
Abstract
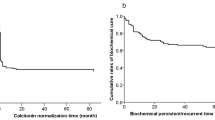
Medullary thyroid carcinoma (MTC) is an uncommon tumor, representing about 0.1 % of all human cancers. It develops from the calcitonin-secreting parafollicular C cells of the thyroid gland. MTC is mainly sporadic but about 25 % are inherited (multiple endocrine neoplasia or familial MTC) due to a RET germline mutation. Lymph node spread is early and distant metastases are present in 7–23 % of patients at presentation. Besides lymph nodes, the main distant metastatic sites are the bone, liver, and lung. Postoperative serum calcitonin (Ct) measurement plays a central role in detecting persistent or recurrent disease and estimating the extent of the disease. Ct and CEA doubling times (after initial surgery) predict tumor progression and may guide the timing of diagnostic imaging procedures. Prognosis is linked to the age at diagnosis, the stage of the disease, and also to the serum Ct and CEA doubling time. Total thyroidectomy and an initial appropriate neck lymph node dissection are associated with a higher biochemical cure rate.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Similar content being viewed by others

References
Raue F, Kotzerke J, Reinwein D, et al. Prognostic factors in medullary thyroid carcinoma: evaluation of 741 patients from the German medullary thyroid carcinoma register. Clin Investig. 1993;71:7–12.
Rossi RL, Cady B, Meissner WA, et al. Non familial medullary thyroid carcinoma. Am J Surg. 1980;139:554–60.
Moley JF, De Benedetti MK. Patterns of nodal metastases in palpable medullary thyroid carcinoma: recommendations for extent of node dissection. Ann Surg. 1999;229:880–7.
Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American Thyroid Association. Thyroid. 2009;19:565–612.
Atkins D, Eccles M, Flottorp S, et al. GRADE Working Group: grading quality of evidence and strength of recommendations. BMC Health Serv Res. 2004;4:38.
Swiglo BA, Murad MH, Schünemann HJ, et al. A case for clarity, consistency, and helpfulness: state-of-the-art clinical practice guidelines in endocrinology using the grading of recommendations, assessment, development, and evaluation system. J Clin Endocrinol Metab. 2008;93:666–73.
Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American college of chest physicians task force. Chest. 2006;129:174–81.
Schlumberger M, Carlomagno F, Baudin E, et al. New therapeutic approaches to treat medullary thyroid carcinoma. Nat Clin Pract Endocrinol Metab. 2008;4:22–32.
Kraeber-Bodéré F, Salaun PY, Oudoux A, et al. Pretargeted radioimmunotherapy in rapidly progressing, metastatic, medullary thyroid cancer. Cancer. 2010;116(4 Suppl):1118–25.
Roman S, Lin R, Sosa JA. Prognosis of medullary thyroid carcinoma: demographic, clinical and pathologic predictors of survival in 1252 cases. Cancer. 2006;107:2134–42.
Giraudet al, Vanel D, Leboulleux S, et al. Imaging medullary thyroid carcinoma with persistent elevated calcitonin levels. J Clin Endocrinol Metab. 2007;92:4185–90.
Mirallié E, Vuillez JP, Bardet S, et al. High frequency of bone/bone marrow involvement in advanced medullary thyroid cancer. J Clin Endocrinol Metab. 2005;90:779–88.
Hundahl SA, Fleming ID, Fremgen AM, et al. A national cancer data base report on 53,856 cases of thyroid carcinoma treated in the US 1985-1995. Cancer. 1998;83:2638–48.
Modigliani E, Cohen R, Campos JM, et al. Prognostic factors for survival and for biochemical cure in medullary thyroid carcinoma: results in 899 patients. The GETC Study Group. Clin Endocrinol. 1998;48:265–73.
Barbet J, Campion L, Kraeber-Bodere F, et al. Prognostic impact of serum calcitonin and carcinoembryonic antigen doubling-times in patients with medullary thyroid carcinoma. J Clin Endocrinol Metab. 2005;90:6077–84.
Giraudet al, Al Ghulzan A, Aupérin A, et al. Progression of medullary thyroid carcinoma: assessment with calcitonin and carcinoembryonic antigen doubling times. Eur J Endocrinol. 2008;158:239–46.
Scollo C, Baudin E, Travagli JP, et al. Rationale for central and bilateral lymph node dissection in sporadic and hereditary medullary thyroid cancer. J Clin Endocrinol Metab. 2003;88:2070–5.
Moley JF, Dilley WG, DeBenedetti MK. Improved results of cervical reoperation for medullary thyroid carcinoma. Ann Surg. 1997;225:734–40.
Kebebew E, Kikuchi S, Duh QY, et al. Long-term results of reoperation and localizing studies in patients studies in patients with persistent or recurrent medullary thyroid cancer. Arch Surg. 2000;135:895–901.
Brierley J, Tsang R, Simpson WJ, et al. Medullary thyroid cancer: analyses of survival and prognostic factors and the role of radiation therapy in local control. Thyroid. 1996;6:305–10.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Drissi, F., Mirallié, E. (2016). Management of Postoperative Hypercalcitoninemia in MTC. In: Cooper, D., Durante, C. (eds) Thyroid Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-22401-5_38
Download citation
DOI: https://doi.org/10.1007/978-3-319-22401-5_38
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-22400-8
Online ISBN: 978-3-319-22401-5
eBook Packages: MedicineMedicine (R0)