
Abstract
Aims/hypothesis
We aimed to investigate the association between maternal consumption of gluten-containing foods and other selected foods during late pregnancy and offspring risk of islet autoimmunity (IA) and type 1 diabetes in The Environmental Determinants of Diabetes in the Young (TEDDY) study.
Methods
The TEDDY study recruited children at high genetic risk for type 1 diabetes at birth, and prospectively follows them for the development of IA and type 1 diabetes (n = 8556). A questionnaire on the mother’s diet in late pregnancy was completed by 3–4 months postpartum. The maternal daily intake was estimated from a food frequency questionnaire for eight food groups: gluten-containing foods, non-gluten cereals, fresh milk, sour milk, cheese products, soy products, lean/medium-fat fish and fatty fish. For each food, we described the distribution of maternal intake among the four participating countries in the TEDDY study and tested the association of tertile of maternal food consumption with risk of IA and type 1 diabetes using forward selection time-to-event Cox regression.
Results
By 28 February 2019, 791 cases of IA and 328 cases of type 1 diabetes developed in TEDDY. There was no association between maternal late-pregnancy consumption of gluten-containing foods or any of the other selected foods and risk of IA, type 1 diabetes, insulin autoantibody-first IA or GAD autoantibody-first IA (all p ≥ 0.01). Maternal gluten-containing food consumption in late pregnancy was higher in Sweden (242 g/day), Germany (247 g/day) and Finland (221 g/day) than in the USA (199 g/day) (pairwise p < 0.05).
Conclusions/interpretation
Maternal food consumption during late pregnancy was not associated with offspring risk for IA or type 1 diabetes.
Trial registration
ClinicalTrials.gov NCT00279318.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.

Introduction
Type 1 diabetes arises as a result of both genetic predisposition and exposure to non-genetic factors. The asymptomatic prediabetic period, called islet autoimmunity (IA), is characterised by the appearance of islet autoantibodies, which are highly predictive of type 1 diabetes [1, 2]. Dietary factors may contribute to the development of IA or type 1 diabetes. Most investigations of dietary factors have focused on the timing of introduction of certain foods in infancy [3,4,5,6,7] and the frequency or amount of food consumption during childhood [8,9,10,11].
Relatively fewer studies have explored the relationship between maternal diet during pregnancy and the development of IA or type 1 diabetes in offspring [12,13,14,15,16], despite the well-documented impact of maternal nutrition on fetal development and childhood health outcomes [17,18,19]. The studies exploring this topic have identified protective effects from vegetable consumption [15], potato consumption [13], dietary sources of vitamin D [12] and consumption of butter, low-fat margarines, berries and coffee [14]. Maternal consumption of cereals, fish/dietary n-3 fatty acids and cow’s milk reportedly had no effect on the autoantibody status of the offspring [12,13,14,15, 20].
Gluten intake appears important in the development of autoimmune diseases, including celiac disease [21,22,23] and, at times, type 1 diabetes [24, 25]. However, recent large population-based studies report conflicting results—increased gluten intake during pregnancy was associated with increased risk of type 1 diabetes in Denmark [26], but not in Norway [27]. Neither study examined the role of maternal gluten intake in the appearance of islet autoantibodies.
The Environmental Determinants of Diabetes in the Young (TEDDY) is an international multicentre observational study prospectively following children from birth until the age of 15 years and seeking environmental factors involved in both type 1 diabetes [28] and celiac disease [29]. Environmental triggers during late pregnancy and infancy, including duration of breast feeding and timing of complementary food introduction, are closely monitored. Furthermore, prospective and frequent testing for islet autoantibodies gives the TEDDY study a unique opportunity to contribute to this small, but growing, pool of data. The aims of this manuscript are to describe late-pregnancy food consumption in TEDDY, and to explore the possible relationship between maternal consumption of gluten-containing foods and other selected foods and the development of IA or type 1 diabetes in offspring with increased genetic risk.
Methods
Study population
The TEDDY study is approved by local Ethical Institutional Review Boards and is monitored by an External Advisory Board formed by the National Institutes of Health. It involves six clinical research centres located in Colorado, Georgia/Florida and Washington State in the USA and in Finland, Germany and Sweden that all follow the same study protocol, which includes scheduled visits every third month until the age of 4 years and every sixth month thereafter [30]. Between September 2004 and February 2010, 424,788 newborn infants were screened and 21,589 infants fulfilled the inclusion criteria based on HLA genoty**. Altogether, 8676 children were enrolled in the follow-up study. Written informed consent was obtained for all study participants from a parent or primary caretaker, separately, for genetic screening and participation in the prospective follow-up, beginning at birth. Of these, 120 children were HLA ineligible and were thus excluded from the final sample, leaving a total of 8556 children for this study (Fig. 1).

Study population
Screening for IA and type 1 diabetes
Blood samples to test autoantibody status were drawn quarterly starting at 3 months of age during the first 4 years and biannually thereafter. Three autoantibodies against GAD (GADA), insulin (IAA) and insulinoma antigen-2 (IA-2A) were tested. Methods for testing samples for autoantibody positivity are described more thoroughly elsewhere [31]. An individual was considered autoantibody positive when a blood sample was confirmed positive at the two laboratories used in TEDDY (Barbara Davis Center for Childhood Diabetes, University of Colorado, USA and Bristol Laboratory, University of Bristol, UK). Persistent IA was defined as confirmed positive autoantibodies to IAA, GADA or IA-2A in at least two consecutive samples, collected at least 3 months apart. Previously published studies in TEDDY found a relationship between the order of autoantibody appearance and risk of type 1 diabetes [32,33,34,35]. We therefore examined secondary outcomes of IAA only or GADA only as the first appearing autoantibody (IAA-first IA and GADA-first IA, respectively). Type 1 diabetes was diagnosed by a physician according to the American Diabetes Association’s criteria. Data as of 28 February 2019 were used for all analyses.
Other characteristics
The infant screening form was completed by a family member at birth, and provided information about basic demographic and maternal characteristics, including family history of diabetes. This information was verified within the infant’s first year of life in another questionnaire. Mothers reported prenatal details such as consumption of selected foods, medications, smoking habits and education level attained, in addition to dietary supplement use, through self-administered questionnaire at 3.0–4.5 months postpartum. Trained interviewers reviewed questionnaires for completeness and detail at the first visit.
Information about basic demographic maternal characteristics was received from the infant screening form. A questionnaire was mailed home to the mother prior to the first clinic visit (3.0–4.5 months postpartum). This questionnaire contained questions regarding illnesses, use of medications or dietary supplements, smoking and alcohol consumption, and maternal diet during the last month of pregnancy (for the USA and Sweden) or the eighth month of pregnancy (for Finland and Germany). Information about maternal education was obtained at the 9 month clinic visit. Parents reported education level on a ten-category scale that was subsequently aggregated into three categories in order for the variable to be comparable across countries: basic primary education (high school qualification or less), vocational school or some university, and university degree or higher. Alcohol consumption was recorded as ‘yes’ if any alcohol was consumed during any trimester in pregnancy.
Maternal food consumption
Information on maternal dietary intake during the eighth or ninth month of pregnancy (depending on country) was collected using a food frequency questionnaire (FFQ) specifically designed to capture consumption of cereals/grains, milk and milk products, soy and fish/seafood [34]. The mother reported how often she ate foods such as cereals, bread, porridge, pastas, pizza, bakery products, cow’s milk and cream, sour milk and other cultured cow’s milks including yoghurts, cheeses, soy and soy products, and various fishes and seafood. Altogether, 36 food items or food groups were included in the FFQ. Fish were categorised according to the fat content: lean, medium or fatty. One portion of each type of food was described in the questionnaire to help the mother to estimate the consumption frequency per portion; examples of portion sizes are: one slice of bread, one bowl of oatmeal, one glass of milk, two slices of cheese, one serving of salmon and one serving of shrimps. Consumption frequencies of non-gluten cereals, i.e. those containing oats, rice and corn, were asked for separately from the consumption frequencies of foods containing wheat, barley and/or rye. All food consumption frequencies were converted into daily consumption frequencies (servings/day). Therefore, daily consumption frequencies were used as such but weekly frequencies were divided by 7 and monthly by 30. Differences in customary serving sizes (in grams) by country were taken into consideration. The amount (g/day) of food consumed was estimated from mean daily consumption frequencies and summed up in nine food categories: gluten-containing foods, non-gluten cereals, fresh milks (and cream), sour milks (including all cultured milks), cheese products, soy products, lean fish/seafood, medium-fat fish and fatty fish. Lean and medium-fat fish exposures were pooled in the analyses because reported medium-fat fish consumption was low. Soy products were infrequently reported—80% of mothers reported zero soy consumption.
Statistical analysis
For each food group, we described maternal intake for all countries and separately by country. Overall differences between intakes across countries were tested using the Kruskal–Wallis test. For any food group showing significantly different overall distributions, we tested pairwise differences between countries using the Wilcoxon signed rank test.
Four endpoints were analysed: time to IA (any), time to IAA-first IA, time to GADA-first IA and time to type 1 diabetes. Each endpoint was analysed separately. The stratified Cox proportional hazards model was used for each analysis with country as the stratification. For the time to first antibody (IA, IAA-first IA, GADA-first IA), HLA-DR-DQ genotype, family history of type 1 diabetes, sex and probiotics before 28 days of age (yes/no) were covariates in the analysis. For time to type 1 diabetes, HLA-DR-DQ genotype, family history of type 1 diabetes and sex were covariates in the analysis. Potential confounders, such as maternal age, maternal education, BMI and smoking during pregnancy (yes/no), were examined in a forward stepwise algorithm with a cut-off of 0.01 in the Cox proportional hazards models for all endpoints.
Our primary focus was the relationship between gluten-containing food consumption during late pregnancy and each of the four outcomes, given that gluten intake during pregnancy has been implicated as a risk factor for type 1 diabetes in the offspring [26]. Daily gluten-containing food consumption was categorised into tertiles and scaled as 1, 2, 3 in the analysis to increase the power to detect a monotonic relationship with exposure. A two-tailed significance level of 0.05 for gluten-containing food exposure was considered statistically significant.
Other maternal food consumption variables were analysed similarly to the gluten-containing food analysis, except for soy products which was dichotomised (0, >0). For these secondary analyses, a two-tailed 0.01 level was considered statistically significant to account for the multiple comparisons.
Results
Of 8556 TEDDY participants, 791 cases of IA and 328 cases of type 1 diabetes developed by 28 February 2019. Maternal and participant characteristics of the study population (n = 8556) are shown in Table 1. Approximately 11% (n = 951) have a first-degree relative with type 1 diabetes and 39% (n = 3339) have the highest risk HLA-DR3/4 genotype. Maternal age at delivery ranged from 27 to 34 years (median = 30 years). Among mothers of TEDDY participants, 48% (n = 4118) have a college degree, 13% (n = 1150) smoked during pregnancy and 33% (n = 2851) drank alcohol during pregnancy. Participant characteristics are provided by study endpoints in the Electronic supplementary material (ESM) Table 1.
Table 2 shows the mean, count and tertile cut-points for each of the food groups overall and by participating country. Maternal intake of all food groups differed by country (Kruskal–Wallis p < 0.001), as did most pairwise comparisons between countries (Table 2, Wilcoxon signed rank p < 0.05). Consistent with a previous examination of gluten-containing cereal servings per day [36], mean maternal gluten-containing food consumption in late pregnancy was higher in Sweden (242 g/day), Germany (247 g/day) and Finland (221 g/day) than in the USA (199 g/day). Mothers in Finland reported the highest consumption of fresh milk (482 g/day), sour milk (223 g/day), cheese products (75 g/day) and fatty fish (24 g/day), compared with other TEDDY countries.
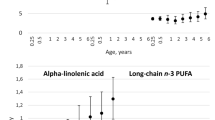
We found no evidence of an association between tertile of maternal gluten-containing food consumption and risk of IA (high vs low, HR 1.00; 95% CI 0.83, 1.20), type 1 diabetes (high vs low, HR 0.88; 95% CI 0.67, 1.17), IAA-first IA (high vs low, HR 0.95; 95% CI 0.71, 1.26) or GADA-first IA (high vs low, HR 1.08; 95% CI 0.82, 1.43). Complete model results are provided in ESM Table 2. Other than first-degree relative status, no other maternal factors were significantly associated with any outcome and were therefore excluded from the model. Results did not change when we treated the gluten food measure analytically similar to previous studies [26, 27], using a continuous measure and comparing the lowest with highest groups of maternal intake (10th compared with 90th percentile). Kaplan–Meier survival curves for each endpoint are shown in Fig. 2. From forward selection Cox regression, there were also no significant (p < 0.01) associations detected between any maternal food group consumption and any of the four offspring endpoints: IA, IAA-first IA, GADA-first IA and type 1 diabetes. Interactions for each of the eight food groups with HLA and with country (country was included as a covariate as opposed to a stratification variable for this analysis) were also examined for each of the four endpoints. There were no significant (p < 0.01) interactions for any of the food groups for any endpoint.

Kaplan–Meier survival curves from any IA (a), type 1 diabetes (T1D) (b), IAA-first IA (c) and GADA-first IA (d) by tertile (cut-points: 168, 247 g/day) of maternal gluten-containing food consumption in late pregnancy; tertile 1, blue; tertile 2, red; tertile 3, green
Additional sensitivity analyses were conducted by including SNP covariates and other covariates which have previously been associated with either autoimmunity or type 1 diabetes in the models. For IAA as the first antibody, GAD as the first antibody and any persistent confirmed antibody endpoints, the additional covariates were extensively hydrolysed cow’s milk-based formula prior to 7 days of age (yes/no), weight z-score at 12 months and SNPs rs2476601 in PTPN22, rs2816316 in RGS1, rs2292239 in ERBB3, rs3184504 in SH2B3, rs4948088 in COBL, rs1004446 in INS, rs1270876 in CLEC16A, rs10517086, rs1143678 in ITGAM and rs4597342 in ITGAM [37,38,39]. For the type 1 diabetes endpoint, the additional covariates were SNPs rs2476601 in PTPN22, rs2292239 in ERBB3, rs3184504 in SH2B3, rs1004446 in INS, rs7111341 in INS, rs11711054 in CCR5 and rs3825932 in INT [38]. These sensitivity analyses did not find any significant (p < 0.01) association with any of the food groups for any endpoint.
Discussion
Maternal late-pregnancy consumption of gluten-containing foods, non-gluten cereals, fresh milk, sour milk, cheese products, lean/medium-fat fish, fatty fish and soy products was not associated with risk of IA, type 1 diabetes, IAA-first IA or GADA-first IA in children with high genetic risk. These findings were robust to sensitivity analyses examining differences (interactions) by HLA genotype and country of origin, despite differences in the amount of maternal late-pregnancy food consumption among Finland, Germany, Sweden and the USA. Additional adjustment for characteristics previously associated with IA or type 1 diabetes in this study did not alter these findings.
The lack of association between maternal gluten-containing food consumption and offspring risk of IA confirms smaller, country-specific studies of maternal cereal consumption among high-risk children in the USA [13] and Finland [14]. Our study extends these findings by establishing no relationship between maternal gluten-containing food consumption and offspring risk of type 1 diabetes among high-risk children. While outside the scope of this study, we cannot exclude the possibility that maternal gluten consumption may act in concert with offspring gluten exposures, such as the timing of gluten introduction during infancy or childhood gluten intake, that have been previously associated with risk of IA or type 1 diabetes [3, 24, 25].
Our study supports similarly null findings between maternal gluten intake and type 1 diabetes reported from the population-based study in Norway [27]. The modest magnitude of association reported in Denmark showed only marginal significance, and, with fewer cases represented than for either Norway or the present study, may be a chance finding. However, notable differences between these studies and ours should be considered. Findings may not be directly comparable as we report the amount (g/day) of gluten-containing foods assessed by our selective FFQ rather than estimating total gluten amount in the maternal diet as reported by these two prior studies. Furthermore, results from our genetically high-risk population may not be generalisable to the general population. We also cannot exclude the possibility that our findings might be different if we had assessed second-trimester rather than third-trimester gluten consumption, similar to the two population-based studies. Maternal FFQs were completed slightly later than for the prior studies (at 3 months postpartum compared with during the second trimester of pregnancy). This methodological difference is unlikely to explain differences in study findings, however, as maternal pregnancy diet recall has been shown to have comparable accuracy as recent diet recall, up to 6 [40] or 7 [41] years postpartum.
Previous investigations of broader maternal food consumption during pregnancy in high-risk prospective studies have focused on the IA outcome, and found no association for cereals, fish or cow’s milk [12,13,14,15, 20]. Our study supports these previous findings, showing no relationship between cereals (gluten-containing or non-gluten), fish (lean/medium or fatty) or milk (fresh, sour or cheese products) and risk of IA. Our study extends these findings to demonstrate no relationship between maternal food group consumption during late pregnancy and additional outcomes, including: IAA-first IA, GADA-first IA and type 1 diabetes. The protective factors previously identified (vegetable consumption [15], potato consumption [13], dietary sources of vitamin D [12] and consumption of butter, low-fat margarines, berries and coffee [14]) were not included in the maternal FFQ, and therefore could not be studied.
Our study has many strengths. As the largest prospective study of high-risk children, this study is well powered to identify risk factors for type 1 diabetes [42, 43]. Maternal FFQs were collected prior to the development of offspring outcomes; therefore, maternal food consumption reporting is not subject to recall bias. The intense, frequent follow-up of study participants enables precise and harmonised ascertainment of type 1 diabetes outcomes [31], including the preclinical IA outcomes that cannot be examined in registry-based linkage studies such as those from Norway and Denmark [26, 27]. Study participants represent the population most likely to develop type 1 diabetes—children of European ancestry carrying higher risk HLA genotypes. Our results are therefore generalisable to similarly high-risk populations. Shared protocols in this multi-national study allowed us to demonstrate no difference in findings across countries. All analyses or sensitivity analyses included the full set of previously identified risk factors and potential confounders, giving us the ability to demonstrate no independent effect of maternal consumption of gluten-containing foods or other foods in the disease process. We appropriately accounted for the multiple testing burden a priori by establishing a forward selection significance threshold at an α of 0.01 for foods to be included in regression modelling.
For children at high genetic risk, maternal food consumption in late pregnancy is not associated with risk of IA or type 1 diabetes. Our results do not support the avoidance of gluten-containing or other foods during late pregnancy to modify the risk of type 1 diabetes disease in offspring.
Data availability
Data described in the manuscript will be made available upon request from the NIDDK Central Repository at https://www.niddkrepository.org/studies/teddy.
Abbreviations
- FFQ:
-
Food frequency questionnaire
- IA:
-
Islet autoimmunity
- IA-2A:
-
Insulinoma antigen-2 autoantibody
- IAA:
-
Insulin autoantibody
- GADA:
-
GAD autoantibody
- TEDDY:
-
The Environmental Determinants of Diabetes in the Young
References
Orban T, Sosenko JM, Cuthbertson D et al (2009) Pancreatic islet autoantibodies as predictors of type 1 diabetes in the Diabetes Prevention Trial-Type 1. Diabetes Care 32(12):2269–2274. https://doi.org/10.2337/dc09-0934
Jacobsen LM, Larsson HE, Tamura RN et al (2019) Predicting progression to type 1 diabetes from ages 3 to 6 in islet autoantibody positive TEDDY children. Pediatr Diabetes 20(3):263–270. https://doi.org/10.1111/pedi.12812
Norris JM, Barriga K, Klingensmith G et al (2003) Timing of initial cereal exposure in infancy and risk of islet autoimmunity. JAMA 290(13):1713–1720. https://doi.org/10.1001/jama.290.13.1713
Uusitalo U, Lee HS, Andren Aronsson C et al (2018) Early infant diet and islet autoimmunity in the TEDDY study. Diabetes Care 41(3):522–530. https://doi.org/10.2337/dc17-1983
Virtanen SM, Räsänen L, Ylönen K et al (1993) Early introduction of dairy products associated with increased risk of IDDM in Finnish children. The Childhood in Diabetes in Finland Study Group. Diabetes 42(12):1786–1790. https://doi.org/10.2337/diab.42.12.1786
Virtanen SM, Takkinen HM, Nevalainen J et al (2011) Early introduction of root vegetables in infancy associated with advanced ß-cell autoimmunity in young children with human leukocyte antigen-conferred susceptibility to type 1 diabetes. Diabet Med 28(8):965–971. https://doi.org/10.1111/j.1464-5491.2011.03294.x
Frederiksen B, Kroehl M, Lamb MM et al (2013) Infant exposures and development of type 1 diabetes mellitus: the Diabetes Autoimmunity Study in the Young (DAISY). JAMA Pediatr 167(9):808–815. https://doi.org/10.1001/jamapediatrics.2013.317
Lamb MM, Frederiksen B, Seifert JA, Kroehl M, Rewers M, Norris JM (2015) Sugar intake is associated with progression from islet autoimmunity to type 1 diabetes: the Diabetes Autoimmunity Study in the Young. Diabetologia 58(9):2027–2034. https://doi.org/10.1007/s00125-015-3657-x
Lamb MM, Miller M, Seifert JA et al (2015) The effect of childhood cow's milk intake and HLA-DR genotype on risk of islet autoimmunity and type 1 diabetes: the Diabetes Autoimmunity Study in the Young. Pediatr Diabetes 16(1):31–38. https://doi.org/10.1111/pedi.12115
Syrjala E, Nevalainen J, Peltonen J et al (2019) A joint modeling approach for childhood meat, fish and egg consumption and the risk of advanced islet autoimmunity. Sci Rep 9(1):7760. https://doi.org/10.1038/s41598-019-44196-1
Virtanen SM, Nevalainen J, Kronberg-Kippila C et al (2012) Food consumption and advanced beta cell autoimmunity in young children with HLA-conferred susceptibility to type 1 diabetes: a nested case-control design. Am J Clin Nutr 95(2):471–478. https://doi.org/10.3945/ajcn.111.018879
Fronczak CM, Baron AE, Chase HP et al (2003) In utero dietary exposures and risk of islet autoimmunity in children. Diabetes Care 26(12):3237–3242. https://doi.org/10.2337/diacare.26.12.3237
Lamb MM, Myers MA, Barriga K, Zimmet PZ, Rewers M, Norris JM (2008) Maternal diet during pregnancy and islet autoimmunity in offspring. Pediatr Diabetes 9(2):135–141. https://doi.org/10.1111/j.1399-5448.2007.00311.x
Virtanen SM, Uusitalo L, Kenward MG et al (2011) Maternal food consumption during pregnancy and risk of advanced β-cell autoimmunity in the offspring. Pediatr Diabetes 12(2):95–99. https://doi.org/10.1111/j.1399-5448.2010.00668.x
Brekke HK, Ludvigsson J (2010) Daily vegetable intake during pregnancy negatively associated to islet autoimmunity in the offspring--the ABIS study. Pediatr Diabetes 11(4):244–250. https://doi.org/10.1111/j.1399-5448.2009.00563.x
Niinisto S, Takkinen HM, Uusitalo L et al (2014) Maternal dietary fatty acid intake during pregnancy and the risk of preclinical and clinical type 1 diabetes in the offspring. Br J Nutr 111(5):895–903. https://doi.org/10.1017/s0007114513003073
Barker DJP (1997) Maternal nutrition, fetal nutrition, and disease in later life. Nutrition 13(9):807–813. https://doi.org/10.1016/S0899-9007(97)00193-7
Wu G, Bazer FW, Cudd TA, Meininger CJ, Spencer TE (2004) Maternal nutrition and fetal development. J Nutr 134(9):2169–2172. https://doi.org/10.1093/jn/134.9.2169
Yajnik CS, Deshpande SS, Jackson AA et al (2008) Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: the Pune Maternal Nutrition Study. Diabetologia 51(1):29–38. https://doi.org/10.1007/s00125-007-0793-y
Ludvigsson J (2003) Cow-milk-free diet during last trimester of pregnancy does not influence diabetes-related autoantibodies in nondiabetic children. Ann N Y Acad Sci 1005:275–278. https://doi.org/10.1196/annals.1288.042
Andren Aronsson C, Lee HS, Hard Af Segerstad EM et al (2019) Association of gluten intake during the first 5 years of life with incidence of celiac disease autoimmunity and celiac disease among children at increased risk. JAMA 322(6):514–523. https://doi.org/10.1001/jama.2019.10329
Mårild K, Dong F, Lund-Blix NA et al (2019) Gluten intake and risk of celiac disease: long-term follow-up of an at-risk birth cohort. Am J Gastroenterol 114(8):1307–1314. https://doi.org/10.14309/ajg.0000000000000255
Lund-Blix NA, Mårild K, Tapia G, Norris JM, Stene LC, Størdal K (2019) Gluten intake in early childhood and risk of celiac disease in childhood: a nationwide cohort study. Am J Gastroenterol 114(8):1299–1306. https://doi.org/10.14309/ajg.0000000000000331
Lund-Blix NA, Dong F, Marild K et al (2019) Gluten intake and risk of islet autoimmunity and progression to type 1 diabetes in children at increased risk of the disease: the Diabetes Autoimmunity Study in the Young (DAISY). Diabetes Care 42(5):789–796. https://doi.org/10.2337/dc18-2315
Hakola L, Miettinen ME, Syrjala E et al (2019) Association of cereal, gluten, and dietary fiber intake with islet autoimmunity and type 1 diabetes. JAMA Pediatr 173(10):953–960. https://doi.org/10.1001/jamapediatrics.2019.2564
Antvorskov JC, Halldorsson TI, Josefsen K et al (2018) Association between maternal gluten intake and type 1 diabetes in offspring: national prospective cohort study in Denmark. BMJ 362:k3547. https://doi.org/10.1136/bmj.k3547
Lund-Blix NA, Tapia G, Mårild K et al (2020) Maternal and child gluten intake and association with type 1 diabetes: the Norwegian Mother and Child Cohort Study. PLoS Med 17(3):e1003032. https://doi.org/10.1371/journal.pmed.1003032
Hagopian WA, Erlich H, Lernmark A et al (2011) The Environmental Determinants of Diabetes in the Young (TEDDY): genetic criteria and international diabetes risk screening of 421 000 infants. Pediatr Diabetes 12(8):733–743. https://doi.org/10.1111/j.1399-5448.2011.00774.x
Liu E, Lee H-S, Aronsson CA et al (2014) Risk of pediatric celiac disease according to HLA haplotype and country. N Engl J Med 371(1):42–49. https://doi.org/10.1056/NEJMoa1313977
Lernmark B, Johnson SB, Vehik K et al (2011) Enrollment experiences in a pediatric longitudinal observational study: the Environmental Determinants of Diabetes in the Young (TEDDY) study. Contemp Clin Trials 32(4):517–523. https://doi.org/10.1016/j.cct.2011.03.009
Vehik K, Fiske SW, Logan CA et al (2013) Methods, quality control and specimen management in an international multicentre investigation of type 1 diabetes: TEDDY. Diabetes Metab Res Rev 29(7):557–567. https://doi.org/10.1002/dmrr.2427
Krischer JP, Liu X, Lernmark A et al (2017) The influence of type 1 diabetes genetic susceptibility regions, age, sex, and family history on the progression from multiple autoantibodies to type 1 diabetes: a TEDDY study report. Diabetes 66(12):3122–3129. https://doi.org/10.2337/db17-0261
Krischer JP, Lynch KF, Lernmark A et al (2017) Genetic and environmental interactions modify the risk of diabetes-related autoimmunity by 6 years of age: the TEDDY study. Diabetes Care 40(9):1194–1202. https://doi.org/10.2337/dc17-0238
Krischer JP, Lynch KF, Schatz DA et al (2015) The 6 year incidence of diabetes-associated autoantibodies in genetically at-risk children: the TEDDY study. Diabetologia 58(5):980–987. https://doi.org/10.1007/s00125-015-3514-y
Lynch KF, Lee HS, Törn C et al (2018) Gestational respiratory infections interacting with offspring HLA and CTLA-4 modifies incident β-cell autoantibodies. J Autoimmun 86:93–103. https://doi.org/10.1016/j.jaut.2017.09.005
Uusitalo U, Lee HS, Aronsson CA et al (2015) Gluten consumption during late pregnancy and risk of celiac disease in the offspring: the TEDDY birth cohort. Am J Clin Nutr 102(5):1216–1221. https://doi.org/10.3945/ajcn.115.119370
Elding Larsson H, Vehik K, Haller MJ et al (2016) Growth and risk for islet autoimmunity and progression to type 1 diabetes in early childhood: The Environmental Determinants of Diabetes in the Young Study. Diabetes 65(7):1988–1995. https://doi.org/10.2337/db15-1180
Sharma A, Liu X, Hadley D et al (2018) Identification of non-HLA genes associated with development of islet autoimmunity and type 1 diabetes in the prospective TEDDY cohort. J Autoimmun 89:90–100. https://doi.org/10.1016/j.jaut.2017.12.008
Hummel S, Beyerlein A, Tamura R et al (2017) First infant formula type and risk of islet autoimmunity in The Environmental Determinants of Diabetes in the Young (TEDDY) study. Diabetes Care 40(3):398–404. https://doi.org/10.2337/dc16-1624
Mejía-Rodríguez F, Orjuela MA, García-Guerra A, Quezada-Sanchez AD, Neufeld LM (2012) Validation of a novel method for retrospectively estimating nutrient intake during pregnancy using a semi-quantitative food frequency questionnaire. Matern Child Health J 16(7):1468–1483. https://doi.org/10.1007/s10995-011-0912-8
Bunin GR, Gyllstrom ME, Brown JE, Kahn EB, Kushi LH (2001) Recall of diet during a past pregnancy. Am J Epidemiol 154(12):1136–1142. https://doi.org/10.1093/aje/154.12.1136
TEDDY Study Group (2007) The Environmental Determinants of Diabetes in the Young (TEDDY) study: study design. Pediatr Diabetes 8(5):286–298. https://doi.org/10.1111/j.1399-5448.2007.00269.x
Lee HS, Burkhardt BR, McLeod W et al (2014) Biomarker discovery study design for type 1 diabetes in The Environmental Determinants of Diabetes in the Young (TEDDY) study. Diabetes Metab Res Rev 30(5):424–434. https://doi.org/10.1002/dmrr.2510
Acknowledgements
Thank you to the participants and families of the TEDDY study, whose continued commitment make such research possible. The TEDDY Study Group is acknowledged for excellent collaboration (see the ESM).
Authors’ relationships and activities
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Funding
The TEDDY study is funded by U01 DK63829, U01 DK63861, U01 DK63821, U01 DK63865, U01 DK63863, U01 DK63836, U01 DK63790, UC4 DK63829, UC4 DK63861, UC4 DK63821, UC4 DK63865, UC4 DK63863, UC4 DK63836, UC4 DK95300, UC4 DK100238, UC4 DK106955, UC4 DK112243, UC4 DK117483 and Contract No. HHSN267200700014C from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the National Institute of Allergy and Infectious Diseases (NIAID), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Institute of Environmental Health Sciences (NIEHS), the Centers for Disease Control and Prevention (CDC) and JDRF. This work was supported in part by the NIH/NCATS Clinical and Translational Science Awards to the University of Florida (UL1 TR000064) and the University of Colorado (UL1 TR002535).
Author information
Authors and Affiliations
Consortia
Contributions
RKJ led the interpretation of data, drafted the manuscript and approved the final version. RT led the statistical analyses, critically revised the manuscript for intellectual content and approved the final version. NF led the study design, critically revised the manuscript for intellectual content and approved the final version. UU, JY, SN, CAA, A-GZ, WH, MR, JT, BA, JK, SMV and JMN substantially contributed to the study design and the acquisition and interpretation of data, critically revised the manuscript for intellectual content and approved the final version. JMN is the guarantor of this work and, as such, accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM
(PDF 114 kb)
Rights and permissions
About this article

Cite this article
Johnson, R.K., Tamura, R., Frank, N. et al. Maternal food consumption during late pregnancy and offspring risk of islet autoimmunity and type 1 diabetes. Diabetologia 64, 1604–1612 (2021). https://doi.org/10.1007/s00125-021-05446-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-021-05446-y