
Abstract
Objectives
This study evaluated the association between aortic valve calcification (AVC) and aortic stenosis (AS) by scoring the AVC to determine the threshold scores for significant AS on non-electrocardiographic (ECG)–gated computed tomography (CT).
Methods
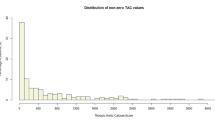
We retrospectively analyzed the AVC scores of 5385 patients on non-contrast non-ECG-gated CT, who underwent transthoracic echocardiography (TTE) from March 1, 2013, to December 26, 2019, at our institution. Multivariable logistic regression models were used to identify potential risk factors for significant AS. The thresholds for significant AS were computed using receiver operator characteristic (ROC) curves, based on the AVC scores after propensity score matching.
Results
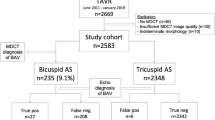
A significant association was found between AS and age (p < 0.001; odds ratio [OR], 1.04; 95% confidence interval [CI], 1.02–1.06), female sex (p < 0.001; OR, 4.5; 95% CI, 2.75–7.36), bicuspid aortic valve (p < 0.001; OR, 23.2; 95% CI, 7.35–72.9), and AVC score (AVC score/100) (p < 0.001; OR, 1.82; 95% CI, 1.71–1.95). All sex-specific AVC thresholds for significant AS (moderate and over AS severity, moderate and over AS severity without discordance, discordant severe AS, and concordant severe AS) showed high sensitivity and specificity (AUC, 0.939–0.968; sensitivity, 84.6–96%; specificity, 84.2–97.1%).
Conclusions
We determined the optimal AVC threshold scores for significant AS, which may aid in diagnosing significant asymptomatic AS on incidental detection of AVC through non-ECG-gated CT for non-cardiac indications.
Key Points
• Increased frequency of non-electrocardiographic (ECG)–gated computed tomography (CT) for non-cardiac indications has led to the increased incidental identification of aortic valve calcification (AVC).
• It is important to identify patients with significant aortic stenosis (AS) who require additional echocardiographic assessment on incidental detection of AVC via non-ECG-gated CT.
• We determined the AVC thresholds with high sensitivity and specificity to identify significant AS on non-ECG-gated CT, which could lead to early diagnosis of asymptomatic significant AS and improved prognosis.






Similar content being viewed by others

Abbreviations
- AS:
-
Aortic stenosis
- AU:
-
Arbitrary units
- AUC:
-
Area under the curve
- AVA:
-
Aortic valve area
- AVAi:
-
Aortic valve area indexed to the body surface area
- AVC:
-
Aortic valve calcification
- AVCi:
-
Aortic valve calcification indexed to the body surface area
- BAV:
-
Bicuspid aortic valve
- CI:
-
Confidence intervals
- CKD:
-
Chronic kidney disease
- CT:
-
Computed tomography
- ECG:
-
Electrocardiography
- EF:
-
Ejection fraction
- ICC:
-
Intraclass correlation coefficients
- MG:
-
Mean transvalvular gradient
- OR:
-
Odds ratios
- PSM:
-
Propensity score matching
- ROC:
-
Receiver operator characteristic
- SD:
-
Standard deviation
- TTE:
-
Transthoracic echocardiography
- VIF:
-
Variance inflation factor
- Vmax:
-
Peak aortic jet velocity
References
Dweck MR, Jones C, Joshi NV et al (2012) Assessment of valvular calcification and inflammation by positron emission tomography in patients with aortic stenosis. Circulation 125:76–86
Jenkins WS, Vesey AT, Shah AS et al (2015) Valvular (18)F-fluoride and (18)F-fluorodeoxyglucose uptake predict disease progression and clinical outcome in patients with aortic stenosis. J Am Coll Cardiol 66:1200–1201
Vahanian A, Beyersdorf F, Praz F et al (2022) 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 43:561–623
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15:827–832
Lew R, Doros G (2010) Design based on intra-class correlation coefficients. Am J Biostatistics 1:1–8
Clavel MA, Messika-Zeitoun D, Pibarot P et al (2013) The complex nature of discordant severe calcified aortic valve disease grading: new insights from combined Doppler echocardiographic and computed tomographic study. J Am Coll Cardiol 62:2329–2338
Bossé Y, Mathieu P, Pibarot P (2008) Genomics: the next step to elucidate the etiology of calcific aortic valve stenosis. J Am Coll Cardiol 51:1327–1336
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15:155–163
Kang DH, Park SJ, Lee SA et al (2020) Early surgery or conservative care for asymptomatic aortic stenosis. N Engl J Med 382:111–119
Strange G, Stewart S, Celermajer D et al (2019) Poor long-term survival in patients with moderate aortic stenosis. J Am Coll Cardiol 74:1851–1863
Rosenhek R, Klaar U, Schemper M et al (2004) Mild and moderate aortic stenosis. Natural history and risk stratification by echocardiography. Eur Heart J 25:199–205
Pio SM, Amanullah MR, Butcher SC et al (2021) Discordant severity criteria in patients with moderate aortic stenosis: prognostic implications. Open Heart 8:e001639
Mühlenbruch G, Thomas C, Wildberger JE et al (2005) Effect of varying slice thickness on coronary calcium scoring with multislice computed tomography in vitro and in vivo. Invest Radiol 40:695–699
Hughes-Austin JM, Dominguez A 3rd, Allison MA et al (2016) Relationship of coronary calcium on standard chest CT scans with mortality. JACC Cardiovasc Imaging 9:152–159
Decker JA, Bette S, Scheurig-Muenkler C, Bertram J et al (2022) Virtual non-contrast reconstructions of photon-counting detector CT angiography datasets as substitutes for true non-contrast acquisitions in patients after evar-performance of a novel calcium-Preserving Reconstruction Algorithm. Diagnostics (Basel) 12:558
Braverman AC, Güven H, Beardslee MA, Makan M, Kates AM, Moon MR (2005) The bicuspid aortic valve. Curr Probl Cardiol 30:470–522
Mohler ER 3rd (2000) Are atherosclerotic processes involved in aortic-valve calcification? Lancet 356:524–525
Wallby L, Janerot-Sjöberg B, Steffensen T, Broqvist M (2002) T lymphocyte infiltration in non-rheumatic aortic stenosis: a comparative descriptive study between tricuspid and bicuspid aortic valves. Heart 88:348–351
Mohler ER 3rd, Gannon F, Reynolds C et al (2001) Bone formation and inflammation in cardiac valves. Circulation. 103:1522–1528
Aggarwal SR, Clavel MA, Messika-Zeitoun D et al (2013) Sex differences in aortic valve calcification measured by multidetector computed tomography in aortic stenosis. Circ Cardiovasc Imaging 6:40–47
Davis AT, Palmer AL, Pani S, Nisbet A (2018) Assessment of the variation in CT scanner performance (image quality and Hounsfield units) with scan parameters, for image optimisation in radiotherapy treatment planning. Phys Med 45:59–64
Acknowledgements
The authors are grateful to Tohru Sekiya, the former president of Nitobe Bunka College, for his insightful comments.
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Kotaro Ouchi.
Conflict of interest
Makoto Kawai received research grants from DAIICHI SANKYO COMPANY, Ltd., Japan. The remaining authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and Biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• retrospective
• case-control study
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ouchi, K., Sakuma, T., Nojiri, A. et al. Optimal threshold score of aortic valve calcification for identification of significant aortic stenosis on non-electrocardiographic-gated computed tomography. Eur Radiol 33, 1243–1253 (2023). https://doi.org/10.1007/s00330-022-09114-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-022-09114-6