
Abstract
Background
The role of routine preoperative oesopha gogastroduodenoscopy (OGD) for all bariatric surgery candidates is controversial. We aim to investigate the prevalence of clinically significant OGD findings in a primarily Chinese obese population and identify factors that predict a normal screening OGD.
Methods
Medical records of patients who underwent primary bariatric surgery in our centre from August 2002 to December 2014 were reviewed. OGD findings were classified into two groups: group 1 consisted of normal findings and abnormal findings that would not alter the surgical plan; group 2 consisted of lesions that might delay or alter the surgical procedure.
Results
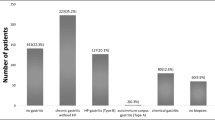
We identified 268 patients (169 female), of mean age 39.1 ± 10.8 years, mean baseline body weight 108.7 ± 6.1 kg and mean body mass index (BMI) 40.3 ± 6.1 kg/m2 for analysis. Overall prevalence of abnormal OGD findings was 51.1 %, which included gastritis (32.5 %), hiatus hernia (17.9 %), duodenitis (8.6 %) and erosive oesophagitis (7.5 %); 27.2 % had group 2 lesions. Univariate analysis revealed older age (p = 0.016), use of NSAIDs (p = 0.004) and presence of reflux symptoms (p = 0.029) as significant risk factors of group 2 lesions. On multivariate analysis, use of NSAIDs (p = 0.015) and reflux symptoms (p = 0.039) remained significant predictive factors. In the low-risk subgroup (40 years and younger, without reflux symptoms or use of NSAIDs), the prevalence of group 2 abnormalities was 18.9 %.
Conclusions
Significant endoscopic abnormalities are common among obese Chinese patients which may delay or change the surgical plan. The negative predictive value in low-risk patients was not strong. We therefore recommend routine preoperative endoscopy for all patients.

Similar content being viewed by others


References
Suter M, Dorta G, Giusti V, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly obese patients. Obes Surg. 2004;14(7):959–66.
El-Serag HB, Graham DY, Satia JA, et al. Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am J Gastroenterol. 2005;100(6):1243–50.
Kang MS, Park DI, Oh SY, et al. Abdominal obesity is an independent risk factor for erosive esophagitis in a Korean population. J Gastroenterol Hepatol. 2007;22(10):1656–61.
Menon S, Trudgill N. Risk factors in the aetiology of hiatus hernia: a meta-analysis. Eur J Gastroenterol Hepatol. 2011;23:133–8.
Sharaf RN, Weinshel EH, Bini EJ, et al. Endoscopy plays an important preoperative role in bariatric surgery. Obes Surg. 2004;14(10):1367–72.
Zeni TM, Frantzides CT, Mahr C, et al. Value of preoperative upper endoscopy in patients undergoing laparoscopic gastric bypass. Obes Surg. 2006;16(2):142–6.
Muñoz R, Ibáñez L, Salinas J, et al. Importance of routine preoperative upper GI endoscopy: why all patients should be evaluated? Obes Surg. 2009;19(4):427–31.
Loewen M, Giovanni J, Barba C. Screening endoscopy before bariatric surgery: a series of 448 patients. Surg Obes Relat Dis. 2008;4(6):709–12.
Schigt A, Coblijn U, Lagarde S, et al. Is esophagogastroduodenoscopy before Roux-en-Y gastric bypass or sleeve gastrectomy mandatory? Surg Obes Relat Dis. 2014;10(3):411–7. quiz 565–6.
Dhariwal A, Plevris JN, Lo NT, et al. Age, anemia, and obesity-associated oxygen desaturation during upper gastrointestinal endoscopy. Gastrointest Endosc. 1992;38:684–8.
ASGE Standards of Practice Committee. The role of endoscopy in the bariatric surgery patient. Gastrointest Endosc. 2015;81(5):1063–72.
Sauerland S, Angrisani L, Belachew M, et al. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2005;19:200–21.
Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Surg Obes Relat Dis. 2013;9(2):159–91.
Lee WJ, Wang W. Bariatric surgery: Asia-Pacific perspective. Obes Surg. 2005;15(6):751–7.
Kasama K, Mui W, Lee WJ, et al. IFSO-APC consensus statements 2011. Obes Surg. 2012;22(5):677–84.
Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101(8):1900–20. quiz 1943.
Merrouche M, Sabaté JM, Jouet P, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly obese patients before and after bariatric surgery. Obes Surg. 2007;17(7):894–900.
Greenstein RJ, Nissan A, Jaffin B. Esophageal anatomy and function in laparoscopic gastric restrictive bariatric surgery: implications for patient selection. Obes Surg. 1998;8(2):199–206.
Bernante P, Breda C, Zangrandi F, et al. Emergency sleeve gastrectomy as rescue treatment for acute gastric necrosis due to type II paraesophageal hernia in an obese woman with gastric banding. Obes Surg. 2008;18(6):737–41.
Küper MA, Kratt T, Kramer KM, et al. Effort, safety, and findings of routine preoperative endoscopic evaluation of morbidly obese patients undergoing bariatric surgery. Surg Endosc. 2010;24:1996–2001.
Dhariwal A, Plevris JN, Lo NT, et al. Age, anemia, and obesity associated oxygen desaturation during upper gastrointestinal endoscopy. Gastrointest Endosc. 1992;38:684–8.
Madan AKTD, Isom J, Minard G, et al. Monitored anesthesia care with propofol versus surgeon-monitored sedation with benzodiazepines and narcotics for preoperative endoscopy in the morbidly obese. Obes Surg. 2008;18:545–8.
Soricelli E, Iossa A, Casella G, et al. Sleeve gastrectomy and crural repair in obese patients with gastroesophageal reflux disease and/or hiatal hernia. Surg Obes Relat Dis. 2013;9(3):356–61.
Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975–2012, National Cancer Institute. Bethesda, MD; [updated 2015 April; cited 2015 June 6] Available from http://seer.cancer.gov/csr/1975_2012/.
Schirmer B, Erenoglu C, Miller A. Flexible endoscopy in the management of patients undergoing Roux-en-Y gastric bypass. Obes Surg. 2002;12:634–8.
Tashiro A, Sano M, Kinameri K, et al. Comparing mass screening techniques for gastric cancer in Japan. World J Gastroenterol WJG. 2006;12(30):4873–4.
Choi KS, Jun JK, Lee HY, et al. Performance of gastric cancer screening by endoscopy testing through the National Cancer Screening Program of Korea. Cancer Sci. 2011;102(8):1559–64.
Corsini DA, Simoneti CA, Moreira G, et al. Cancer in the excluded stomach 4 years after gastric bypass. Obes Surg. 2006;16:932–4.
Escalona A, Guzman S, Ibanez L, et al. Gastric cancer after Roux-en-Y gastric bypass. Obes Surg. 2005;15:423–7.
Harper JL, Beech D, Tichansky DS, et al. Cancer in the bypassed stomach presenting early after gastric bypass. Obes Surg. 2007;17:1268–71.
Raijman I, Strother SV, Donegan WL. Gastric cancer after gastric bypass for obesity. Case report. J Clin Gastroenterol. 1991;13:191–4.
Escalona A, Guzm ∼ in S, Ib ∼ ifiez L. Gastric cancer after Roux-en-Y gastric bypass. Obes Surg. 2005;15:423–7.
Lord RV, Edwards PD, Coleman MJ. Gastric cancer in the bypassed segment after operation for morbid obesity. Aust NZ J Surg. 1997;67:580–2.
Khitin L, Roses R, Birkett D. Cancer in the gastric remnant after gastric bypass. Curr Surg. 2003;60:521–3.
Mong C, Van Dam J, Morton J, et al. Preoperative endoscopic screening for laparoscopic Roux-en-Y gastric bypass has a low yield for anatomic findings. Obes Surg. 2008;18(9):1067–73.
Erim T, Cruz-Correa MR, Szomstein S, et al. Prevalence of Helicobacter pylori seropositivity among patients undergoing bariatric surgery: a preliminary study. World J Surg. 2008;32:2021–5.
Verma S, Sharma D, Kanwar P, et al. Prevalence of Helicobacter pylori infection in bariatric patients: a histologic assessment. Surg Obes Relat Dis. 2013;9:679–85.
Azagury D, Dumonceau JM, Morel P, et al. Preoperative work-up in asymptomatic patients undergoing Roux-en-Y gastric bypass: is endoscopy mandatory? Obes Surg. 2006;16:1304–11.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent Statement
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lee, J., Wong, S.KH., Liu, S.YW. et al. Is Preoperative Upper Gastrointestinal Endoscopy in Obese Patients Undergoing Bariatric Surgery Mandatory? An Asian Perspective. OBES SURG 27, 44–50 (2017). https://doi.org/10.1007/s11695-016-2243-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-016-2243-8