involvement during their acute illness. Also, of 86 patients who had experienced critical acute respiratory symptoms requiring oxygen mask/cannula and/or invasive/non-invasive mechanical ventilation during their hospital stay, 48 (56%) had impaired pulmonary diffusion tests in follow up (odds ratio of 4.6, range of 1.85–11.48). Besides, 13% of those with intact kidney function at the time of admission showed abnormal estimated glomerular filtration rate (eGFR) of < 90 mL/min/1.73 m2 in follow-up. Moreover, among 94 patients with antibody testing, the seropositivity of neutralizing antibodies was significantly lower in follow-up (58.5% with a median titer of 10) comparing to the acute phase (96.2% with the median titer of 19) [149].
In a prospective cohort study of 183 patients (mean age 57 years, 61.5% male), the persistence of symptoms at 35 days after hospitalization were: fatigue in 55%, dyspnea in 45%, and muscle pain in 51%, associated with a lower rating of physical health, mental health, quality of life, and active social role [55].
In a longitudinal study of 180 non-hospitalized RT-PCR proven COVID-19 patients, 53% of patients reported persistence of at least 1 symptom, and 33% reported 1 or 2 symptoms after a mean of 125 days from the onset of disease. The most prevalent persistent symptoms were fatigue, loss of smell and taste, and joint pain [51].
An app-based study about COVID-19 reported that while most of the patients fully recovered within 2 weeks, 1 in 10 patients still reported symptoms for 3 or more weeks. Their research showed that some people experienced fatigue, headache, cough, anosmia, sore throat, delirium, and chest pain as long-lasting symptoms [89]. The Public Health England Guidance implied that 1 in 10 mild cases who have not been admitted to the hospital had symptoms lasting for 4 weeks [133]. A cross-sectional study by Mandal et al., reported that the prevalence of persisting symptoms after a median follow-up of 54 days following hospitalization were: breathlessness (53%), cough (34%), fatigue (69%), and depressive symptoms (14.6%) [64].
Van den Borst et al., studied 124 patients (mean age 59 ± 14 years, 60% male) 3 months after recovery from acute COVID-19; 27 patients with mild, 51 with moderate, 26 with severe, and 20 with the critical disease. They found that a substantial number of patients reported problems across some domains of Nijmegen Clinical Screening Instrument (NCSI), including impairment in general quality of life (72%), fatigue (69%), and functional impairments in daily life (64%) [25].
Arnold et al., conducted a prospective cohort study with 110 COVID-19 survivors (median age of 60 years) who were followed with a median of 83 days after hospital admission and 90 days following the onset of COVID-19 symptoms. They divided the patients into mild (n = 27), moderate (n = 65), and severe (n = 18) groups. At follow-up, although most symptoms had been improved, however, 74% of the patients were still suffering from at least 1 ongoing symptom such as: breathlessness 39%, fatigue 39%, and insomnia 24%. In the mild group, 59% of patients reported ongoing symptoms, whereas the rates of ongoing symptoms for the moderate and severe groups were 75% and 89%, respectively [65].
Townsmen et al., studied 128 post-acute COVID-19 patients (mean age ± SD, 49.5 ± 15 years) at a median follow-up of 72 days after initial COVID-19 symptoms. More than half of the participants (52.3%) reported persistent fatigue regardless of the severity of their acute phase. They also found no association between post-acute COVID-19 fatigue and routine laboratory markers of inflammation and cell turnover (leukocyte, neutrophil or lymphocyte counts, neutrophil-to-lymphocyte ratio, lactate dehydrogenase, C-reactive protein) or pro-inflammatory molecules (IL-6 or sCD25) [33].
In a longitudinal study of 538 COVID-19 survivors (54.5% female; median age, 52.0 years), ** services for long COVID: lessons from a study of wounded healers. Clin Med. 2021;21:59." href="/article/10.1007/s15010-021-01666-x#ref-CR26" id="ref-link-section-d141937920e3318">26] reported that the participants repeatedly mentioned the role of social media in feeling better and diminishing their anxiety/stress and stigma when communicating with others and with their colleagues about their symptoms.
Pharmacological options
As hypothesized above, the core mechanism that possibly leads to chronic symptoms is an ongoing inflammatory state and oxidative stress. If proven, non-steroid anti-inflammatory drugs (NSAIDs), corticosteroids, and antioxidants such as CoQ10 could be possible approaches to management [109, 124].
Considering the nature of multisystem inflammatory syndrome in children (MIS-C), four initial treatment domains, including supportive care, empirical broad-spectrum antibiotics, anti-inflammatory agents, and anticoagulants are suggested. Anti-inflammatory management aims to reduce tissue inflammation to prevent or slow down the progression of coronary artery aneurysms [121].
Regarding anti-inflammatory agents, high dose IVIG and aspirin are advised as in Kawasaki disease [164]. However, there has been a debate over the administration of steroids in MIS-C. More recent studies suggest the use of corticosteroids based on each patient’s condition guided by a multi-disciplinary team [121]. Agents that target inflammatory molecules such as IL-1 [165], IL-6 [166], and TNF-α [167] are also suggested for the management of MIS-C.
While these medications might be protective on some occasions, these drugs' pros and cons should be weighed before prescribing due to the possible adverse effects. Metastasio et al., in their case study, reported using Kratum (Mitragyna speciosa) in their patient resulted in early recovery from the acute COVID-19 syndromes, including body pain, fatigue, and malaise, which are challenging for patients/physicians to deal with [168]. The therapeutic benefits of the plant are possibly related to the fact that it is a rich source of mitragynine, and the related metabolite 7-hydroxymitragynine[169]. Further studies may reveal the herbals’ benefit in long COVID haulers, especially for those with contraindications for NSAIDs. The harms and benefits of over-the-counter vitamins and supplements are unknown [134]. Although this is an early systematic review in the field, our qualitative assessment of the literature does not support prophylactic use of the anticoagulants for COVID-19 survivors; this requires multinational large-scale cohorts RCTs.
Role of physical and mental rehabilitation
Post-acute care is usually defined as the care provided following release from the hospital; however, here we extend this concept further to those surviving from an acute phase COVID-19, whether or not the patient had been admitted to a hospital. We recommend that the local public health authorities should develop adaptive post-acute COVID-19 care centers that specifically work on the palliative care of COVID-19 long haulers. Importantly, the vulnerable populations such as those in nursing homes, residential care centers, refugees, and asylum seekers should not be neglected [107]. As long COVID has a multisystem involvement, it has been suggested that a broad range of rehabilitation disciplines would be beneficial [128]. Cough and breathlessness are common. If there is no sign of superinfection or low oxygen saturation, breathing control exercise could help. The role of graded exercise in fatigue management is still a source of debate, and in long COVID patients it should be considered cautiously [134]. Myalgia Encephalomyelitis (ME) Association on post-viral fatigue syndrome (PVFS) highlighted the role of a multidisciplinary approach in managing chronic fatigue; it included resting, activity management, mental well-being, nutrition, and adequate sleep [78]. Also, based on the experience of post-infectious fatigue syndrome induced by Q-fever, it was generally thought the cognitive-behavioral therapy (CBT) could be beneficial in the management of post-infectious fatigue syndrome [170]; however, a recent study by Vink et al., reanalyzed the results of “Qure study” and showed that CBT was neither helpful in that regard nor possibly in the post-infectious fatigue syndrome of COVID-19 [119].
Another point to consider is early rehabilitation; the current definition of the recovery from COVID-19 is misleading as it mentions 3 weeks or without an episode of fever. We suggest that full recovery should be considered when the post-acute symptoms are adequately addressed; in doing so, Belli et al., in their study showed that the majority of their study population had a very severe degree of disability (dependency) at the time of discharge, demonstrated by Barthel index ≤ 60, requiring early rehabilitation [52]. Barthel Index is used to assess performance in activities of daily life (ADLs). In a report of the Italian cohort of post-acute COVID-19 patients, all of the included participants were grade 4 or 5 on the mMrc dyspnea scale, suggesting dyspnea during even minimal activities, and only a few of them could perform the 6-min walk test (6MWT) [45].
For those discharged from the hospital, Sun et al., recommend aerobic exercises, balance training, breathing training, and resistance strength training (start with low intensity and gradually raise the duration and intensity) as being beneficial in early recovery [123]. In a case series, Ferraro et al., recruited 7 post-acute infectious patients. All of the participants underwent a tailored rehabilitation intervention twice a day, each time for half an hour, for 6 days a week. In the beginning, 6 of 7 patients had fatigue, and 1 of them had an extreme sense of exertion. Following rehabilitation, 5 of 7 were without fatigue, and the remaining 2 had only a light sense of exertion. Besides, at the beginning of the study, all 7 patients had a deficient physical performance using the metrics of 6 MWT and 10 MWT. In this regard, the authors found a considerable improvement in outcomes of all patients, especially in 2 cases [71]. Liu et al., did a prospective 6-week respiratory rehabilitation, quasi-experimental study, with 72 post-acute COVID-19 patients discharged from the hospital (36 with and 36 without respiratory rehabilitation). They found that 6-week respiratory rehabilitation improved their respiratory function tests, their level of anxiety, and their quality of life in the elderly patients post-acute phase COVID-19 (all P-values ˂ 0.05) [60].
We would also like to highlight the development of more relevant functional assessment tools for COVID-19 survivors. For example, in spite of the broad use of 6 MWT in long COVID-related literature, it has been criticized as it shows "floor effects" because of respiratory failure and dyspnea in the acute phase, especially for discharged from ICU. Concerning this, Rivera-Lillo et al., suggested using 1-min sit and stand test instead of 6 MWT in the general population [171]. Also, Curci et al., suggested Chelsea Critical Care Physical Assessment Tool (CPAx) for those discharged from the ICU [172].
When to return to usual activities?
The crucial question is: “when can the survivors return to usual pre-infection activities?”. There is a paucity of evidence concerning this issue; however, we believe that this decision should also include the patients' occupation/activity and should be made on a one-by-one basis. For example, additional follow-up tests may be warranted in the case of competitive athletes who wishes to return to the field. A recent expert consensus recommended that mildly symptomatic athletes, besides 2 weeks of convalescence, should have a normal electrocardiogram and transthoracic echocardiography prior to returning to competitive sports [173]. In their review, Mitrani et al., [120] mentioned that there is no guideline to help physicians deal with the cardiac COVID-19 long haulers in their follow-up to rapidly diagnose complications such as arrhythmias or cardiomyopathies. There is an absolute need to screen for residual cardiac involvement in the convalescent phase of acute cardiac injury and for long-term sequelae of “post–COVID-19 cardiac syndrome”. The issue could become more complicated with a lack of proper assessment tools; Starekova et al., in a study of the utility of cardiac MRI as a screening tool among 145 asymptomatic or mildly symptomatic athletes who survived COVID-19, concluded that cardiac MRI is not useful in the cardiac assessment of the survivors [63].
Salman et al., propose a protocol for returning to the usual physical activity for the COVID-19 survivors [131]. There are several concerns about how and when the COVID survivors should start their physical activity/exercise. Some potential risks, including cardiac, pulmonary, and psychiatric, have to be stratified and considered before advising the return to physical activity. Besides, the physicians should consider patients’ pre-illness baseline physical activities before any recommendation. Those with persistent symptoms or a history of severe COVID-19 or cardiac involvement of COVID (e.g., myocarditis) are recommended to consult their medical doctor before returning to physical activities.
Also, Salman et al., recommended waiting at least a week after being asymptomatic to resume exercise. Moreover, the first 2 weeks of exercise should be minimal exertion, with gradual progression. The self-monitoring of the signs/symptoms and mood using a diary is highly recommended in all steps. For example, suppose patients felt fatigued or unable to feel recovered one hour or a day after exercise; in that case, they should step back to the prior activity level and seek medical advice when unsure.
Concluding comments and further suggestion
We found many discrepancies and lacunae in the myriad of papers available on the subject with data based on isolated cases and lacking the numerical strength for reliable data analysis. We found only one randomized clinical trial. We found a significant void of global collaborative studies on COVID 19 patients, their clinical presentation, management and long-term effects of the disease. We need a global consensus on the nomenclature of the long COVID 19 syndrome with a clear definition of the timeline to differentiate between prolonged symptomatic infection and actual post-recovery COVID 19 syndrome. Likewise, the diagnostic criteria need to be clearly established based on the severity of infection. More research is needed to focus on the pathophysiology of this complicated ailment. The clinical presentation needs to be analyzed between the spectrum of age, gender, race and concurrent comorbidities. Long-term follow-up has to be established with a clear focus on identifying the risk factors that predispose certain individuals to more complications versus others and a timeline for repeat testing or intervention and rehabilitation.
The unique pattern of morbidity and mortality that spans across a wide spectrum of demographics mandates that a more detailed, holistic approach is dedicated to the research of COVID 19 and its long-term effects.
After about 12 months following the declaration of the SARS-COV-2 pandemic by the World Health Organization, mysteries about this new virus, including the extent that the infection could cause long and persistent symptoms, are still not clear. There are also debates regarding the definition of prolonged disease, its diagnosis criteria, and its management. We highlight that the burden of the long COVID is overgrowing as more individuals become affected by the disease. Investigations in this field require considerable funding support and research investment. Also, we strongly suggest patient tracking via disease registries, similar to cancer registries.
Unfortunately, there is a wide gap in the literature related to the long-term COVID, which may reflect the need for long-term multi-national studies with adequate funding. This would allow for extensive subgroup analyses involving a wide range of ages, ethnicities, occupations, gender, and socioeconomic status. These studies will bring a more precise definition and symptom categorization for the long COVID. We also highlight the need for more rigorous research and develo** special guidelines in particular populations such as those with comorbidities and those with the risk of specific complications, such as competitive athletes. As stress is considered to play a role in the progression of the long COVID, the health care workers, as front-liners, are possibly more prone to have higher stress/anxiety and may experience a more symptomatic long COVID, which requires attention and further research [42, 58].
Moreover, unique guidelines need to be developed for particular occupations and activities, such as professional athletes, in whom the long COVID may be associated with more severe and potentially fatal consequences. We also highlight the need to support the vulnerable population by allocating financial and human resources to establish and reinforce telemedicine and in-person long COVID clinics. Finally, SARS-COV-2 has not been with us for long enough time for us to have a realistic estimation of the long-term picture of the post-infectious state; with the emergence of new studies, subsequent updated reviews are expected to appear soon.
To fill the above gaps, we present the following suggestions:
Definition and management of the evolving nature of the disease: World Health Organization did well in naming the COVID-19 for standardizing the literature; there is also a need to develop a timeline for COVID-19, and appropriate action plans in managing this complex disease. In that regard, recovery from COVID-19 is far from just being tested negative or following a limited predetermined period; a consensus on the definition of full recovery should be reached. In addition, the diversity of symptoms requires a more stringent categorization of symptoms; this will help the treatment and rehabilitation programs.
Long-term patient follow-up and global data-sharing: more long-term follow-up of the cross-country populations is recommended. Long-term studies should include all COVID-19 patients, even those with mild symptoms.
Investing in recovery support, including mental health and psychosocial support: since many of these patients have impaired performance in their daily tasks and suffer from mental health symptoms, launching an in-person or online portal based on peer groups is crucial.
Building capacity and knowledge base of health care workers: to deal more efficiently, we highlight the role of continuing medical education (CME) courses in develo** competencies regarding attitudes, skills, and knowledge, especially for primary care practitioners.
Personalized and more organized clinical management approach: since individual patients might experience specific symptoms, the need for personalized holistic management is notable.
Develo** innovative assessment tools for further studies: since this is a new disease that affects all organs, develo** newer functional metric tools to address its long-term impact on the mental and physical health status of the survivors is of paramount importance.
References
Honigsbaum M, Krishnan L. Taking pandemic sequelae seriously: from the Russian influenza to COVID-19 long-haulers. Lancet. 2020;396:1389–91.
Ahmed H, et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) coronavirus outbreaks after hospitalisation or ICU admission: a systematic review and meta-analysis. J Rehabil Med. 2020;52:1–11.
Wu X, Dong D, Ma D. Thin-section computed tomography manifestations during convalescence and long-term follow-up of patients with severe acute respiratory syndrome (SARS). Med Sci Monit Int Med J Exp Clin Res. 2016;22:2793.
Yu C, et al. Cardiovascular complications of severe acute respiratory syndrome. Postgrad Med J. 2006;82:140–4.
Wu Q, et al. Altered lipid metabolism in recovered SARS patients twelve years after infection. Sci Rep. 2017;7:1–12.
Chu KH, et al. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int. 2005;67:698–705.
Leung WK, et al. Enteric involvement of severe acute respiratory syndrome-associated coronavirus infection. Gastroenterology. 2003;125:1011–7.
Chau TN, et al. SARS-associated viral hepatitis caused by a novel coronavirus: report of three cases. Hepatology. 2004;39:302–10.
Yang J-K, et al. Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes. Acta Diabetol. 2010;47:193–9.
Higgins V, et al. COVID-19: from an acute to chronic disease? Potential long-term health consequences. Crit Rev Clin Lab Sci. Dec 2020;58:297–310. https://doi.org/10.1080/10408363.2020.1860895
Giannis D, Ziogas IA, Gianni P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J Clin Virol. 2020;127:104362.
Moldofsky H, Patcai J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. 2011;11:37.
Ngai JC, et al. The long-term impact of severe acute respiratory syndrome on pulmonary function, exercise capacity and health status. Respirology. 2010;15:543–50.
Tansey CM, et al. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch Intern Med. 2007;167:1312–20.
Amenta EM, et al. Postacute COVID-19: an overview and approach to classification. Open Forum Infect Dis. 2020;7:ofaa509. https://doi.org/10.1093/ofid/ofaa509.
Das KM, et al. Follow-up chest radiographic findings in patients with MERS-CoV after recovery. Indian J Radiol Imaging. 2017;27:342.
Wu Y, et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav Immun. 2020;87:18–22.
Tricco AC, et al. PRISMA extension for sco** reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–73.
World Bank country classifications by income level: 2020–2021. 2020; Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed 08 Feb 2021
Guedj E, et al. (18)F-FDG brain PET hypometabolism in patients with long COVID. Eur J Nuclear Med Mol Imaging. 2021;48:1–11.
Mazza MG, et al. Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain Behav Immun. 2020;89:594–600.
Puchner B, et al. Beneficial effects of multi-disciplinary rehabilitation in post-acute COVID-19-an observational cohort study. Eur J Phys Rehabil Med. 2021;57:189–98.
Tabatabaei SMH, et al. Chest CT in COVID-19 pneumonia: what are the findings in mid-term follow-up? Emerg Radiol. 2020;27:711–9.
**ong Q, et al. Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-centre longitudinal study. Clin Microbiol Infect. 2021;27:89–95.
van den Borst B, et al. Comprehensive health assessment three months after recovery from acute COVID-19. Clin Infect Dis. 2020. https://doi.org/10.1093/cid/ciaa1750.
Ladds E, et al. Develo** services for long COVID: lessons from a study of wounded healers. Clin Med. 2021;21:59.
Zhao YM, et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine. 2020;25:100463.
Curci C, et al. Functional outcome after inpatient rehabilitation in post-intensive care unit COVID-19 patients: findings and clinical implications from a real-practice retrospective study. Eur J Phys Rehabil Med. 2021;57:443–450.
Rashidi F, et al. Incidence of symptomatic venous thromboembolism following hospitalization for coronavirus disease 2019: prospective results from a multi-center study. Thromb Res. 2021;198:135–8.
Salisbury R, et al. Incidence of symptomatic, image-confirmed venous thromboembolism following hospitalization for COVID-19 with 90-day follow-up. Blood Adv. 2020;4:6230–9.
Heywood WE, et al. The long tail of Covid-19’ - The detection of a prolonged inflammatory response after a SARS-CoV-2 infection in asymptomatic and mildly affected patients. F1000Research. 2021;9:1349.
Kandemirli SG, et al. Olfactory bulb MRI and paranasal sinus CT findings in persistent COVID-19 anosmia. Acad Radiol. 2021;28(1):28–35.
Townsend L, et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE. 2020;15:e0240784.
Moreno-Pérez O, et al. Post-acute COVID-19 syndrome. Incidence and risk factors: a Mediterranean cohort study. J Infect. 2021;82:378–83.
Halpin SJ, et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: a cross-sectional evaluation. J Med Virol. 2021;93:1013–22.
Roberts LN, et al. Postdischarge venous thromboembolism following hospital admission with COVID-19. Blood J Am Soc Hematol. 2020;136:1347–50.
Guler SA, et al. Pulmonary function and radiological features four months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study. Eur Respir J. 2021;57:2003690.
Fisher KA, et al. Symptoms and recovery among adult outpatients with and without COVID-19 at 11 healthcare facilities—July 2020, United States. Influenza Other Respir Viruses. 2021;15:345–51.
Małek ŁA, et al. Cardiac involvement in consecutive elite athletes recovered from Covid-19: a magnetic resonance study. J Magn Reson Imaging. 2021;53:1723–9.
Lu Y, et al. Cerebral micro-structural changes in COVID-19 patients–an MRI-based 3-month follow-up study. EClinicalMedicine. 2020;25:100484.
Liu C, et al. Chest computed tomography and clinical follow-up of discharged patients with COVID-19 in Wenzhou City, Zhejiang, China. Ann Am Thorac Soc. 2020;17:1231–7.
Forte G, et al. COVID-19 pandemic in the Italian population: validation of a post-traumatic stress disorder questionnaire and prevalence of PTSD symptomatology. Int J Environ Res Public Health. 2020;17:4151.
Godfred-Cato S, et al. COVID-19-associated multisystem inflammatory syndrome in children - United States, March-July 2020. Morb Mortal Wkly Rep. 2020;69:1074–80.
Lerum TV, et al. Dyspnoea, lung function and CT findings three months after hospital admission for COVID-19. Eur Respir J. 2020;57:2003448.
Curci C, et al. Early rehabilitation in post-acute COVID-19 patients: data from an Italian COVID-19 rehabilitation unit and proposal of a treatment protocol. A cross-sectional study. Eur J Phys Rehabil Med. 2020;56:633–41.
Boscolo-Rizzo P, et al. Evolution of altered sense of smell or taste in patients with mildly symptomatic COVID-19. JAMA Otolaryngol-Head Neck Surg. 2020;146:729–32.
Kingstone T, et al. Finding the’right’GP: a qualitative study of the experiences of people with long-COVID. BJGP Open. 2020;4:bjgpopen20X101143.
Carvalho-Schneider C, et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin Microbiol Infect. 2020;27:258–63.
Brito D, et al. High prevalence of pericardial involvement in college student athletes recovering from COVID-19. JACC Cardiovasc Imaging. 2020;14:541–55.
Engelen M, Vanassche T, Balthazar T. Incidence of venous thromboembolism in patients discharged after COVID-19 hospitalisation. Res Pract Thromb Haemost. 2020;4. Available in https://abstracts.isth.org/abstract/incidence-of-venous-thromboembolism-in-patients-discharged-after-covid-19-hospitalisation/.
Petersen MS, et al. Long COVID in the Faroe Islands-a longitudinal study among non-hospitalized patients. Clin Infect Dis. 2020. https://doi.org/10.1093/cid/ciaa1792.
Belli S, et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived the hospitalisation. Eur Respir J. 2020;56:2002096.
Paneroni M, et al. Muscle strength and physical performance in patients without previous disabilities recovering from COVID-19 pneumonia. Am J Phys Med Rehabil. 2020;100:105–9.
Puntmann VO, et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5:1265–73.
Jacobs LG, et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS ONE. 2020;15:e0243882.
Goërtz YMJ, et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: the post-COVID-19 syndrome? ERJ Open Res. 2020;6:00542–2020.
Ladds E, et al. Persistent symptoms after Covid-19: qualitative study of 114 “long Covid” patients and draft quality principles for services. BMC Health Serv Res. 2020;20:1–13.
Jiang H-J, et al. Psychological impacts of the COVID-19 epidemic on Chinese people: exposure, post-traumatic stress symptom, and emotion regulation. Asian Pac J Trop Med. 2020;13:252.
Li Z, et al. Rehabilitation needs of the first cohort of post-acute COVID-19 patients in Hubei, China. Eur J Phys Rehabil Med. 2020;56:339–44.
Liu K, et al. Respiratory rehabilitation in elderly patients with COVID-19: a randomized controlled study. Complement Ther Clin Pract. 2020;39:101166.
Altundag A, et al. The temporal course of COVID-19 anosmia and relation to other clinical symptoms. Eur Arch Oto-Rhino-Laryngol. 2020. https://doi.org/10.1007/s00405-020-06496-5.
Liang L, et al. Three-month follow-up study of survivors of Coronavirus Disease 2019 after discharge. J Korean Med Sci. 2020;35:e418.
Starekova J, et al. Evaluation for myocarditis in competitive student athletes recovering from coronavirus disease with cardiac magnetic resonance imaging. JAMA Cardiol. 2021. https://doi.org/10.1001/jamacardio.2020.7444.
Mandal S, et al. ‘Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax. 2020;76:396–8.
Arnold DT, et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: results from a prospective UK cohort. Thorax. 2020;76:399–401.
Patell R, et al. Postdischarge thrombosis and hemorrhage in patients with COVID-19. Blood J Am Soc Hematol. 2020;136:1342–6.
Shah AS, et al. A prospective study of 12-week respiratory outcomes in COVID-19-related hospitalisations. Thorax. 2020;76:402–4.
Bellan M, et al. Respiratory and psychophysical sequelae among patients with COVID-19 four months after hospital discharge. JAMA Netw Open. 2021;4:e2036142–e2036142.
Eswaran H, et al. Vascular thromboembolic events following COVID-19 hospital discharge: incidence and risk factors. Res Pract Thromb Haemost. 2021;5:292–5.
McMahon DE, et al. Long COVID in the skin: a registry analysis of COVID-19 dermatological duration. Lancet Infect Dis. 2021. https://doi.org/10.1016/S1473-3099(20)30986-5.
Ferraro F, et al. COVID-19 related fatigue: Which role for rehabilitation in post-COVID-19 patients? A case series. J Med Virol. 2020;1:1. https://doi.org/10.1002/jmv.26717.
Zampogna E, et al. Functional impairment during post-acute COVID-19 phase: preliminary finding in 56 patients. Pulmonology. 2021. https://doi.org/10.1016/j.pulmoe.2020.12.008.
Tsivgoulis G, et al. Olfactory bulb and mucosa abnormalities in persistent COVID-19-induced anosmia: a magnetic resonance imaging study. Eur J Neurol. 2021;28:e6–8.
Carfì A, Bernabei R, Landi F. Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324:603–5.
Truffaut L, et al. Post-discharge critical COVID-19 lung function related to severity of radiologic lung involvement at admission. Respir Res. 2021;22:1–6.
Garrigues E, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. 2020;81:e4–6.
Sollini M, et al. Vasculitis changes in COVID-19 survivors with persistent symptoms: an [18 F] FDG-PET/CT study. Eur J Nuclear Med Mol Imaging. 2020;48:1–7.
Baig AM. Chronic COVID syndrome: need for an appropriate medical terminology for Long-COVID and COVID Long-Haulers. J Med Virol. 2020;93:2555–6.
Rolfe RJ, Smith CM, Wolfe CR. The emerging chronic sequelae of COVID-19 and implications for North Carolina. N C Med J. 2021;82:75–8.
Yelin D, et al. Long COVID-19-it’s not over until? Clin Microbiol Infect. 2020. https://doi.org/10.1016/j.cmi.2020.12.001.
Yelin D, et al. Long-term consequences of COVID-19: research needs. Lancet Infect Dis. 2020;20:1115–7.
Raveendran AV. Long COVID-19: challenges in the diagnosis and proposed diagnostic criteria. Diabetes Metab Syndr. 2021;15:145.
Miller A. COVID-19: not just an acute illness. Trends Urol Men’s Health. 2020;11:17–9.
Burgers J. “Long covid”: the Dutch response. BMJ. 2020. https://doi.org/10.1136/bmj.m3202.
Perego E, et al. Why the patient-made term “Long Covid” is needed. Wellcome Open Res. 2020;5:224.
Callard F, Perego E. How and why patients made Long Covid. Soc Sci Med. 2021;268:113426.
Siegelman JN. Reflections of a COVID-19 long hauler. JAMA. 2020;324:2031–2.
Marshall M. The lasting misery of coronavirus long-haulers. Nature. 2020;585:339–41.
Mahase E. Long covid could be four different syndromes, review suggests. BMJ. 2020;371:m3981.
Wise J. Long covid: doctors call for research and surveillance to capture disease. BMJ. 2020;370:m3586.
Nabavi N. Long covid: How to define it and how to manage it. BMJ. 2020;370:m3489.
Becker RCX. Anticipating the long-term cardiovascular effects of COVID-19. J Thromb Thrombolysis. 2020;50:512–24.
Wijeratne T, Crewther S. COVID-19 and long-term neurological problems: Challenges ahead with Post-COVID-19 Neurological Syndrome. Aust J Gen Pract. 2021;50. https://doi.org/10.31128/AJGP-COVID-43. Online ahead of print.
Negrini S, et al. Facing in real time the challenges of the Covid-19 epidemic for rehabilitation. Eur J Phys Rehabil Med. 2020;56:313–5.
The L. Facing up to long COVID. Lancet. 2020;396:1861.
Shelley BP. Gaps in knowledge: unmasking post-(Acute) COVID-19 syndrome and potential long-term complications in COVID-19 survivors. Arch Med Health Sci. 2020;8:173.
Covid NL. let patients help define long-lasting COVID symptoms. Nature. 2020;586:170.
Basheer A. Long COVID–need for follow-up clinics. J Curr Res Sci Med. 2020;6:71.
Manolis AS, Manolis TA. Long COVID: an emerging puzzle: long COVID. Rhythmos. 2021;16:89–94.
Nath A. Long-haul COVID. Neurology. 2020;95:559.
Hertting O. More research is needed on the long-term effects of COVID-19 on children and adolescents. Acta Paediatr. 2021;110:744.
Butler M, et al. Neuropsychiatric complications of covid-19. BMJ. 2020. https://doi.org/10.1136/bmj.m3871.
Sivan M, Taylor S. NICE guideline on long covid. BMJ. 2020. https://doi.org/10.1136/bmj.m4938.
Stefano GB, et al. Selective neuronal mitochondrial targeting in SARS-CoV-2 infection affects cognitive processes to induce “Brain Fog” and results in behavioral changes that favor viral survival. Med Sci Monit. 2021;27:e930886.
Greenhalgh T, Knight M. Long COVID: a primer for family physicians. Am Fam Physician. 2020;102:716–7.
Meeting the challenge of long COVID. Nat Med. 2020;26:1803. https://doi.org/10.1038/s41591-020-01177-6
Tumlinson A, et al. Post-acute care preparedness in a COVID-19 world. J Am Geriatr Soc. 2020;68:1150–4.
Asim M, van Teijlingen E, Sathian B. Coronavirus disease (COVID-19) and the risk of post-traumatic stress disorder: a mental health concern in Nepal. Nepal J Epidemiol. 2020;10:841.
Baig AM. Deleterious outcomes in long-hauler COVID-19: the effects of SARS-CoV-2 on the CNS in Chronic COVID Syndrome. ACS Chem Neurosci. 2020;11:4017–20.
Dani M, et al. Autonomic dysfunction in “long COVID”: rationale, physiology and management strategies. Clin Med (Lond). 2021;21:e63–7.
Ludvigsson JF. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta Paediatr. 2021;110:914–21.
Miglis MG, et al. A case report of postural tachycardia syndrome after COVID-19. Clin Auton Res. 2020;30:449–51.
Morris SB, et al. Case series of multisystem inflammatory syndrome in adults associated with SARS-CoV-2 infection—United Kingdom and United States, March–August 2020. Morb Mortal Wkly Rep. 2020;69:1450.
Bastopcu M. Extensive arterial thrombus following discharge after a Covid-19 infection. Ann Vasc Surg. 2020;72:205–8.
Bickton FM, et al. An improvised pulmonary tele-rehabilitation programme for post-acute COVID-19 patients would be feasible and acceptable in a low-resource setting: a case report. Am J Phys Med Rehabil. 2021. https://doi.org/10.1097/phm.0000000000001666.
Raahimi MM, et al. Late onset of Guillain-Barré syndrome following SARS-CoV-2 infection: part of “long COVID-19 syndrome”? BMJ Case Rep. 2021;14:e240178.
Kumar MA, Krishnaswamy M, Arul JN. Post COVID-19 sequelae: venous thromboembolism complicated by lower GI bleed. BMJ Case Rep CP. 2021;14:e241059.
Touré A, et al. Post-COVID-19 late pulmonary embolism in a young woman about a case. Open J Emerg Med. 2020;8:79–85.
Vink M, Vink-Niese A. Could cognitive behavioural therapy be an effective treatment for long COVID and post COVID-19 fatigue syndrome? Lessons from the qure study for Q-fever fatigue syndrome. Healthcare. 2020;8:552. https://doi.org/10.3390/healthcare8040552.
Mitrani RD, Dabas N, Goldberger JJ. COVID-19 cardiac injury: implications for long-term surveillance and outcomes in survivors. Heart Rhythm. 2020;17:1984–90.
McMurray JC, et al. Multisystem inflammatory syndrome in children (MIS-C), a post-viral myocarditis and systemic vasculitis-a critical review of its pathogenesis and treatment. Front Pediatr. 2020;8:871.
Smith AP. Post-viral fatigue: implications for long COVID. Asian J Res Infect Dis. 2021;6:17–23.
Sun T, et al. Rehabilitation of patients with COVID-19. Expert Rev Respir Med. 2020;14:1249–56.
Wood E, Hall KH, Tate W. Role of mitochondria, oxidative stress and the response to antioxidants in myalgic encephalomyelitis/chronic fatigue syndrome: a possible approach to SARS-CoV-2 ‘long-haulers’? Chronic Dis Transl Med. 2020. https://doi.org/10.1016/j.cdtm.2020.11.002.
Boyraz G, Legros DN. Coronavirus disease (COVID-19) and traumatic stress: probable risk factors and correlates of posttraumatic stress disorder. J Loss Trauma. 2020;25:503–22.
Serrano-Castro PJ, et al. Impact of SARS-CoV-2 infection on neurodegenerative and neuropsychiatric diseases: a delayed pandemic? Neurologia. 2020. https://doi.org/10.1016/j.nrl.2020.04.002.35(4):p.245-251.
Torres-Castro R, et al. Respiratory function in patients post-infection by COVID-19: a systematic review and meta-analysis. Pulmonology. 2020. https://doi.org/10.1016/j.pulmoe.2020.10.013.
Barker-Davies RM, et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br J Sports Med. 2020;54:949–59.
Pinto M, et al. Post-acute COVID-19 rehabilitation network proposal: from intensive to extensive and home-based IT supported services. Int J Environ Res Public Health. 2020;17:9335.
Wade DT. Rehabilitation after COVID-19: an evidence-based approach. Clin Med. 2020;20:359.
Salman D, et al. Returning to physical activity after covid-19. BMJ. 2021;372:m4721.
George PM, et al. Respiratory follow-up of patients with COVID-19 pneumonia. Thorax. 2020;75:1009–16.
COVID-19 rapid guideline: managing the long-term effects of COVID-19. 2020. https://www.ncbi.nlm.nih.gov/books/NBK567261/ Accessed 18 Dec 2020.
Greenhalgh T, et al. Management of post-acute covid-19 in primary care. BMJ. 2020;370:m3026.
Myalgic Encephalomyelitis (ME) Association. Post-viral fatigue (PVF) and Post-viral fatigue syndrome (PVFS) following coronavirus infection. 2020. https://meassociation.org.uk/wp-content/uploads/MEA-PVF-and-PVFS-Following-Coronavirus-Infection-30.04.20.pdf. Accessed 18 Feb 2021.
Mendelson M, et al. Long-COVID: an evolving problem with an extensive impact. S Afr Med J. 2021;111:10–3.
Serrano-Castro PJ, et al. Influencia de la infección SARS-Cov2 sobre enfermedades neurodegenerativas y neuropsiquiátricas: UNA pandemia demorada? Neurologia. 2020;35:245.
Fauci Introduces New Acronym for Long COVID at White House Briefing. 2021. https://www.medscape.com/viewarticle/946419. Accessed 29 Feb 2021.
Wu F, et al. Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications. medRxiv. 2020;9:199. https://doi.org/10.1101/2020.03.30.20047365.
Montalvan V, et al. Neurological manifestations of COVID-19 and other coronavirus infections: a systematic review. Clin Neurol Neurosurg. 2020;194:105921.
Huang C, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506.
Libby P, Lüscher T. COVID-19 is, in the end, an endothelial disease. Eur Heart J. 2020;41:3038–44.
Walker KA, et al. The association of mid-to late-life systemic inflammation with white matter structure in older adults: the atherosclerosis risk in communities study. Neurobiol Aging. 2018;68:26–33.
Walker KA, et al. Midlife systemic inflammatory markers are associated with late-life brain volume: the ARIC study. Neurology. 2017;89:2262–70.
Troyer EA, Kohn JN, Hong S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav Immun. 2020;87:34–9.
Tejera D, et al. Systemic inflammation impairs microglial Aβ clearance through NLRP3 inflammasome. EMBO J. 2019;38:e101064.
He X-F, et al. NLRP3-dependent microglial training impaired the clearance of amyloid-beta and aggravated the cognitive decline in Alzheimer’s disease. Cell Death Dis. 2020;11:849.
Gregorova M, et al. Post-acute COVID-19 associated with evidence of bystander T-cell activation and a recurring antibiotic-resistant bacterial pneumonia. Elife. 2020;9:e63430.
Huang C, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397:220–32.
Huang Y, et al. Impact of coronavirus disease 2019 on pulmonary function in early convalescence phase. Respir Res. 2020;21:163.
Rajpal S, et al. Cardiovascular magnetic resonance findings in competitive athletes recovering from COVID-19 infection. JAMA Cardiol. 2021;6:116–8.
Del Rio C, Collins LF, Malani PJJ. Long-term health consequences of COVID-19. JAMA. 2020;324:1723–4.
Maron BJ, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 3: hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis: a scientific statement from the American Heart Association and American College of Cardiology. Circulation. 2015;132:e273–80.
Recalcati S. Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol. 2020;34:e212–3.
Jia JL, et al. Cutaneous manifestations of COVID-19: a preliminary review. J Am Acad Dermatol. 2020;83:687–90.
Estébanez A, et al. Cutaneous manifestations in COVID-19: a new contribution. J Eur Acad Dermatol Venereol. 2020;34:e250–1.
Colmenero I, et al. SARS-CoV-2 endothelial infection causes COVID-19 chilblains: histopathological, immunohistochemical and ultrastructural study of seven paediatric cases. Br J Dermatol. 2020;183:729–37.
Wijeratne T, Crewther S. Post-COVID 19 Neurological Syndrome (PCNS); a novel syndrome with challenges for the global neurology community. J Neurol Sci. 2020;419:117179.
Helms J, et al. Neurologic features in severe SARS-CoV-2 infection. N Engl J Med. 2020;382:2268–70.
Garner P. Covid-19 at 14 weeks-phantom speed cameras, unknown limits, and harsh penalties. The BMJ Opinion, 2020. https://blogs.bmj.com/bmj/2020/06/23/paul-garner-covid-19-at-14-weeks-phantom-speed-cameras-unknown-limits-and-harsh-penalties/.
Rehman S, et al. Syndrome resembling Kawasaki disease in COVID-19 asymptomatic children. J Infect Public Health. 2020;13:1830–2.
Kabeerdoss J, et al. Severe COVID-19, multisystem inflammatory syndrome in children, and Kawasaki disease: immunological mechanisms, clinical manifestations and management. Rheumatol Int. 2021;41:19–32.
Rauf A, et al. Multisystem inflammatory syndrome with features of atypical kawasaki disease during COVID-19 pandemic. Indian J Pediatr. 2020;87:745–7.
Henderson LA, et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS–CoV-2 and hyperinflammation in pediatric COVID-19: version 1. Arthritis Rheumatol. 2020;72:1791.
Cavalli G, et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: a retrospective cohort study. Lancet Rheumatol. 2020;2:e325–31.
Ye Q, Wang B, Mao J. The pathogenesis and treatment of theCytokine Storm’in COVID-19. J Infect. 2020;80:607–13.
Dolinger MT, et al. Pediatric Crohn’s disease and multisystem inflammatory syndrome in children (MIS-C) and COVID-19 treated with infliximab. J Pediatr Gastroenterol Nutr. 2020. https://doi.org/10.1097/MPG.0000000000002809.
Metastasio A, et al. Can Kratom (Mitragyna speciosa) alleviate COVID-19 pain? A case study. Front Psychiatry. 2020;11:1298.
Kruegel AC, Grundmann O. The medicinal chemistry and neuropharmacology of kratom: a preliminary discussion of a promising medicinal plant and analysis of its potential for abuse. Neuropharmacology. 2018;134:108–20.
Keijmel SP, et al. The Qure study: Q fever fatigue syndrome–response to treatment; a randomized placebo-controlled trial. BMC Infect Dis. 2013;13:1–9.
Rivera-Lillo G, et al. Functional capacity assessment in COVID-19 patients. Eur J Phys Rehabil Med. 2020. https://doi.org/10.23736/s1973-9087.20.06525-9.
Curci C, et al. Which are the main assessment tools of functional capacity in post-acute COVID-19 patients admitted to rehabilitation units? Eur J Phys Rehabil Med. 2020. https://doi.org/10.23736/S1973-9087.20.06579-X.
Phelan D, Kim JH, Chung EHJJc. A game plan for the resumption of sport and exercise after coronavirus disease 2019 (COVID-19) infection. JAMA Cardiol. 2020;5:1085–6.
Funding
The study was performed without the financial support of any funding organization.
Author information
Authors and Affiliations
Contributions
HA and MH conceptualized the study. NG, BB and MK led the literature review with contributions from BR, JM, AAP, LMM, SP, MH, AA and HA. MH led the data analysis with contribution from HA, LM and AA. All authors contributed to the development of the analysis plan, collection and analysis of primary data, data interpretation, and critically reviewed the revised initial draft of the manuscript. All authors have read and approve the final draft.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest in this work.
Ethical approval
The study does not require ethical approval, because the systematic review is based on already published reports and the original data are anonymous. All of the patients’ information were deidentified.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Akbarialiabad, H., Taghrir, M.H., Abdollahi, A. et al. Long COVID, a comprehensive systematic sco** review. Infection 49, 1163–1186 (2021). https://doi.org/10.1007/s15010-021-01666-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-021-01666-x