
Abstract
Purpose
To address the current lack of information about work-related factors for individuals with whiplash-associated disorders (WAD) we investigated the effectiveness of 3 months of neck-specific rehabilitation with internet support in combination with four physiotherapy visits (NSEIT) compared to the same exercises performed twice a week (24 times) at a physiotherapy clinic (NSE).
Methods
This is a prospective, multicentre, randomised controlled trial regarding secondary outcomes of work-related factors in 140 individuals with chronic moderate/severe WAD with 3- and 15-month follow-up.
Results
There were no group differences between NSE and NSEIT in the Work Ability Scale or work subscales of the Neck Disability Index, Whiplash Disability Questionnaire or Fear Avoidance Beliefs Questionnaire (FABQ-work). Both groups improved in all work-related outcome measures, except for FABQ-work after the 3-month intervention and results were maintained at the 15-month follow-up. Conclusions: Despite fewer physiotherapy visits for the NSEIT group, there were no group differences between NSEIT and NSE, with improvements in most work-related measures maintained at the 15-month follow-up. The results of the present study are promising for those with remaining work ability problems after a whiplash injury.
Protocol registered before data collection started: clinicaltrials.gov NCT03022812.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Whiplash-associated disorders (WAD) after e.g., a car crash is common, with a cumulative annual incidence as high as 600 per 100,000 inhabitants [1]. About half of car crash victims affected by a whiplash trauma experience chronic and disabling WAD [2, 3], with frequent and intense pain, slee** problems, and reduced health and societal participation. A high cost following WAD is frequently reported [3], mainly due to reduced ability to work compared to before the car crash. Those with WAD are less likely to return to work than those with other musculoskeletal injuries [4] and reduced ability to work is a commonly identified problem in individuals with WAD [5]. It has been recommended that work functioning should be part of a core outcome set for clinical trials involving WAD [6], something that has scarcely been evaluated in chronic moderate/ severe WAD after an exercise intervention [7, 8]. Being able to work has been shown to be important for general health [9,10,11], but work ability is also important for maintaining treatment gains in physical and psychological outcome measures [12], is thus of utmost importance to investigate after treatment.
The treatment evidence for WAD is inconclusive [13,14,15]. However, neck-specific exercises for those with moderate/severe chronic disabling WAD have seldom been evaluated [15, 16]. In a randomised controlled trial (RCT) of individuals with moderate/severe chronic WAD, neck-specific exercises have shown good and superior results to general physical activity regarding pain, function and work ability [7, 17]. However, the number of physiotherapy visits was extensive (twice a week for three months; 24 visits altogether). More efficient, flexible ways of delivering neck-specific exercises with fewer visits are needed, especially for working individuals. E-health solutions have previously been shown to be effective for other musculoskeletal conditions [18,19,20,21]. Recently, the main results of our RCT regarding internet support for rehabilitation in chronic WAD was published [22] showing improvements over time regarding pain and disability. However, work-related factors were not presented.
The aim of this prospective, multicentre RCT was to compare the effects of an Internet-based, neck-specific rehabilitation programme in combination with four physiotherapy visits (NSEIT) to the same rehabilitation programme performed at a physiotherapy clinic (NSE) twice a week for three months (24 visits) regarding the work-related secondary outcomes of the RCT. The hypothesis was that there should be no group differences and that both groups will improve.
Material and Methods
Design
This is a prospective, multicentre, randomised controlled trial [22, 23] with investigators blinded for randomisation. The trial interventions were delivered by 57 physiotherapists in a primary healthcare setting or working in private outpatient practice in ten county councils in Sweden. It compares two different ways of distributing neck-specific rehabilitation programme: NSEIT or NSE to 140 individuals with chronic WAD. Measurements were made at baseline, 3 months (end of treatment), and 15 months (12 months after the end of the intervention) and include ratings of work-related factors. The study was approved by the regional ethics committee in Linkö**, Sweden (2016/135-31) [23] (ClinicalTrials.gov; NCT03022812). Data were collected between 6 April 2017 and 15 September 2020.
Randomisation
A computerized block randomisation list stratified by gender was used for randomisation into two groups, NSEIT or NSE, with 70 individuals per group [22, 23].
Study Criteria for Participation
Information about the study was made available by healthcare providers and through advertising in newspapers, on posters, social media, and the university’s website. Interested individuals contacted the research team through the website. Study criteria was ensured through several steps: brief survey, telephone interview and physical examination [22, 23] before inclusion. Baseline measurements were completed before inclusion [22, 23].
Inclusion criteria [22, 23]: Individuals with a whiplash injury from a traffic accident involving a four-wheeled motor vehicle at least 6 months but less than 5 years previously with chronic neck problems corresponding to WAD grades II–III [24] verified by clinical examination. Additional inclusion criteria were: neck symptoms within the first week after the injury, average estimated pain in the previous week of at least 20 mm on the visual analogue scale (VAS) [25], neck disability of more than 20% on the Neck Disability Index (NDI) [26], being of working age (18–63 years), having daily access to a computer/tablet/smartphone and the Internet and sufficient self-estimated time to follow the treatment programme [22, 23].
Exclusion criteria [22, 23]: Individuals with signs of head injury at the time of whiplash injury were excluded. Additional exclusion criteria were: previous fractures or dislocation of the cervical column; known or suspected serious physical pathology; previous severe neck problems that resulted in sick leave of more than 1 month during the year before the current whiplash injury; surgery in the cervical column; generalised or more dominant pain elsewhere in the body; other illness/injury that may prevent full participation in the study; inability to understand and write in Swedish; diagnosed severe mental illness, such as psychosis, schizophrenia, or personality disorders; current alcohol or drug abuse [22, 23]; participation in neck-specific exercises in an earlier research study [7, 17].
Participants
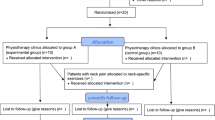
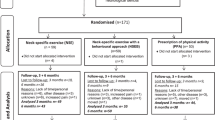
A total of 140 participants, 70 in each group, participated in the study (Fig. 1). They had a mean age of 40.5 years (SD ± 11.5), 79% were women, and they had a mean duration of WAD of 26 months (SD ± 16.8) (Table 1). Most participants were full-time or part-time workers (81%) or students (11%) (Table 1).

The consort flow diagram
Interventions
Both groups performed neck-specific rehabilitation programme for 12 weeks: NSEIT (Internet-based support exercises in combination with four visits to the physiotherapist) or NSE (exercises at a physiotherapy clinic twice/week) [22, 23]. Details of the rehabilitation programme and the education of physiotherapists are described elsewhere [22, 23]. The same physiotherapist could do both interventions.
NSEIT
The participants underwent a 12-week neck-specific rehabilitation programme that included only four visits to the physiotherapist. The exercises were performed and most of the information was given with the help of a non-interactive Internet support outside the healthcare system [22, 23]. With minor adjustments, these exercises had been used with good results in a previous RCT [7, 17] (DOI https://doi.org/https://doi.org/10.3384/report.diva-113,865).
NSE
In the NSE group, participants received the same information and neck-specific rehabilitation program as the NSEIT group but delivered by a physiotherapist [22, 23]. The participants had a total of 24 visits with the physiotherapist (twice a week for 12 weeks). The individuals also performed the exercises at home.
Outcome Measures
The collected background data included: age; sex; marital status; WAD grade; previous treatment for WAD; symptom duration; educational level; occupational classification (“Standard for Swedish work classification” SSY code [27]); NDI [26]; Whiplash Disability Questionnaire (WDQ) [28,29,30]; pain intensity [25]; self-assessment of sick leave; sickness presence (working despite pain; Stanford presenteeism scale) [31]; and Fear-Avoidance Beliefs Questionnaire (FABQ) [32, 33] (Table 1).
Primary outcome measure in the present paper: The Work Ability Score (WAS) [34], also named the single item (question number 1 in the Work Ability Index). In the WAS, present work ability is compared to lifetime best. It is well validated and has a scoring range of 0–10 points, with higher scores indicating greater work ability [34].
Secondary outcome measures in the present paper: neck-related function as measured by the NDI (measures the degree of perceived pain or disability status based on daily activities and underlying neck pain) question 7 regarding work (0 = I can do as much work as I want to/ no disability, 5 = I cannot do any work at all/ worst possible disability) [26] and WDQ (provide information on the impact that the WAD has upon lifestyle) question 3 regarding impact on work “Do your whiplash symptoms interfere with your work/home/study duties?” (0 = not at all/ no disability, 10 = unable to perform/worst possible disability) [28,29,30]. FABQ-work investigates fear-avoidance beliefs in a clinical setting and is the second of two FABQ subscales (work items 6–16, but only summarizing the score of items 6, 7, 9, 10, 11, 12, and 15) as follows: My pain was caused by my work or by an accident at work; My work aggravates my pain; My work is too heavy for me; My work makes or would make my pain worse; My work might harm my neck; I should not do my normal work with my present pain; I do not think that I will be back to my normal work within three months (0 = completely disagree, 6 = completely agree, with a maximum of 42 points indicating severe fear-avoidance beliefs) [32, 33].
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows (Version 28.0. Armonk, NY: IBM Corp). Participants’ characteristics, background data, and estimates of outcome measures at baseline are presented for NSEIT and NSE in Table 1. Frequencies and percentages are presented for binary and other categorical variables and means with standard deviations for all numerical discrete and continuous variables.
A mixed design ANOVA (3 time points × 2 treatment groups) was used to analyse within-group changes between time points (baseline, 3 months, and 15 months follow-up) and between-group differences at each time point, as well as changes between time points in all work-related outcome factors: WAS, NDI work (Sect. 7), WDQ Impact on work (question 3), and FABQ-work. The mixed design ANOVA was used under the assumption that outcome data was multivariate and normally distributed, and that any missing data was missing at random. Mauchly’s test of sphericity was used to test the assumption of sphericity in repeated measures. If this assumption was violated (p < 0.05), the Greenhouse–Geisser corrected epsilon was used. The Bonferroni correction was used for all pairwise contrasts: change baseline to 3 months, change baseline to 15 months, and change 3 to 15 months. All effects were reported as significant at p < 0.05. Partial eta squared (ηp2) was reported as a measure of effect size; 0.01 indicates a small effect, 0.06 indicates an intermediate effect, and 0.14 indicates a large effect [35]. The results of the mixed design ANOVAs are presented in Table 2.
We performed a response analysis based on complete responders in WAS at all three time points; complete responders (NSEIT, n = 55; NSE, n = 57) versus non-complete responders (NSEIT, n = 15; NSE, n = 13). There was a significant difference (p = 0.002) between complete responders and non-complete responders regarding age, with non-complete responders in both treatment groups being younger. However, age was not correlated to change in any of the work-related outcome factors (Pearson correlation coefficient between 0.02 and 0.11).
Results
Primary Outcome Measure
There was no significant interaction effect of time by treatment group of WAS (Table 2, Fig. 2). There was a significant main effect of WAS over time (whole group [F(1.8, 220) = 16.6, p < 0.001, ηp2 = 0.13]; NSEIT [F(2, 109) = 5.7, p = 0.04, ηp2 = 0.10], NSE [F(2, 109) = 8.5, p < 0.001, ηp2 = 0.14]). The pairwise contrasts showed significant within-group effects, between baseline and 3 months follow-up as well as between baseline and 15 months follow-up, in both NSEIT and NSE (Table 2, Fig. 2).

Outcome of Work-Ability Score (WAS) at baseline and at 3 and 15 month follow-up for both intervention groups
Secondary Outcome Measures
There was no significant interaction effect of time by treatment group of NDI work (Table 2). There was a significant main effect of NDI work over time (whole group [F(1.8, 202.9) = 30.7, p < 0.001, ηp2 = 0.22]; NSEIT [F(2, 109) = 15.8, p < 0.001, ηp2 = 0.23], NSE [F(2, 109) = 8.5, p < 0.001, ηp2 = 0.20]). The pairwise contrasts showed significant within-group effects, between baseline and 3 months follow-up as well as between baseline and 15 months follow-up, in both NSEIT and NSE (Table 2).
There was no significant interaction effect of time by treatment group of WDQ work (Table 2). There was a significant main effect of WDQ impact on work over time (whole group [F(2, 220) = 42.8, p < 0.001, ηp2 = 0.28]; NSEIT [F(2, 109) = 19.9, p < 0.001, ηp2 = 0.27], NSE [F(2, 109) = 18.2, p < 0.001, ηp2 = 0.25]). The pairwise contrasts showed significant within-group effects, between baseline and 3 months follow-up as well as between baseline and 15 months follow-up, in both NSEIT and NSE (Table 2).
There was no significant interaction effect of time by treatment group of FABQ-work (Table 2). There was a significant main effect of FABQ-work over time for the whole group, but not when divided by treatment group (whole group [F(2, 214) = 4.7, p = 0.01, ηp2 = 0.04]; NSEIT [F(2, 106) = 2.9, p = 0.06, ηp2 = 0.05], NSE [F(2, 109) = 8.5, p = 0.20, ηp2 = 0.03]).
Exercise Fulfilment
The participants’ self-reported compliance with exercise was higher in the NSE group (94%) than in the NSEIT group (75%, p = 0.006) during the 12-week intervention period.
Discussion
The aim of the prospective, multicentre RCT was to compare the effects of NSEIT to NSE and in this article we describe the secondary outcomes of the RCT concerning work-related factors [22, 23]. Both groups improved in all work-related outcome measures, except for FABQ-work after the 3-month intervention, and results were maintained at the 15-month follow-up. This is confirming our hypothesis that NSEIT is as effective as NSE, but with fewer physiotherapy visits.
This is the first study [22, 23] investigating whether NSEIT is as effective as NSE, and in this paper we present the work-related outcomes. This makes the study unique and novel and is in line with the digitalization occurring throughout global society, responding to the need for increased flexibility, availability, patient independence, and reduced healthcare costs.
There is to our knowledge no quantitative study presenting the outcomes of Internet-delivered treatment investigating chronic WAD, severe WAD, and exercise for work-related factors in WAD. Bring et al. [18] reported that an Internet-delivered behavioural programme was as effective as clinic-based face-to-face therapy sessions in terms of psychosocial factors and that both interventions were superior to self-care instructions for individuals with mild/ moderate acute WAD. This is in line with the present results. The results are also in line with results from other studies showing E-health solutions to be effective for musculoskeletal conditions such as chronic back pain, knee osteoarthritis, total knee arthroplasty, rheumatoid arthritis, and vestibular rehabilitation, as well as other conditions [19, 21, 36,37,38], although work-related factors were not investigated in these studies.
According to Lelieveld et al. [39], an Internet-based programme should preferably be combined with a few visits to the caregiver. The authors strongly believe that the addition to the Internet-based programme of the four physiotherapy visits for an introduction, support, and to check that the exercises have been correctly performed was of great importance for the patient to feel safe, reassured, and motivated. However, this hypothesis needs to be investigated in future qualitative studies. The fact that both groups improved over time also confirms our earlier favourable results for NSE from two RCTs in which the same programme, although not an E-health solution, was used for chronic WAD patients [7, 17, 40]. Ferreira et al. [41] reported that freely accessible websites offering treatment recommendations for low back pain are mostly inaccurate, and this may also be the case for neck pain. Internet-based recommendations for treatment must be based on research, as in the present study.
As shown in our earlier RCT [7] where neck-specific exercise in combination with a behavioural approach had better outcome in work ability than only neck-specific exercises, the authors believe that the elements of behavioural components in the NSEIT/NSE in addition to the exercises were of importance to motivate and help the participants feel safe and reassured. Both groups improved over time and, except for FABQ-work, showed intermediate to large effect sizes. This is in contrast to the findings of a meta-analysis of exercise for the management of neck pain, including WAD, which showed significant improvements but small effect sizes [42]. As the present population has chronic moderate/severe WAD, which is generally recognized as difficult to treat with no spontaneous recovery to be expected after the first six months, these are especially promising results. In addition, the good results were maintained. Other interventions, such as ergonomic interventions, have not shown convincing results in preventing work disability [43].
In this study there was a small effect-size of improvement for FABQ-work, which may be explained by the fact that the participants already scored low values/low fear at baseline. This gave limited room for improvement, although they did close to significantly improve in the NSEIT group at 15-month follow-up.
Within-group changes of WAS were 0.6 to 1.0 from baseline to 15-month follow-up in NSEIT/NSE in the present study. For low back pain, improvements of 1.5 were interpreted as clinically important [44]. Clinically relevant improvement data is yet unavailable for WAS and the chronic WAD population and needs to be investigated in a future study. For this reason, we cannot comment on whether the improvement in the current study was clinically relevant or not.
Work ability measured with WAS, the main outcome in the present study, is a broader concept than work capacity, return to work or being on sick leave. Work ability has been variously defined, e.g., in the work ability house model [45], as the balance between work and individual resources. As the social insurance system differs between countries, work ability and not sick leave may be a preferred outcome. Although it is influenced by individual resources and working conditions, which need to be understood by healthcare professionals [8]. The results of a meta-analysis show that half of those with WAD who return to work display reduced work ability [46]. This may lead to presenteeism or to choose to remain outside the insurance medical system, being dependence to relatives. There are only a few studies, mostly cross-sectional, regarding ability to work in WAD patients, and they use different measures [11]. Apart from our previous RCT [7], showing neck-specific exercises to be superior to prescribed physical activity, there is to our knowledge no RCT of merely physical interventions in chronic WAD that investigates work ability as an outcome measure. This strengthens the importance and scientific contribution of the present study. Work is important across a broad range of aspects, including social roles, socialisation, context, status, and general health, and not only from an economic perspective [47, 48]. Thus, it is important to investigate work as an outcome after interventions [6, 9,10,11].
Strengths and Weaknesses of the Study
A strength of the present study was that it is a randomised controlled multicentre trial including individuals with chronic moderate/severe WAD often being excluded in rehabilitation studies. Another strength is that the good results were not only observed after the 3-month intervention period but were also maintained at the 15-month follow-up. This confirms the results of the previously presented main outcome of pain and neck-specific disability [22]. Apart from the study by Bring et al. [18], which did include acute WAD, there is to our knowledge no quantitative study presenting the outcomes of Internet-delivered treatment for neck pain, and the present study is the only one investigating chronic WAD, severe WAD, and exercise, for work-related factors in WAD.
The present study is a multicentre study involving treating physiotherapists in several units across a large geographical area, which is a risk due to having less control over treatments. However, the physiotherapists were well trained by the project team, they received carefully written, oral, and practical introductions and were free to contact the project leaders for support when needed. The advantage of a multicentre study may be that the study improved reproducibility, generalisability and potential clinical translation of the RCT. The participants themselves expressed their interest in participating in the RCT after seeing an advertisement for the RCT in various media. Prior to inclusion in the study, the criteria for participation were ensured, where the interviewer asked, among other things, whether the potential participant was prepared to carry out the program [22, 23]. This can lead to the results not being transferable to patients in ordinary healthcare and must be investigated in an implementation study without strict RCT criteria.
Individuals who were not able to read/write Swedish and thus unable to understand the information provided or answer the questionnaires were excluded, which makes it less generalizable to the whole population. However, in the future, the Internet-based programme can be translated into other languages, increasing the availability of this healthcare intervention for the whole population.
The power of the present article was counted on the main outcome in the RCT [22, 23]: the NDI, and not on work-related secondary outcomes. Nevertheless, the results of the main outcome and the work-related secondary outcomes support each other, with an improvement over time in both groups but without significant group differences. As clinically relevant improvement data was unavailable for the present outcomes and the chronic WAD population, non-inferiority analyses were not performed, as previously reported for the main outcome RCT data [22]. As previous RCTs conducted by our research team have shown three months of NSE to be cost-effective and superior to remaining on a waiting list or receiving prescribed general physical activity [7, 17, 40], we did not include a control group without specific treatment in the present RCT as it would have been unethical.
Implications for Practice
In individuals with non-specific neck pain, neck strengthening exercises or increased physical activity have shown good results in work-related outcomes [43, 49]. In the present study, neck-specific exercise was tolerated with good results, without group differences and without adverse events [22], showing that NSEIT is as effective as NSE in improving and maintaining work ability for individuals with chronic WAD, but with fewer physiotherapy visits (four compared to 24 visits). As shown in our qualitative study, participating in this neck-specific exercise programme, including being acknowledged and receiving information about WAD, affected the individuals’ work ability [8]. The present study may help to provide evidence of treatment efficacy for patients with WAD and may help to optimize treatment plans for individuals with WAD. However, it is worth noticing that the results are presented at a group level and that NSEIT or NSE may not suit everyone, and for some individuals NSE may be preferred despite the large number of physiotherapy visits. Support for work participation for individuals with chronic WAD can be strengthened.
Conclusion
One can conclude that, despite fewer physiotherapy visits, there were no group differences between NSEIT and NSE, with improvements in most work-related measures maintained at the 15-month follow-up. FABQ-work was close to significant in the NSEIT group at the 15-month follow-up. Thus, we accept the study hypothesis. The result of the present study may be promising for those with impaired work ability after a whiplash injury, although may not be generalisable to all individuals with WAD. More studies regarding rehabilitation for improved work ability are needed to optimize care, especially for those with chronic WAD. To achieve even higher effect sizes, NSE/NSEIT could be combined with rehabilitation, focusing on the work situation and factors improving work ability within a broad but individual context.
Data Availability
Data contains information regarding health and will not be available, due to the Swedish Health Secrets Act, without specific ethical permission.
Code Availability
IBM SPSS version 28 was used for statistical analyses.
References
Holm LW, Carroll LJ, Cassidy JD, Hogg-Johnson S, Côté P, Guzman J, et al. The burden and determinants of neck pain in whiplash-associated disorders after traffic collisions: results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine. 2008;33:S52-S59.
Styrke J, Sojka P, Bjornstig U, Stalnacke BM. Symptoms, disabilities, and life satisfaction five years after whiplash injuries. Scand J Pain. 2014;5(4):229–236.
Pink J, Petrou S, Williamson E, Williams M, Lamb SE. Economic and health-related quality of life outcomes of whiplash associated disorders. Spine. 2016;41:1378–1386.
Biering-Sørensen Møller A, Stoltenberg CDG, Holm JW, Skov PD. The return-to-work process of individuals sick-listed because of whiplash-associated disorder: a three-year follow-up study in a Danish cohort of long-term sickness absence. BMC Public Health. 2014;14:113.
Hoving JL, O’Leary EF, Niere KR, Green S, Buchbinder R. Validity of the neck disability index, Northwick Park Neck Pain Questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders. Pain. 2003;102:273–281.
Chen K, Andersen T, Carroll L, Connelly L, Côte P, Curatolo M, et al. Recommendations for core outcome domain set for whiplash-associated disorders (CATWAD). Clin J Pain. 2019;35:727–736.
Lo HK, Johnston V, Landén Ludvigsson M, Peterson G, Overmeer T, David M, et al. Factors associated with work ability following exercise interventions for people with chronic whiplash-associated disorders: secondary analysis of a randomized controlled trial. J Rehabil Med. 2018;50(9):828–836.
Peolsson A, Hermansen A, Peterson G, Nilsing SE. Return to work a bumpy road: a qualitative study on experience of work ability and work situation in individuals with chronic whiplash-associated disorders. BMC Public Health. 2021;21:785.
Waddell G, Burton AK. Is work good for your health and well-being? Department of Work and Pensions: London, UK. https://www.gov.uk/government/publications/is-work-good-for-your-health-and-well-being. Accessed 10 Mar 2022.
Norström F, Virtanen P, Hammarström A, Gustafsson PE, Janlert U. How does unemployment affect self-assessed health? A systematic review focusing on subgroup effects. BMC Public Health. 2014;14:310.
Gane EM, Plinsinga ML, Brakenridge CL, Smits EJ, Aplin T, Johnston V. The impact of musculoskeletal injuries sustained in road traffic crashes on work-related outcomes: a systematic review. Int J Environ Res Public Health. 2021;18:11504.
Sullivan M, Adams H, Thibault P, Moore E, Carriere JS, Larivière C. Return to work helps maintain treatment gains in the rehabilitation of whiplash injury. Pain. 2017;158:980–987.
Verhagen AP, Scholten-Peeters GGGM, van Wijngaarden S, de Bie R, Bierma-Zeinstra SMA. Conservative treatments for whiplash. Cochrane Database Syst Rev. 2007. https://doi.org/10.1002/14651858.CD003338.pub3.
Rushton A, Wright C, Heneghan N, Eveleigh G, Calvert M, Freemantle N. Physiotherapy rehabilitation for whiplash associated disorder II: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2011;1: e000265.
Rebbeck T. The role of exercise and patient education in the noninvasive management of whiplash. J Orthop Sports Phys Ther. 2017;47:481–491.
Gross AR, Paquin JP, Dupont G, Blanchette S, Lalonde P, Cristie T, et al. Exercises for mechanical neck disorders: a Cochrane review update. Man Ther. 2016;24:25–45.
Ludvigsson ML, Peterson G, Peolsson A. Neck-specific exercise for radiating pain and neurological deficits in chronic whiplash: a 1-year follow-up of a randomised clinical trial. Sci Rep. 2020;10:6758.
Bring A, Åsenlöf P, Söderlund A. What is the comparative effectiveness of current standard treatment, against an individually tailored behavioural programme delivered either on the Internet or face-to-face for people with acute whiplash associated disorder? A randomized controlled trial. Clin Rehabil. 2015;30:441–453.
Garg S, Garg D, Turin TC, Chowdhury MF. Web-based interventions for chronic back pain: a systematic review. J Med Internet Res. 2016;18: e139.
Schafer AGM, Zalpour C, von Piekartz H, Hall TM, Paelke V. The efficacy of electronic health-supported home exercise interventions for patients with osteoarthritis of the knee: systematic review. J Med Internet Res. 2018;20: e152.
van Vugt VA, de Kruif AJ, van der Wouden JC, van der Horst HE, Maarsingh OR. Experiences of patients and physiotherapists with blended internet-based vestibular rehabilitation: a qualitative interview study. BJGP Open. 2020;4:1–10.
Peterson G, Peolsson A. Efficacy of neck-specific exercise with internet support versus neck-specific exercise at a physiotherapy clinic in chronic whiplash-associated disorders multicenter randomized controlled noninferiority trial. J Med Internet Res. 2023;25(e43888):p1-15.
Peolsson A, Landén Ludvigsson M, Peterson G. Neck-specific exercises with internet-based support compared to neck-specific exercises at a physiotherapy clinic for chronic whiplash-associated disorders: study protocol of a randomized controlled multicentre trial. BMC Musculoskelet Disord. 2017;18:524.
Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, et al. Scientific monograph of the Quebec task force on whiplash associated disorders: redefining “whiplash” and its management. Spine. 1995;20:S1-S73.
Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983;16:87–101.
Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manip Physiol Ther. 1991;14:409–415.
Statistics Sweden (SCB) SSYK 2012 Standard för svensk yrkesklassificering. 2012. http://www.scb.se/statistik/_publikationer/OV9999_2012A01_BR_ X70BR1201.pdf (In Swedish). (Developed from the ISCO-08 (International Standard Classification of Occupation 2008 http://www.ilo.org/public/english/bureau/stat/isco/isco88/index.htm)
Willis C, Niere KR, Hoving JL, Green S, O’Leary EF, Buchbinder R. Reproducibility and responsiveness of the whiplash disability questionnaire. Pain. 2004;110:681–688.
Pinfold M, Niere KR, O’Leary EF, Hoving JL, Green S, Buchbinder R. Validity and internal consistency of a whiplash-specific disability measure. Spine. 2004;29:263–268.
Stupar M, Côté P, Beaton DE, Boyle E, Cassidy JD. A test-retest reliability study of the whiplash disability questionnaire in patients with acute whiplash-associated disorders. J Manip Physiol Ther. 2015;38:629–636.
Koopman C, Pelletier KR, Murray JF, Sharda CE, Berger ML, Turpin RS. Stanford presenteeism scale: health status and employee productivity. J Occup Environ Med. 2002;44:14–20.
Waddell G, Newton M, Henderson I, Somerville D, Main CJ, Slade PD, et al. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52:157–168.
Dedering A, Borjesson T. Assessing fear-avoidance beliefs in patients with cervical radiculopathy. Physiother Res Int. 2013;18:193–202.
El Fassi M, Bocquet V, Majery N, Lair ML, Couffignal S, Mairiaux P. Work ability assessment in a worker population: comparison and determinants of Work Ability Index and Work Ability Score. BMC Public Health. 2013;13:305.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Erlbaum; 1988.
Riva S, Camerini A-L, Allam A, Schultz PJ. Interactive sections of an Internet-based intervention increase empowerment of chronic back pain patients: randomized controlled trial. Internet Res. 2014;16: e180.
Revenäs Å, Opava C, Ahlén H, Brusewitz M, Pettersson S, Åsenlöf P. Mobile internet service for self-management of physical activity in people with rheumatoid arthritis: evaluation of test version. RMD Open. 2016;2: e000214.
Shukla H, Nair SR, Thakker D. Role of telerehabilitation in patients following total knee arthroplasty: evidence from a systematic literature review and meta-analysis. J Telemed Telecare. 2017;23:339–346.
Lelieveld O, Armbrust W, Geertzen J, de Graaf I, van Leeuwen MA, Sauer PJ, et al. Promoting physical activity in children with juvenile idiopathic arthritis through an internet-based program: results of a pilot randomized controlled trial. Arthritis Care Res. 2010;62:697–703.
Peolsson A, Landén Ludvigsson M, Tigerfors AM, Peterson G. Effects of neck-specific exercises compared to waiting list for individuals with chronic whiplash-associated disorders: a prospective, randomized controlled study. Arch Phys Med Rehabil. 2016;97:189–195.
Ferreira G, Traeger AC, Machado G, O’Keeffe M, Maher CG. Credibility, accuracy, and comprehensiveness of Internet-based information about low back pain: a systematic review. J Med Internet Res. 2019;21: e13357.
Southerst D, Nordin MC, Côte P, Shearer HM, Varatharajan S, Yu H, et al. Is exercise effective for the management of neck pain and associated disorders or whiplash-associated disorders?: a systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) collaboration. Spine J. 2016;16:1503–1523.
Varatharajan SJ, Côte P, Shearer HM, Loisel P, Wong JJ, Southerest D, et al. Are work disability prevention interventions effective for the management of neck pain or upper extremity disorders? A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMA) collaboration. J Occup Rehabil. 2014;24:692–708.
Boekel I, Dutmer AL, Schiphorst Preuper HR, Reneman MF. Validation of the work ability index-single item and the Pain Disability Index-work item in patients with chronic low back pain. Eur Spine J. 2022;31:943–952.
Ilmarinen J. From work ability to research implementation. IJERPH. 2019;16:2882.
Kamper SJ, Rebbeck TJ, Maher CG, McAuley JH, Sterling M. Course and prognostic factors of whiplash: a systematic review and meta-analysis. Pain. 2008;138:617–629.
Gebel M, Voβemer J. The impact of employment transitions on health in Germany: a difference-in-difference propensity score matching approach. Soc Sci Med. 2014;108:128–136.
Gnambs T, Stigbauer B, Selenko E. Psychological effects of (non)employment: a cross-national comparison of the United States and Japan. Scand J Psychol. 2015;56:659–669.
Louw S, Makwela S, Manas L, Meyer L, Terblanche D, Brink Y. Effectiveness of exercise in office workers with neck pain: a systematic review and meta-analysis. South African J Physiother. 2017;73: e392.
Funding
Open access funding provided by Linkö** University. Funding was received in competition and paid to the Department of Health, Medicine and Caring Sciences, Linkö** University or to the Centre for Clinical Research Sörmland, Uppsala University. The authors acknowledge financial support from the Swedish Research Council, the Swedish Innovation Agency, the Medical Research Council of Southeast Sweden, and the county councils of Östergötland and Sörmland.
Author information
Authors and Affiliations
Contributions
AP and GP initiated the study and were responsible for the overall design. ENS is an expert in her fields and critically discussed the work-related questionnaires with AP and GP. AP and GP had the responsibility for funding. AP and GP were mainly responsible for data collection. ENS was a test-leader and study coordinator in one of the county councils involved. Data analysis was performed by AP in dialogue with the university statistician. AP wrote the manuscript in dialogue with GP and ENS. All authors read, revised, and approved the final version.
Corresponding author
Ethics declarations
Conflict of interests
No conflicts of interest/ competing interests are reported for the present study. The manuscript does not contain any information about medical device(s)/drug(s).
Ethical Approval
The study was approved by the regional ethics committee in Linkö**, Sweden (2016/135–31).
Consent to Participate
Patients were included after providing oral and written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Peolsson, A., Nilsing Strid, E. & Peterson, G. Novel Internet Support for Neck-Specific Rehabilitation Improves Work-Related Outcomes to the Same Extent as Extensive Visits to a Physiotherapy Clinic in Individuals with Chronic Whiplash-Associated Disorders: A Prospective Randomised Study. J Occup Rehabil (2024). https://doi.org/10.1007/s10926-024-10176-0
Accepted:
Published:
DOI: https://doi.org/10.1007/s10926-024-10176-0