
Abstract
Background
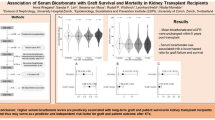
Metabolic acidosis is a risk factor for faster kidney function decline in chronic kidney disease (CKD) and in adult kidney transplant recipients (KTRs). We hypothesized that metabolic acidosis would be highly prevalent and associated with worse allograft function in pediatric KTRs.
Methods
Pediatric KTRs at Montefiore Medical Center from 2010 to 2018 were included. Metabolic acidosis was defined as serum bicarbonate < 22 mEq/L or receiving alkali therapy. Regression models were adjusted for demographic factors and donor/recipient characteristics.
Results
Sixty-three patients were identified with a median age at transplant of 10.5 (interquartile range (IQR) 4.4–15.2) years and post-transplant follow-up of 3 (IQR 1–5) years. Baseline serum bicarbonate was 21.7 ± 2.4 mEq/L, serum bicarbonate < 22 mEq/L was present in 28 (44%), and 44% of all patients were receiving alkali therapy. The prevalence of acidosis ranged from 58 to 70% during the first year of follow-up. At baseline, each 1-year higher age at transplant and every 10 ml/min/1.73 m2 higher eGFR were associated with 0.16 mEq/L (95% CI: 0.03–0.3) and 0.24 mEq/L (95% CI: 0.01–0.5) higher serum bicarbonate, respectively. Older age at transplant was associated with lower odds of acidosis (OR: 0.84; 95% CI: 0.72–0.97). During follow-up, metabolic acidosis was independently associated with 8.2 ml/min/1.73 m2 (95% CI 4.4–12) lower eGFR compared to not having acidosis; furthermore, eGFR was significantly lower among KTRs with unresolved acidosis compared with resolved acidosis.
Conclusions
Among pediatric KTRs, metabolic acidosis was highly prevalent in the first year post-transplantation and was associated with lower eGFR during follow-up.
Graphical abstract
A higher resolution version of the Graphical abstract is available as Supplementary information





Similar content being viewed by others

Data availability
Due to concerns over maintenance of patient confidentiality, the dataset is not publicly available but may be available from the corresponding author on reasonable request.
References
Brown DD, Roem J, Ng DK, Reidy KJ, Kumar J, Abramowitz MK, Mak RH, Furth SL, Schwartz GJ, Warady BA, Kaskel FJ, Melamed ML (2020) Low serum bicarbonate and CKD progression in children. Clin J Am Soc Nephrol 15:755–765
Dobre M, Rahman M, Hostetter TH (2015) Current status of bicarbonate in CKD. J Am Soc Nephrol 26:515–523
Chen W, Levy DS, Abramowitz MK (2019) Acid base balance and progression of kidney disease. Semin Nephrol 39:406–417
de Brito-Ashurst I, Varagunam M, Raftery MJ, Yaqoob MM (2009) Bicarbonate supplementation slows progression of CKD and improves nutritional status. J Am Soc Nephrol 20:2075–2084
Ho JQ, Abramowitz MK (2022) Clinical consequences of metabolic acidosis-muscle. Adv Chronic Kidney Dis 29:395–405
Fernando ME, Jayanivash J, Srinivasaprasad ND, Suren S, Thirumalvalavan K (2019) Post-renal transplant metabolic acidosis: a neglected entity. Indian J Nephrol 29:116–121
Djamali A, Singh T, Melamed ML, Stein JH, Aziz F, Parajuli S, Mohamed M, Garg N, Mandelbrot D, Wesson DE, Astor BC (2019) Metabolic acidosis 1 year following kidney transplantation and subsequent cardiovascular events and mortality: an observational cohort study. Am J Kidney Dis 73:476–485
Park S, Kang E, Park S, Kim YC, Han SS, Ha J, Kim DK, Kim S, Park SK, Han DJ, Lim CS, Kim YS, Lee JP, Kim YH (2017) Metabolic acidosis and long-term clinical outcomes in kidney transplant recipients. J Am Soc Nephrol 28:1886–1897
Raphael KL, Shihab FS (2017) Acidosis and kidney allograft survival. J Am Soc Nephrol 28:1672–1674
Ritter A, Mohebbi N (2020) Causes and consequences of metabolic acidosis in patients after kidney transplantation. Kidney Blood Press Res 45:792–801
Schulte K, Puchel J, Schussel K, Borzikowsky C, Kunzendorf U, Feldkamp T (2019) Effect of sodium bicarbonate in kidney transplant recipients with chronic metabolic acidosis. Transplant Direct 5:e464
Skiba K, Gojowy D, Szotowska M, Bartmanska M, Kolonko A, Cierpka L, Wiecek A, Adamczak M (2018) Metabolic acidosis in kidney transplant recipients. Pol Arch Intern Med 128:587–593
Mathur V, Reaven NL, Funk SE, Tangri N (2022) Serum bicarbonate and graft and patient outcomes among kidney transplant recipients: a retrospective cohort study evaluating changes in serum bicarbonate over time. Kidney Med 5:100573
Keven K, Ozturk R, Sengul S, Kutlay S, Ergun I, Erturk S, Erbay B (2007) Renal tubular acidosis after kidney transplantation–incidence, risk factors and clinical implications. Nephrol Dial Transplant 22:906–910
Jerome Harambat KK, Azukaitis K, Bayazit AK, Canpolat N, Doyon A, Duzova A, Niemirska A (2017) Metabolic acidosis is common and associates with disease progression in children with chronic kidney disease. Kidney Int 92:1507–1514
Cho MH (2018) Pediatric kidney transplantation is different from adult kidney transplantation. Korean J Pediatr 61:205–209
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637
Chen W, Abramowitz MK (2014) Metabolic acidosis and the progression of chronic kidney disease. BMC Nephrol 15:55
Furth SL, Abraham AG, Jerry-Fluker J, Schwartz GJ, Benfield M, Kaskel F, Wong C, Mak RH, Moxey-Mims M, Warady BA (2011) Metabolic abnormalities, cardiovascular disease risk factors, and GFR decline in children with chronic kidney disease. Clin J Am Soc Nephrol 6:2132–2140
Alva S, Divyashree M, Kamath J, Prakash PS, Prakash KS (2020) A study on effect of bicarbonate supplementation on the progression of chronic kidney disease. Indian J Nephrol 30:91–97
Di Iorio BR, Bellasi A, Raphael KL, Santoro D, Aucella F, Garofano L, Ceccarelli M, Di Lullo L, Capolongo G, Di Iorio M, Guastaferro P, Capasso G, UBI Study Group (2019) Treatment of metabolic acidosis with sodium bicarbonate delays progression of chronic kidney disease: the UBI Study. J Nephrol 32:989–1001
Goraya N, Simoni J, Jo CH, Wesson DE (2014) Treatment of metabolic acidosis in patients with stage 3 chronic kidney disease with fruits and vegetables or oral bicarbonate reduces urine angiotensinogen and preserves glomerular filtration rate. Kidney Int 86:1031–1038
BiCARB Study Group (2020) Clinical and cost-effectiveness of oral sodium bicarbonate therapy for older patients with chronic kidney disease and low-grade acidosis (BiCARB): a pragmatic randomised, double-blind, placebo-controlled trial. BMC Med 18:91
Melamed ML, Horwitz EJ, Dobre MA, Abramowitz MK, Zhang L, Lo Y, Mitch WE, Hostetter TH (2020) Effects of sodium bicarbonate in CKD stages 3 and 4: a randomized, placebo-controlled, multicenter clinical trial. Am J Kidney Dis 75:225–234
Mariani LH, Martini S, Barisoni L, Canetta PA, Troost JP, Hodgin JB, Palmer M, Rosenberg AZ, Lemley KV, Chien HP, Zee J, Smith A, Appel GB, Trachtman H, Hewitt SM, Kretzler M, Bagnasco SM (2018) Interstitial fibrosis scored on whole-slide digital imaging of kidney biopsies is a predictor of outcome in proteinuric glomerulopathies. Nephrol Dial Transplant 33:310–318
Imenez Silva PH, Mohebbi N (2022) Kidney metabolism and acid-base control: back to the basics. Pflugers Arch 474:919–934
Noce A, Marrone G, Wilson Jones G, Di Lauro M, Pietroboni Zaitseva A, Ramadori L, Celotto R, Mitterhofer AP, Di Daniele N (2021) Nutritional approaches for the management of metabolic acidosis in chronic kidney disease. Nutrients 13:1–18
Rodig NM, McDermott KC, Schneider MF, Hotchkiss HM, Yadin O, Seikaly MG, Furth SL, Warady BA (2014) Growth in children with chronic kidney disease: a report from the Chronic Kidney Disease in Children Study. Pediatr Nephrol 29:1987–1995
Franke D, Thomas L, Steffens R, Pavičić L, Gellermann J, Froede K, Querfeld U, Haffner D, Živičnjak M (2015) Patterns of growth after kidney transplantation among children with ESRD. Clin J Am Soc Nephrol 10:127–134
Messa PG, Alfieri C, Vettoretti S (2016) Metabolic acidosis in renal transplantation: neglected but of potential clinical relevance. Nephrol Dial Transplant 31:730–736
Acknowledgements
The author SK would like to thank Drs. Frederick Kaskel and Dr. Michal Melamed as the research described was supported by the TL1DK136048 New York Consortium for Interdisciplinary Training on Kidney, Urological and Hematological Research (NYC Train KUHR) as well as by the NIH/National Center for Advancing Translational Science (NCATS) Einstein-Montefiore CTSA Grant Number 1UM1TR004400. KJR is supported by R01DK131811 and R01DK131176.
Funding
This study was funded by the TL1DK136048 New York Consortium for Interdisciplinary Training on Kidney, Urological and Hematological Research (NYC Train KUHR) and by the NIH/National Center for Advancing Translational Science (NCATS) Einstein-Montefiore CTSA Grant Number UL1TR001073.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the institutional review board for Montefiore Medical Center / Albert Einstein College of Medicine (IRB Number: 2021–13548).
Informed consent
The need for informed consent was waived due to the use of de-identified data.
Conflict of interest
Stella Kilduff has grant funding by TL1DK136048 and UL1TR001073. Author Kimberly Reidy has grants supported by R01DK131811 and R01DK131176. Dr. Kimberly Reidy is also a site investigator for Advicienne and Travere Therapeutics funded clinical trials that are unrelated to this manuscript. Authors Stella Kilduff, Nicole Hayde, Shankar Viswanathan, and Matthew Abramowitz declare that they have no conflicts of interest or disclosures.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kilduff, S., Hayde, N., Viswanathan, S. et al. Metabolic acidosis in pediatric kidney transplant recipients. Pediatr Nephrol 38, 4165–4173 (2023). https://doi.org/10.1007/s00467-023-06072-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-023-06072-z