
Abstract
Background
The dog is the most popular companion animal and is a valuable large animal model for several human diseases. Canine immune-mediated hematological diseases, including immune-mediated hemolytic anemia (IMHA) and immune thrombocytopenia (ITP), share many features in common with autoimmune hematological diseases of humans. The gut microbiome has been linked to systemic illness, but few studies have evaluated its association with immune-mediated hematological disease. To address this knowledge gap, 16S rRNA gene sequencing was used to profile the fecal microbiota of dogs with spontaneous IMHA and ITP at presentation and following successful treatment. In total, 21 affected and 13 healthy control dogs were included in the study.
Results
IMHA/ITP is associated with remodeling of fecal microbiota, marked by decreased relative abundance of the spirochete Treponema spp., increased relative abundance of the pathobionts Clostridium septicum and Escherichia coli, and increased overall microbial diversity. Logistic regression analysis demonstrated that Treponema spp. were associated with decreased risk of IMHA/ITP (odds ratio [OR] 0.24–0.34), while Ruminococcaceae UCG-009 and Christensenellaceae R-7 group were associated with increased risk of disease (OR = 6.84 [95% CI 2–32.74] and 8.36 [95% CI 1.85–71.88] respectively).
Conclusions
This study demonstrates an association of immune-mediated hematological diseases in dogs with fecal dysbiosis, and points to specific bacterial genera as biomarkers of disease. Microbes identified as positive or negative risk factors for IMHA/ITP represent an area for future research as potential targets for new diagnostic assays and/or therapeutic applications.
Similar content being viewed by others


Background
Nearly half of all American households own dogs as companion animals (American Pet Products Association Survey 2015–2016) and dogs are increasingly recognized as a large animal model of human diseases [1,2,3]. Immune-mediated hematological disease, including immune-mediated hemolytic anemia (IMHA) and immune thrombocytopenia (ITP), is an important cause of morbidity and mortality in dogs. IMHA shares many of the features of warm autoimmune hemolytic anemia in people [4]. Similarly, ITP in the two species shows several common characteristics [5,6,7,8]. Erythrocytes or platelets become bound by immunoglobin, leading to opsonization and phagocytosis by macrophages [9,10,11]. As a result of this process, canine patients present with anemia or thrombocytopenia. First-line therapy involves immunosuppression with corticosteroids, but up to 70% of canine patients with IMHA and up to 20% of patients with ITP succumb to their disease or are euthanized because of aggressive autoimmunity [12,13,14,15,16,17].
Numerous environmental triggers, including infections, toxins, drugs, parasites, or neoplasia [11, 18,19,20,21,22], have been implicated in the development of autoimmune disease. Notably, there is increasing recognition that the “exposome”—environmental factors that include the patient’s mucosal microbiota—impacts the manifestation of autoimmune disease in humans [23, 24]. Over the past 10 years, a growing evidence base has demonstrated that gut microbiota are crucial for host function and nutrient availability [25,26,27], xenobiotic detoxification [28,29,30], and immune system maturation and regulation [31, 43]. Dysbiosis has been documented in human ITP patients in several studies and is speculated to contribute to pathogenesis [44, 45]. One study of human ITP patients found a link to alterations in the intestinal microbiome and treatment response [46]. Similarly, our preliminary data suggested changes in the intestinal microbiome in dogs with ITP or IMHA, including enrichment of potential pathogens (Clostridium septicum and Escherichia coli) [47]. A case report describing fecal microbiota transplantation to treat human ITP raises awareness of the therapeutic potential of this strategy, andan ongoing clinical trial is evaluating the efficacy of probiotics in human ITP [48].
In the current study, we hypothesize that alterations in the gut microbiome, inferred from fecal microbiota, are a hallmark of immune-mediated hematological diseases in dogs. Characterizing the fecal microbiota of healthy and diseased dogs, we sought to identify microbial biomarkers of IMHA/ITP in this model species.
Results
Study population
A total of 31 patients were initially recruited. Twenty-one patients, comprising 17 dogs with IMHA and four dogs with ITP, were responsive to immunosuppressive treatment and were included in the study (Fig. 1A). In addition, 13 healthy dogs were sampled, comprising three ‘in contact’ controls from the same households as affected animals and 10 that were not in contact with affected animals (Fig. 1A). Response to immunosuppressive treatment was defined by an increase in packed cell volume in IMHA, or platelet count in ITP, without relapse, within the first eight weeks of treatment (Fig. 1B). Samples were collected from affected animals at baseline, and two and eight weeks after initiating treatment.

Study design of a survey of gut microbiota in canine immune-mediated hematological disease. A Fecal samples of healthy dogs were collected once both from the disease in-contact and non-in-contact dogs. Samples of diseased dogs were collected at presentation (week 0/baseline) and week 2 and week 8 after treatment. B Assessments of the clinical response of IMHA (PCV %) or ITP (platelet count × 1000/μL) patients at weeks 0, 2, and 8. The normal values of PCV and platelet counts are depicted by shading. IMHA: immune-mediated hemolytic anemia, ITP: immune thrombocytopenia, PCV: packed cell volume
During the study period, 15 of the 21 reported cases were prescribed antimicrobial therapy, including amoxicillin with clavulanic acid (1), ampicillin (1), enrofloxacin (2), doxycycline (4), and metronidazole (10). The beta diversity profile of fecal samples from dogs treated with antimicrobials overlapped with that of dogs not treated with antimicrobials (p = 0.21 by PERMANOVA test; Additional file 1: Figure S1).
Characterization of fecal microbiota in study dogs reveals consistent mammalian patterns
The qualified dataset contained an average of 49,333 non-chimeric reads, ranging from 27,115 to 71,579 reads/sample (median = 48,690 reads/sample; mean = 49,333 reads/sample) after DADA2 amplicon sequence variant (ASV) de-noising. Broad taxonomic representation of fecal microbiota was similar in healthy and diseased dogs at baseline (Additional file 1: Figure S2). In descending order by relative abundance (> 1% on average), Firmicutes, Bacteroidetes, Spirochaetes, Euryarchaeota and Proteobacteria were the dominant phyla in most of the healthy and baseline disease samples. Firmicutes and Bacteroidetes accounted for over 50% of gut microbiota. Treponema (Spirochaetes), Methanobrevibacter (Euryarchaeota), and Escherichia-Shigella (Proteobacteria) were the dominant genera belonging to the most abundant phyla. To distinguish the primary differences between healthy dogs and those with immune-mediated hematological disease, we combined all unaffected dogs to create a single control group, and all affected dogs to create a single disease group, in subsequent analyses.
Immune-mediated hematological diseases are associated with fecal microbial alterations
Fecal microbial composition, including abundance and diversity, was analyzed in detail in the healthy and IMHA/ITP dogs to determine the differences between disease status at baseline, prior to initiation of immunosuppressive therapy. Alpha diversity, as measured by Shannon’s index and Simpson’s index, was higher in affected dogs (Fig. 2A).

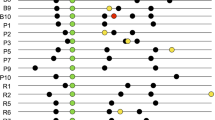
Differential diversity and composition of gut microbiota in healthy and diseased dogs. A Alpha diversity measured by the Shannon’s index and Simpson’s index. The diseased dogs had significantly higher Shannon’s and Simpson’s indices. B Baseline differential abundance heatmap of gut microbiota between healthy and diseased dogs. Thirty-seven significantly differentiated features (amplicon sequence variants; ASVs) were identified by the DESeq2 test (p < 0.05 and standard error of the log2 fold change estimate, lfcSE < 4)
We used DESeq2 [49] to identify microbes that were differentially abundant between healthy and diseased dogs (p < 0.05 and standard error of the log2 fold change estimate [lfcSE] < 4) (Fig. 2B). Eight taxa were enriched in the healthy dogs, predominantly belonging to the genus Treponema. Twenty-nine taxa were enriched in the affected dogs, including several potential pathogens such as Clostridium septicum (the closest NCBI RefSeq annotation for Clostridium sensu stricto 1 in Fig. 2B) and Escherichia coli (the closest NCBI RefSeq annotation for Escherichia-Shigella in Fig. 2B).
Distinct fecal microbes predict risk of immune-mediated hematological disease
Since we observed several taxa associated with canine IMHA/ITP (Fig. 3A), we used logistic regression analysis to test whether these taxa would predict the risk of develo** IMHA/ITP. In total, we observed 12 taxa associated with either increased or decreased odds of develo** IMHA/ITP (Fig. 3B and Additional file 1: Table S1). Amongst these were three taxa belonging to the genus Treponema associated with decreased risk of IMHA/ITP (odds ratio [OR] = 0.24–0.34; see details in Additional file 1: Table S1). Analysis of the ASVs from these taxa showed that the closest species annotations were Treponema bryantii (94.07–98.02% identity) and Treponema pectinovorum (94.47% identity). We also identified seven taxa, including one Treponema sp. (Treponema parvum; 92.10% identity; OR = 2.74, 95% confidence interval [CI] = 1.15–7.98), two Eubacterium coprostanoligenes (92.89% identity, OR = 2.03, 95% CI = 1.12–4.83 and 90.51% identity, OR = 2.7, 95% CI = 1.28–9.82) and Phascolarctobacterium succinatutens (99.60% identity, OR = 2.58, 95% CI = 1.12–7.57), associated with increased risk of IMHA/ITP, with odds ratios ranging from 2.03 to 8.36 (Additional file 1: Table S1). Two of the taxa most strongly associated with disease were Ruminococcaceae UCG-009 (OR = 6.84, 95% CI = 2–32.74) and Christensenellaceae R-7 group (OR = 8.36, 95% CI = 1.85–71.88), with the closest species annotations being Papillibacter cinnamivorans (92.89% identity) and Novibacillus thermophilus (88.54% identity), respectively.

Risk of disease conferred by the differential abundance of microbial amplicon sequence variants (ASVs) identified by odds ratios (OR). A Significant ASVs identified by DESeq2 test were tested by logistic regression models. B Models passing a p < 0.05 threshold are presented with odds ratios (OR) and 95% confidence intervals
Fecal microbial alterations persist with remission of disease following treatment
We next asked whether disease-associated changes in the fecal microbiota of IMHA/ITP dogs resolved with treatment. Treatment with immunosuppressive drugs yielded robust recovery of hematological parameters in the affected dogs included in this study (Fig. 1B). Beta diversity analysis showed no significant shift in microbiome structure following treatment (Fig. 4A, p = 0.21 by PERMANOVA test; Fig. 4B, p = 0.85 by Kruskal–Wallis test). Microbial changes along PC2, accounting for approximately 16% of the total variance in our data set, showed a possible association with treatment, but changes, if any, were subtle (Fig. 4C).

A Beta diversity profile (weighted Unifrac distance) of gut microbiota among healthy and diseased dogs at baseline, and weeks 2 and 8. B Time course comparison of the diseased group's microbiota measured by distance (weighted Unifrac) to the healthy group. C Violin plots demonstrate microbial composition among groups or time points along axis 2 (Kruskal–Wallis test among groups, p = 0.01). The significance of pairwise tests by Dunn's test is labelled as *p < 0.05, **p < 0.01
We examined relative abundance of the 12 risk-associated taxa identified from logistic regression analysis of baseline samples (Fig. 3 and Additional file 1: Table S1). Relative abundance of five taxa showed significant differences from the healthy group (Fig. 5). Treponema (ASV 47 and ASV 107) and Lachnospiraceae (ASV 271) showed lower relative abundance in diseased dogs throughout treatment. In contrast, Ruminococcaceae UCG-009 (ASV 185) and Christensenellaceae R-7 group (ASV 212) show higher relative abundance in diseased dogs. In addition, the Christensenellaceae R-7 group (ASV 212) remained more abundant throughout treatment, consistent with changes in beta diversity. In all cases, there were no significant changes in relative abundance with treatment.

The relative abundance alterations of no-risk versus risk taxa among groups and time points. Five significantly altered taxa were identified by a Kruskal–Wallis test with Dunn’s post-hoc test (compared to the healthy group). The significance of pairwise tests is labelled as *p < 0.05, **p < 0.01, ***p < 0.001
Discussion
Our study is the first to examine the fecal microbiota of dogs with the two most common immune-mediated hematological diseases in this species. Although we regard this as a pilot study, the differential abundance of several bacterial species within the diseased dogs was notable. These differences raise the intriguing possibility that fecal microbial composition may play a protective or pathogenic role in immune-mediated diseases of the blood. To our surprise, there were no significant changes in fecal microbial populations with treatment over the eight-week period of observation despite remission of disease, arguing against rapid shifts in the fecal microbiome that mirror those of clinical disease.
Several species of the genus Treponema showed lower abundance in the diseased dogs, prompting us to speculate that they may play a protective role in health. In contrast, Ruminococcaceae and Christensenellaceae R-7 group species showed higher abundance in the diseased dogs, raising the possibility that they may play a pathogenic role in disease. Several studies in other species have demonstrated the importance of the intestinal microbiome in the initiation and progression of autoimmune disease, driven by mechanisms including the translocation of pathobionts that elaborate proinflammatory molecules, bacterial mimicry of autoantigens, and parallel dysregulation of the metabolome with attenuation of anti-inflammatory pathways [50,51,52,53].
Increasing recognition of the role of the intestinal microbiome in distal homeostatic and pathogenic immune pathways suggests that manipulation of the mucosal microbiota with antibiotics, prebiotics, probiotics, synbiotics, or fecal transplantation may represent a novel therapeutic opportunity in autoimmunity [53,54,55,56]. Various studies have documented intestinal dysbiosis in human ITP, as well as bacterial signatures that correlate with clinical indices, but the discordance of findings and relative paucity of data underscore the complexity of this field and the need for additional research [44, 45, 57, 58]. Moreover, to the best of our knowledge similar studies have not been performed in autoimmune hemolytic anemia in human patients, which represents an unmet need in this area of medicine [4, 56].
The lower abundance of Treponema spp. in diseased dogs in the current study is a novel finding. Although this spirochete genus has been associated with syphilis [59], gastritis [60], Alzheimer’s disease [61], periodontitis and gingivitis [62] in people, and periodontitis in dogs [63,64,65], the potentially protective role of certain Treponema spp. has been poorly characterized. Nguyen and colleagues documented decreased abundance of four core genera, including Treponema, in the feces and cecal mucus of mice with complete Freund adjuvant-induced arthritis, a model of rheumatoid arthritis [66]. The synthesis of anti-inflammatory short chain fatty acids by Treponema spp. was suggested as a possible protective mechanism, but both their impact on disease and any mechanistic basis of such interactions remain speculative at this juncture. Moreover, one species, Treponema parvum, was among those seven taxa associated with increased risk of IMHA/ITP in our study, emphasizing the danger of broad, genus-level statements that ignore species-level nuances.
The increased abundance of Ruminococcaceae and Christensenellaceae R-7 group species in the diseased dogs also represents a novel, albeit unexpected, finding. In general, the Ruminococcaceae are anti-inflammatory, short-chain fatty acid-synthesizing bacteria present in high abundance in the intestinal microbiota of healthy people [67] and dogs [42, 68], and low abundance in human patients with various autoimmune diseases [69, 70], including ITP [58]. Of note in the canine intestinal microbiome is the species Faecalibacterium prausnitzii, a strict anaerobe of the phylum Firmicutes, class Clostridia, and order Clostridiales that is considered a hallmark of intestinal microbial health [42, 71]. Nevertheless, individual species within this family may have pathogenic potential. The closest species annotation for Ruminococcaceae UCG-009 is Papillibacter cinnamivorans, a bacterium whose abundance is associated with both beneficial outcomes, for example in dogs fed a Mulberry leaf supplement in the treatment of obesity [72], and deleterious outcomes, for example in patients with Parkinson’s disease [73]. Similarly, another species belonging to this family, Ruminococcus anavus, was present in greater abundance in the feces of patients with ITP, in which alterations of microbial species correlated with clinical indices [46]. In similar fashion to the Ruminococcaceae, the Christensenellaceae are generally considered to be anti-inflammatory healthy bacteria [74], present in lower abundance in states of autoimmunity [75]. However, little is known of the species we identified, Novibacillus thermophilus, and the possibility remains that intestinal microbial perturbations represent protective rather than pathogenic mechanisms, triggered as a response to immune-mediated disease [76].
Other bacteria positively associated with disease in our study included Clostridium septicum, Eubacterium coprostanoligenes, and Phascolarctobacterium succinatutens. While none of these bacteria has been associated with immune-mediated disorders, they have been associated with other disease entities. Documented in the fecal microbiota of healthy people and dogs, Clostridium septicum has been associated with sepsis [77], type 3c diabetes mellitus [78], and colorectal cancer [79,80,81,82]. Bacteria within the genus Eubacterium are generally considered beneficial to health, producing butyrate and metabolizing bile acids and cholesterol [83, 84]. Eubacterium coprostanoligenes is a cholesterol-reducing anaerobic coccobacillus that has been implicated in the phenomenon of manure “foaming” [85], but little is known about its pathogenic potential. Its abundance in the feces of children with autism spectrum disorder was positively correlated with gastrointestinal symptoms [86]. Fecal microbiota transplantation decreased the abundance of this bacterium, with an improvement in both behavioral and gastrointestinal symptoms, suggesting a possible association with neurobehavioral disease [86]. Its potential role in autoimmune disease remains unknown. The abundance of bacteria within the genus Phascolarctobacterium has been associated with neuropsychiatric disorders [87], psoriasis [88], Hashimoto thyroiditis [89], and diabetes mellitus [90, 91], suggesting pathogenic potential in a variety of settings. There was a positive correlation between the concentration of soluble interleukin-2 receptor in psoriasis patients and fecal abundance of Phascolarctobacterium [88], raising the possibility that this bacterium may contribute to the pro-inflammatory phenotype of this disease. Phascolarctobacterium succinatutens has been implicated as a signature species in human metabolic dysfunction fatty liver disease [92], although its abundance was reduced in the intestinal microbiome of obese cats [93]. This dichotomy once again highlights the challenges inherent in associating specific bacteria with specific diseases within and across mammalian taxa.
The lack of significant changes in the fecal microbiota with treatment of the IMHA/ITP patients in this study, all of which responded to immunosuppression within eight weeks, was unanticipated. We had speculated that dysbiotic signatures associated with disease would normalize in parallel with clinical remission, as has been found in several diseases of immune-mediated etiology in human patients and rodent models, including rheumatoid arthritis [66, 94], uveitis [95], keratoconjunctivitis sicca [51], neuropsychiatric disorders [86], diabetes mellitus [96], and autoimmune thyroid disorders [97]. It is possible the changes we documented in fecal microbiota may take longer than eight weeks to normalize, or that the apparent dysbiosis in these patients may never completely resolve while they are being treated. Furthermore, several dogs received antimicrobial drugs during the time immunosuppressive therapy was administered, potentially inhibiting normalization of fecal microbial communities despite the apparent absence of an antimicrobial impact on beta diversity (Additional file 1: Figure S1). There is also increasing recognition that glucocorticoids negatively impact intestinal microbial diversity in several species [98,99,100,101,102]. Nevertheless, changes in the microbiota induced by glucocorticoids are thought to underlie their beneficial impact in systemic lupus erythematosus [103, 104] and inflammatory bowel disease [105], underscoring the complexity of the inter-relationship between intestinal microbial composition, disease status, and the influence of therapeutic drugs. If dysbiosis is a primary pathogenic driver of IMHA and ITP, we hypothesize that delayed normalization of microbial composition could contribute to the tendency of patients to relapse with premature cessation of immunosuppressive treatment.
There were several shortcomings of this study, from which only preliminary conclusions can therefore be drawn. A modest number of dogs with IMHA and ITP were recruited from multiple centers of wide geographical dispersion, managed by different clinicians with different clinical approaches. Given the limited number of cases, both diseases were considered as one group, potentially undermining our ability to discern disease-specific signatures. We included only samples from dogs responding to immunosuppressive treatment, precluding the assessment of bacterial signatures associated with unresponsive, or relapsing, disease. Most of the healthy control dogs were from different households from the cases recruited into the study, giving us no opportunity to control for differences attributable to specific environmental exposure. Patients were tracked for only eight weeks, with the risk of missing longer-term changes in the fecal microbiota. There were also limitations in the taxonomic resolution of short-reading sequences. Nevertheless, several notable observations were made, robust to the confounding influence of recruiting center, specific disease, and other variables. Pilot data were generated that motivate further studies in a larger number of patients in the future.
In conclusion, immune-mediated hematological disease in dogs was associated with alterations in fecal microbiota in this small cohort of patients. Whether these changes were of primary pathogenic potential or epiphenomena remains unknown. Novel treatments that aim to restore healthy microbial composition may provide an adjunct to current immunosuppressive approaches in canine IMHA and ITP. Further research at the nexus of the intestinal microbiome and autoimmune disease in this species is warranted.
Methods
Inclusion criteria, treatment regimen, and sample collection
Immune-mediated hemolytic anemia was diagnosed by documenting a packed cell volume (PCV) of < 35% or a hemoglobin concentration of < 11 g/dL, associated with two examples of antibodies directed against erythrocyte antigens, as indicated by either a positive saline agglutination or Coombs’ test result, or moderate to marked spherocytosis [106]. When only one of the above tests suggestive of antibodies was available, the additional indicator of hemolysis (i.e. hyperbilirubinemia, hemoglobinuria, hemoglobinemia, erythrocyte ghosts) fulfilled inclusion criteria. Idiopathic (non-associative) disease was diagnosed using a standardized diagnostic approach ruling out potential trigger factors—including iatrogenic causes, neoplasia, and infection—as assessed by history, physical examination, imaging of the thorax and abdomen, and screening for vector-borne pathogens [106].
Immune thrombocytopenia was diagnosed by documenting a platelet count of less than 50,000/µL in a dog with no macroplatelets (confirmed on a blood smear) and no evidence of associative disease or disseminated intravascular coagulation, as assessed by imaging of the thorax and abdomen, screening for vector-borne pathogens, and coagulation tests. A canine bleeding assessment tool (DOGiBAT) score of at least 2 was required for inclusion [107].
In both IMHA and ITP, treatment-naïve cases were recruited, defined by the administration of no more than three doses of an immunosuppressive drug or biologic in the 28 days preceding presentation, either consecutively or non-consecutively. To minimize confounding factors, cases were excluded if they had received any antimicrobial drugs or pre/probiotics in the five days preceding presentation, or one or more doses of a vaccine or a toxin in the 28 days preceding presentation (Additional file 1: Table S2). Dogs were not allowed to receive antimicrobials during the study period except doxycycline for prophylaxis against vector-borne pathogens (pending test results), metronidazole for non-limiting diarrhea associated with mycophenolate mofetil administration, or drugs to treat secondary infections that arose once the dogs had been recruited (e.g. urinary tract infection) (Additional file 1: Figures S3 and S4). Neither the patients nor control dogs had received long-term antimicrobial drugs prior to recruitment.
All recruited cases received immunosuppressive therapy, comprising initial dexamethasone (0.2–0.3 mg/kg IV q24h; maximum dose 8 mg), followed by prednisone or prednisolone (1.6-3 mg/kg PO q24h; maximum dose 60 mg) and, in most cases, a second immunosuppressive drug (Additional file 1: Figures S3 and S4; Table S2). The administration of blood products was permitted as clinically indicated. After initial recruitment, cases were excluded if clinically significant comorbidities (e.g. diabetes mellitus) were diagnosed. Cases that failed to respond to treatment or that relapsed during the eight-week study period were also excluded from the final dataset. Corticosteroid therapy was tapered gradually, according to a standard protocol [108]. Remission of disease was defined by the attainment of a PCV > 37% (IMHA) or a platelet count of > 150,000/µL (ITP) and the absence of immune markers of disease. Relapse, if it occurred, was defined by a drop in PCV of at least 5% (IMHA) or a drop in platelet count of at least 50,000/µL (ITP) since the preceding visit.
Patients were recruited from four centers, including the Matthew J Ryan Hospital, University of Pennsylvania (Penn Vet; n = 16), Cornell University Hospital for Animals (n = 12), the Lloyd Veterinary Medical Center, Iowa State University (n = 1), and the Foster Hospital for Small Animals, Tufts University (n = 2). At each time point, a fresh fecal sample was collected by rectal palpation or from a clean surface within 15 min of defecation. Fresh fecal samples were also collected once from healthy control dogs, both from the same household as patients (when available; in-contact, n = 3) and different households (non‒in-contact; n = 10). Inclusion criteria for healthy control dogs included the presence of systemic health based on a history and physical examination; the absence of antimicrobial or pre/pro-biotic consumption within five days of presentation; and the consumption of no more than two doses, either consecutively or non-consecutively, of any drug, including immunosuppressives and biologicals but excluding nutraceuticals, within 28 days of presentation. Neither the patients nor control dogs had consumed raw diets or treats within 28 days of presentation.
Fresh fecal samples of at least 10 g in weight were collected within 15 min of defecation or by rectal palpation, delivered to Penn Vet within three hours of collection, and kept at 4 °C for no more than 48 h, before being treated and stored at − 20 °C. If drop-off at Penn Vet was not possible within three hours of defecation, fecal samples were stored in a − 20 °C freezer (within three hours of defecation) and transported to Penn Vet on ice within 10 days of being placed in the − 20 °C freezer.
16S rRNA gene sequencing and data analysis
Bacterial genomic DNA was extracted from homogenized fecal samples using the PowerSoil DNA Isolation Kit (MO BIO Laboratories, Carlsbad, CA) following the manufacturer’s instructions. A mock community genomic DNA library was amplified and sequenced as a quality control sample. Additional controls included extraction of blank-processed samples (water only) to determine background microbial signal. A Nextera dual-index amplicon library construction method targeted the V4 region of the 16S rRNA gene by PCR amplification [109]. Pico-green-based amplicons were sequenced on a MiSeq platform (Illumina, San Diego, CA) using 250 bp paired-end chemistry.
A total of 3,990,059 paired-end sequences were generated for the 71 samples (excluding samples with fewer than 5,000 read counts, blank and mock control samples) from the Illumina MiSeq platform. The 16S rRNA gene amplicon sequences were processed using the Quantitative Insights Into Microbial Ecology 2 (QIIME 2) pipeline (version 2019.10) [110]. Reads were truncated at 220 bp for forward reads and 200 bp for reverse reads, then de-noised using the DADA2 algorithm [111, 112]. Amplicon sequence variants (ASVs) were obtained via the de-noising process with quality filtering and removal of chimeras. Consensus taxonomy was assigned using the classifier-consensus-vsearch plugin (the VSEARCH algorithm) [113, 114] against SILVA NR132 99% 16S rRNA gene sequences [115, 116]. The NCBI 16S RefSeq Nucleotide sequence records (retrieved from https://www.ncbi.nlm.nih.gov/refseq/targetedloci/16S_process/ on January 8th 2022) were downloaded and trained as a BLAST database; the closet taxonomy of each ASV was assigned by using ‘blastn’ algorithm under the criteria of e-value ≤ 1e-5, max_target_seqs = 1, and max_hsps = 1. Representative sequences were aligned with MAFFT v7, and variable positions were then masked. A phylogenetic tree was built with the FastTree 2.1 and then rooted with midpoint.
Microbiome diversity and composition were analyzed in the context of disease status, and then visualized using the MARco [117], vegan [118], and pheatmap [119] packages in R software (version 4.1.2) [120]. A Kruskal–Wallis test and Dunn’s post-hoc test were used for all statistical analyses of group comparisons with a significance level of α = 0.05, and the p values were adjusted with a false discovery rate (FDR). A DESeq2 [49] analysis allowed group comparisons of each feature under the criteria of p < 0.05 and lfcSE < 4. Alpha diversity indices were estimated by richness, Shannon’s index, and Simpson’s index. Beta diversity of microbial communities was measured by weighted Unifrac distance [121, 122] using a principal coordinates analysis (PCoA). Heterogeneity was examined using ADONIS tests.
Availability of data and materials
Raw 16S rRNA gene sequences and metagenomic sequences for all samples used in this study have been deposited in the Sequence Read Archive (SRA) (accession number pending).
References
Davis BW, Ostrander EA. Domestic dogs and cancer research: a breed-based genomics approach. ILAR J. 2014;55(1):59–68.
Fenger JM, London CA, Kisseberth WC. Canine osteosarcoma: a naturally occurring disease to inform pediatric oncology. ILAR J. 2014;55(1):69–85.
Gilmore KM, Greer KA. Why is the dog an ideal model for aging research? Exp Gerontol. 2015;71:14–20.
Barcellini W. New insights in the pathogenesis of autoimmune hemolytic anemia. Transfus Med Hemother. 2015;42(5):287–93.
Kohli R, Chaturvedi S. Epidemiology and clinical manifestations of immune thrombocytopenia. Hamostaseologie. 2019;39(3):238–49.
LeVine DN, Brooks MB. Immune thrombocytopenia (ITP): Pathophysiology update and diagnostic dilemmas. Vet Clin Pathol. 2019;48(Suppl 1):17–28.
Semple JW, Rebetz J, Maouia A, Kapur R. An update on the pathophysiology of immune thrombocytopenia. Curr Opin Hematol. 2020;27(6):423–9.
LeVine DN, Birkenheuer AJ, Brooks MB, Nordone SK, Bellinger DA, Jones SL, Fischer TH, Oglesbee SE, Frey K, Brinson NS, et al. A novel canine model of immune thrombocytopenia: Has immune thrombocytopenia (ITP) gone to the dogs? Br J Haematol. 2014;167(1):110–20.
Harvey JW. Veterinary hematology: a diagnostic guide and color atlas. Elsevier Health Sciences; 2011.
McCullough S. Immune-mediated hemolytic anemia: understanding the nemesis. Vet Clin North Am Small Anim Pract. 2003;33(6):1295–315.
Mitchell K, Kruth S: Immune-mediated hemolytic anemia and other regenerative anemias. Textbook of veterinary internal medicine 2010:761–772.
Piek CJ. Canine idiopathic immune-mediated haemolytic anaemia: a review with recommendations for future research. Vet Q. 2011;31(3):129–41.
Swann JW, Skelly BJ. Systematic review of evidence relating to the treatment of immune-mediated hemolytic anemia in dogs. J Vet Intern Med. 2013;27(1):1–9.
Swann JW, Skelly BJ. Systematic review of prognostic factors for mortality in dogs with immune-mediated hemolytic anemia. J Vet Intern Med. 2015;29(1):7–13.
Cooper SA, Huang AA, Raskin RE, Weng HY, Scott-Moncrieff JC. Clinical data, clinicopathologic findings and outcome in dogs with amegakaryocytic thrombocytopenia and primary immune-mediated thrombocytopenia. J Small Anim Pract. 2016;57(3):142–7.
O’Marra SK, Delaforcade AM, Shaw SP. Treatment and predictors of outcome in dogs with immune-mediated thrombocytopenia. J Am Vet Med Assoc. 2011;238(3):346–52.
Simpson K, Chapman P, Klag A. Long-term outcome of primary immune-mediated thrombocytopenia in dogs. J Small Anim Pract. 2018;59(11):674–80.
Bloom JC, Thiem PA, Sellers TS, Deldar A, Lewis HB. Cephalosporin-induced immune cytopenia in the dog: demonstration of erythrocyte-, neutrophil-, and platelet-associated IgG following treatment with cefazedone. Am J Hematol. 1988;28(2):71–8.
Mellor PJ, Roulois AJ, Day MJ, Blacklaws BA, Knivett SJ, Herrtage ME. Neutrophilic dermatitis and immune-mediated haematological disorders in a dog: suspected adverse reaction to carprofen. J Small Anim Pract. 2005;46(5):237–42.
Reimer ME, Troy GC, Warnick LD. Immune-mediated hemolytic anemia: 70 cases (1988–1996). J Am Anim Hosp Assoc. 1999;35(5):384–91.
Swann JW, Skelly BJ. Evaluation of immunosuppressive regimens for immune-mediated haemolytic anaemia: a retrospective study of 42 dogs. J Small Anim Pract. 2011;52(7):353–8.
Whitley NT, Day MJ. Immunomodulatory drugs and their application to the management of canine immune-mediated disease. J Small Anim Pract. 2011;52(2):70–85.
Floreani A, Leung PS, Gershwin ME. Environmental basis of autoimmunity. Clin Rev Allergy Immunol. 2016;50(3):287–300.
Miyauchi E, Shimokawa C, Steimle A, Desai MS, Ohno H. The impact of the gut microbiome on extra-intestinal autoimmune diseases. Nat Rev Immunol. 2023;23(1):9–23.
LeBlanc JG, Milani C, de Giori GS, Sesma F, van Sinderen D, Ventura M. Bacteria as vitamin suppliers to their host: a gut microbiota perspective. Curr Opin Biotechnol. 2013;24(2):160–8.
Sannino DR, Dobson AJ, Edwards K, Angert ER, Buchon N. The drosophila melanogaster gut microbiota provisions thiamine to its host. MBio. 2018;9(2):10–128.
de Vos WM, Tilg H, Van Hul M, Cani PD. Gut microbiome and health: mechanistic insights. Gut. 2022;71(5):1020–32.
Kohl KD, Oakeson KF, Orr TJ, Miller AW, Forbey JS, Phillips CD, Dale C, Weiss RB, Dearing MD. Metagenomic sequencing provides insights into microbial detoxification in the guts of small mammalian herbivores (Neotoma spp.). FEMS Microbiol Ecol. 2018;94(12):fiy184.
Turner LA, Bucking C. The role of intestinal bacteria in the ammonia detoxification ability of teleost fish. J Exp Biol. 2019;222:jeb209882.
Zhu L, Yang Z, Yao R, Xu L, Chen H, Gu X, Wu T, Yang X. Potential mechanism of detoxification of cyanide compounds by gut microbiomes of bamboo-eating pandas. mSphere. 2018;3(3):10–128.
Thaiss CA, Zmora N, Levy M, Elinav E. The microbiome and innate immunity. Nature. 2016;535(7610):65–74.
**menez C, Torres J. Development of microbiota in infants and its role in maturation of gut mucosa and immune system. Arch Med Res. 2017;48(8):666–80.
Lloyd-Price J, Arze C, Ananthakrishnan AN, Schirmer M, Avila-Pacheco J, Poon TW, Andrews E, Ajami NJ, Bonham KS, Brislawn CJ, et al. Multi-omics of the gut microbial ecosystem in inflammatory bowel diseases. Nature. 2019;569(7758):655–62.
Hoyles L, Fernandez-Real JM, Federici M, Serino M, Abbott J, Charpentier J, Heymes C, Luque JL, Anthony E, Barton RH, et al. Molecular phenomics and metagenomics of hepatic steatosis in non-diabetic obese women. Nat Med. 2018;24(7):1070–80.
Zhu W, Gregory JC, Org E, Buffa JA, Gupta N, Wang Z, Li L, Fu X, Wu Y, Mehrabian M, et al. Gut microbial metabolite TMAO enhances platelet hyperreactivity and thrombosis risk. Cell. 2016;165(1):111–24.
Sampson TR, Debelius JW, Thron T, Janssen S, Shastri GG, Ilhan ZE, Challis C, Schretter CE, Rocha S, Gradinaru V, et al. Gut microbiota regulate motor deficits and neuroinflammation in a model of Parkinson’s disease. Cell. 2016;167(6):1469-1480 e1412.
Brennan CA, Garrett WS. Gut microbiota, inflammation, and colorectal cancer. Annu Rev Microbiol. 2016;70:395–411.
Klingensmith NJ, Coopersmith CM. The gut as the motor of multiple organ dysfunction in critical illness. Crit Care Clin. 2016;32(2):203–12.
Deng P, Swanson KS. Gut microbiota of humans, dogs and cats: current knowledge and future opportunities and challenges. Br J Nutr. 2015;113(Suppl):S6-17.
Berry ASF, Johnson K, Martins R, Sullivan MC, Farias Amorim C, Putre A, Scott A, Wang S, Lindsay B, Baldassano RN, et al. Natural infection with giardia is associated with altered community structure of the human and canine gut microbiome. mSphere. 2020;5(4):10–128.
Wang S, Martins R, Sullivan MC, Friedman ES, Misic AM, El-Fahmawi A, De Martinis ECP, O’Brien K, Chen Y, Bradley C, et al. Diet-induced remission in chronic enteropathy is associated with altered microbial community structure and synthesis of secondary bile acids. Microbiome. 2019;7(1):126.
Pilla R, Suchodolski JS. The role of the canine gut microbiome and metabolome in health and gastrointestinal disease. Front Vet Sci. 2019;6:498.
Vazquez-Baeza Y, Hyde ER, Suchodolski JS, Knight R. Dog and human inflammatory bowel disease rely on overlap** yet distinct dysbiosis networks. Nat Microbiol. 2016;1:16177.
Liu C, Cheng L, Ji L, Li F, Zhan Y, Wu B, Ke Y, Chen P, Hua F, Yuan L, et al. Intestinal microbiota dysbiosis play a role in pathogenesis of patients with primary immune thrombocytopenia. Thromb Res. 2020;190:11–9.
Zhang X, Gu S, You L, Xu Y, Zhou D, Chen Y, Yan R, Jiang H, Li Y, Lv L, et al. Gut microbiome and metabolome were altered and strongly associated with platelet count in adult patients with primary immune thrombocytopenia. Front Microbiol. 2020;11:1550.
Wang Y, Liu F, Zhang G, Su Y, Sun X, Chen Q, Wang C, Fu H, He Y, Zhu X, et al. Gut microbiome alterations and its link to corticosteroid resistance in immune thrombocytopenia. Sci China Life Sci. 2021;64(5):766–83.
Liu P-Y, McGonigle K, Carroll A, Chiango J, Scavello H, Martins R, Mehta S, Krespan E, LeVine D, Fellman C et al: The intestinal microbiome of dogs with immune-mediated hemolytic anemia or immune thrombocytopenia. In: American college of veterinary internal medicine hybrid forum. Austin, TX, USA; 2022.
Borody T, Campbell J, Torres M, Nowak A, Leis S. Reversal of idiopathic thrombocytopenic purpura [ITP] with fecal microbiota transplantation [FMT]: 941. Off J Am Coll Gastroenterol ACG. 2011;106:352.
Love MI, Huber W, Anders S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014;15(12):550.
Shaheen WA, Quraishi MN, Iqbal TH. Gut microbiome and autoimmune disorders. Clin Exp Immunol. 2022;209(2):161–74.
Watane A, Raolji S, Cavuoto K, Galor A. Microbiome and immune-mediated dry eye: a review. BMJ Open Ophthalmol. 2022;7(1):e000956.
Christovich A, Luo XM. Gut microbiota, leaky gut, and autoimmune diseases. Front Immunol. 2022;13: 946248.
Mousa WK, Chehadeh F, Husband S. Microbial dysbiosis in the gut drives systemic autoimmune diseases. Front Immunol. 2022;13: 906258.
Pereira MS, Kriegel MA. Evolving concepts of host-pathobiont interactions in autoimmunity. Curr Opin Immunol. 2022;80: 102265.
Smits LP, Bouter KE, de Vos WM, Borody TJ, Nieuwdorp M. Therapeutic potential of fecal microbiota transplantation. Gastroenterology. 2013;145(5):946–53.
D’Angelo G. Microbiota and hematological diseases. Int J Hematol Oncol Stem Cell Res. 2022;16(3):164–73.
Wang X, Yi W, He L, Luo S, Wang J, Jiang L, Long H, Zhao M, Lu Q. Abnormalities in gut microbiota and metabolism in patients with chronic spontaneous Urticaria. Front Immunol. 2021;12: 691304.
Yu X, Zheng Q, He Y, Yu D, Chang G, Chen C, Bi L, Lv J, Zhao M, Lin X, et al. Associations of gut microbiota and fatty metabolism with immune thrombocytopenia. Front Med (Lausanne). 2022;9: 810612.
Radolf JD, Deka RK, Anand A, Šmajs D, Norgard MV, Yang XF. Treponema pallidum, the syphilis spirochete: making a living as a stealth pathogen. Nat Rev Microbiol. 2016;14(12):744–59.
Waskito LA, Rezkitha YAA, Vilaichone RK, Sugihartono T, Mustika S, Dewa Nyoman Wibawa I, Yamaoka Y, Miftahussurur M. The role of non-Helicobacter pylori bacteria in the pathogenesis of gastroduodenal diseases. Gut Pathog. 2022;14(1):19.
Chakravarthi ST, Joshi SG. An association of pathogens and biofilms with Alzheimer’s disease. Microorganisms. 2021;10(1):56.
Wyss C, Dewhirst FE, Gmür R, Thurnheer T, Xue Y, Schüpbach P, Guggenheim B, Paster BJ. Treponema parvum sp. nov., a small, glucoronic or galacturonic acid-dependent oral spirochaete from lesions of human periodontitis and acute necrotizing ulcerative gingivitis. Int J Syst Evol Microbiol. 2001;51:955–62.
Kačírová J, Sondorová M, Maďari A, Styková E, Mucha R, Nemcová R, Marečáková N, Farbáková J, Maďar M. Detection of periodontal pathogens from dental plaques of dogs with and without periodontal disease. Pathogens. 2022;11(4):480.
Kwon D, Bae K, Kim H, Kim SH, Lee D, Lee JH. Treponema denticola as a prognostic biomarker for periodontitis in dogs. PLoS ONE. 2022;17(1): e0262859.
Oba PM, Carroll MQ, Alexander C, Valentine H, Somrak AJ, Keating SCJ, Sage AM, Swanson KS. Microbiota populations in supragingival plaque, subgingival plaque, and saliva habitats of adult dogs. Anim Microbiome. 2021;3(1):38.
Nguyen NT, Sun WH, Chen TH, Tsai PC, Chen CC, Huang SL. Gut mucosal microbiome is perturbed in rheumatoid arthritis mice and partly restored after TDAG8 deficiency or suppression by salicylanilide derivative. Int J Mol Sci. 2022;23(7):3527.
De Weirdt R, Van de Wiele T. Micromanagement in the gut: microenvironmental factors govern colon mucosal biofilm structure and functionality. NPJ Biofilms Microbiomes. 2015;1:15026.
Pilla R, Suchodolski JS. The gut microbiome of dogs and cats, and the influence of diet. Vet Clin North Am Small Anim Pract. 2021;51(3):605–21.
Tremlett H, Fadrosh DW, Faruqi AA, Zhu F, Hart J, Roalstad S, Graves J, Lynch S, Waubant E. Gut microbiota in early pediatric multiple sclerosis: a case-control study. Eur J Neurol. 2016;23(8):1308–21.
**ang S, Qu Y, Qian S, Wang R, Wang Y, ** Y, Li J, Ding X. Association between systemic lupus erythematosus and disruption of gut microbiota: a meta-analysis. Lupus Sci Med. 2022;9(1):e000599.
Suchodolski JS. Analysis of the gut microbiome in dogs and cats. Vet Clin Pathol. 2022;50(1):6–17.
Park M, Jaiswal V, Kim K, Chun J, Lee MJ, Shin JH, Lee HJ. Mulberry leaf supplements effecting anti-inflammatory genes and improving obesity in elderly overweight dogs. Int J Mol Sci. 2022;23(23):15215.
Petrov VA, Saltykova IV, Zhukova IA, Alifirova VM, Zhukova NG, Dorofeeva YB, Tyakht AV, Kovarsky BA, Alekseev DG, Kostryukova ES, et al. Analysis of gut microbiota in patients with Parkinson’s disease. Bull Exp Biol Med. 2017;162(6):734–7.
Waters JL, Ley RE. The human gut bacteria Christensenellaceae are widespread, heritable, and associated with health. BMC Biol. 2019;17(1):83.
Rauz S, Low L, Suleiman K, Bassilious K, Rossiter A, Acharjee A, Loman N, Murray PI, Wallace GR. OP-10 gut microbiota Dysbiosis as a driver of inflammation in ocular mucous membrane pemphigoid. BMJ Open Ophthalmol. 2022;7(Suppl 1):A3.
Zhao X, Jiang L, Fang X, Guo Z, Wang X, Shi B, Meng Q. Host-microbiota interaction-mediated resistance to inflammatory bowel disease in pigs. Microbiome. 2022;10(1):115.
Khalid M, Lazarus R, Bowler IC, Darby C: Clostridium septicum sepsis and its implications. BMJ Case Rep 2012, 2012.
Talukdar R, Sarkar P, Jakkampudi A, Sarkar S, Aslam M, Jandhyala M, Deepika G, Unnisa M, Reddy DN. The gut microbiome in pancreatogenic diabetes differs from that of Type 1 and Type 2 diabetes. Sci Rep. 2021;11(1):10978.
Alves MLF, Ferreira MRA, Donassolo RA, Rodrigues RR, Conceição FR. Clostridium septicum: a review in the light of alpha-toxin and development of vaccines. Vaccine. 2021;39(35):4949–56.
Chew SS, Lubowski DZ. Clostridium septicum and malignancy. ANZ J Surg. 2001;71(11):647–9.
Dalal N, Jalandra R, Bayal N, Yadav AK, Harshulika, Sharma M, Makharia GK, Kumar P, Singh R, Solanki PR, et al. Gut microbiota-derived metabolites in CRC progression and causation. J Cancer Res Clin Oncol. 2021;147(11):3141–55.
Gagnière J, Raisch J, Veziant J, Barnich N, Bonnet R, Buc E, Bringer MA, Pezet D, Bonnet M. Gut microbiota imbalance and colorectal cancer. World J Gastroenterol. 2016;22(2):501–18.
Louis P, Flint HJ. Diversity, metabolism and microbial ecology of butyrate-producing bacteria from the human large intestine. FEMS Microbiol Lett. 2009;294(1):1–8.
Mukherjee A, Lordan C, Ross RP, Cotter PD. Gut microbes from the phylogenetically diverse genus Eubacterium and their various contributions to gut health. Gut Microbes. 2020;12(1):1802866.
Strom N, Ma Y, Bi Z, Andersen D, Trabue S, Chen C, Hu B. Eubacterium coprostanoligenes and Methanoculleus identified as potential producers of metabolites that contribute to swine manure foaming. J Appl Microbiol. 2022;132(4):2906–24.
Li N, Chen H, Cheng Y, Xu F, Ruan G, Ying S, Tang W, Chen L, Chen M, Lv L, et al. Fecal microbiota transplantation relieves gastrointestinal and autism symptoms by improving the gut microbiota in an open-label study. Front Cell Infect Microbiol. 2021;11: 759435.
Cheung SG, Goldenthal AR, Uhlemann AC, Mann JJ, Miller JM, Sublette ME. Systematic review of gut microbiota and major depression. Front Psychiatry. 2019;10:34.
Zhang X, Shi L, Sun T, Guo K, Geng S. Dysbiosis of gut microbiota and its correlation with dysregulation of cytokines in psoriasis patients. BMC Microbiol. 2021;21(1):78.
Liu S, An Y, Cao B, Sun R, Ke J, Zhao D. The composition of gut microbiota in patients bearing Hashimoto’s thyroiditis with Euthyroidism and hypothyroidism. Int J Endocrinol. 2020;2020:5036959.
Li W, Li L, Yang F, Hu Q, **ong D. Correlation between gut bacteria Phascolarctobacterium and exogenous metabolite α-linolenic acid in T2DM: a case-control study. Ann Transl Med. 2022;10(19):1056.
Yang HT, Liu JK, **u WJ, Tian TT, Yang Y, Hou XG, **e X. Gut Microbiome-based diagnostic model to predict diabetes mellitus. Bioengineered. 2021;12(2):12521–34.
Zhang Y, Yan S, Sheng S, Qin Q, Chen J, Li W, Li T, Gao X, Wang L, Ang L, et al. Comparison of gut microbiota in male MAFLD patients with varying liver stiffness. Front Cell Infect Microbiol. 2022;12: 873048.
Ma X, Brinker E, Graff EC, Cao W, Gross AL, Johnson AK, Zhang C, Martin DR, Wang X. Whole-genome shotgun metagenomic sequencing reveals distinct gut microbiome signatures of obese cats. Microbiol Spectr. 2022;10(3): e0083722.
Dagar S, Singh J, Saini A, Kumar Y, Chhabra S, Minz RW, Rani L. Gut bacteriome, mycobiome and virome alterations in rheumatoid arthritis. Front Endocrinol (Lausanne). 2022;13:1044673.
Rodríguez-Fernández CA, Iglesias MB, de Domingo B, Conde-Pérez K, Vallejo JA, Rodríguez-Martínez L, González-Barcia M, Llorenç V, Mondelo-Garcia C, Poza M et al. Microbiome in Immune-Mediated Uveitis. Int J Mol Sci. 2022;23(13):7020.
Hasain Z, Mokhtar NM, Kamaruddin NA, Mohamed Ismail NA, Razalli NH, Gnanou JV, Raja Ali RA. Gut microbiota and gestational diabetes mellitus: a review of host-gut microbiota interactions and their therapeutic potential. Front Cell Infect Microbiol. 2020;10:188.
Gong B, Wang C, Meng F, Wang H, Song B, Yang Y, Shan Z. Association between gut microbiota and autoimmune thyroid disease: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2021;12: 774362.
Liu H, Zhang B, Li F, Liu L, Li F. Shifts in the intestinal microflora of meat rabbits in response to glucocorticoids. J Sci Food Agric. 2022;102(12):5422–8.
MacLeod KJ, Kohl KD, Trevelline BK, Langkilde T. Context-dependent effects of glucocorticoids on the lizard gut microbiome. Mol Ecol. 2022;31(1):185–96.
Petrullo L, Ren T, Wu M, Boonstra R, Palme R, Boutin S, McAdam AG, Dantzer B. Glucocorticoids coordinate changes in gut microbiome composition in wild North American red squirrels. Sci Rep. 2022;12(1):2605.
Qiu D, **a Z, Deng J, Jiao X, Liu L, Li J. Glucorticoid-induced obesity individuals have distinct signatures of the gut microbiome. Bio Factors. 2019;45(6):892–901.
Zhao H, Jiang X, Chu W. Shifts in the gut microbiota of mice in response to dexamethasone administration. Int Microbiol. 2020;23(4):565–73.
Guo M, Wang H, Xu S, Zhuang Y, An J, Su C, **a Y, Chen J, Xu ZZ, Liu Q, et al. Alteration in gut microbiota is associated with dysregulation of cytokines and glucocorticoid therapy in systemic lupus erythematosus. Gut Microbes. 2020;11(6):1758–73.
Wang M, Zhu Z, Lin X, Li H, Wen C, Bao J, He Z. Gut microbiota mediated the therapeutic efficacies and the side effects of prednisone in the treatment of MRL/lpr mice. Arthritis Res Ther. 2021;23(1):240.
Huang EY, Inoue T, Leone VA, Dalal S, Touw K, Wang Y, Musch MW, Theriault B, Higuchi K, Donovan S, et al. Using corticosteroids to reshape the gut microbiome: implications for inflammatory bowel diseases. Inflamm Bowel Dis. 2015;21(5):963–72.
Garden OA, Kidd L, Mexas AM, Chang YM, Jeffery U, Blois SL, Fogle JE, MacNeill AL, Lubas G, Birkenheuer A, et al. ACVIM consensus statement on the diagnosis of immune-mediated hemolytic anemia in dogs and cats. J Vet Intern Med. 2019;33(2):313–34.
Makielski KM, Brooks MB, Wang C, Cullen JN, O’Connor AM, LeVine DN. Development and implementation of a novel immune thrombocytopenia bleeding score for dogs. J Vet Intern Med. 2018;32(3):1041–50.
Swann JW, Garden OA, Fellman CL, Glanemann B, Goggs R, LeVine DN, Mackin AJ, Whitley NT. ACVIM consensus statement on the treatment of immune-mediated hemolytic anemia in dogs. J Vet Intern Med. 2019;33(3):1141–72.
Kozich JJ, Westcott SL, Baxter NT, Highlander SK, Schloss PD. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Appl Environ Microbiol. 2013;79(17):5112–20.
Bolyen E, Rideout JR, Dillon MR, Bokulich NA, Abnet CC, Al-Ghalith GA, Alexander H, Alm EJ, Arumugam M, Asnicar F, et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat Biotechnol. 2019;37(8):852–7.
Callahan BJ, McMurdie PJ, Rosen MJ, Han AW, Johnson AJ, Holmes SP. DADA2: High-resolution sample inference from Illumina amplicon data. Nat Methods. 2016;13(7):581–3.
Rosen MJ, Callahan BJ, Fisher DS, Holmes SP. Denoising PCR-amplified metagenome data. BMC Bioinform. 2012;13:283.
Rognes T, Flouri T, Nichols B, Quince C, Mahe F. VSEARCH: a versatile open source tool for metagenomics. PeerJ. 2016;4: e2584.
Bokulich NA, Kaehler BD, Rideout JR, Dillon M, Bolyen E, Knight R, Huttley GA, Gregory Caporaso J. Optimizing taxonomic classification of marker-gene amplicon sequences with QIIME 2’s q2-feature-classifier plugin. Microbiome. 2018;6(1):90.
Quast C, Pruesse E, Yilmaz P, Gerken J, Schweer T, Yarza P, Peplies J, Glockner FO. The SILVA ribosomal RNA gene database project: improved data processing and web-based tools. Nucleic Acids Res. 2013;41:D590-596.
Yilmaz P, Parfrey LW, Yarza P, Gerken J, Pruesse E, Quast C, Schweer T, Peplies J, Ludwig W, Glockner FO. The SILVA and “All-species Living Tree Project (LTP)” taxonomic frameworks. Nucleic Acids Res. 2014;42:D643-648.
Po-Yu Liu. poyuliu/MARco: MARco: Microbiome Analysis RcodeDB (Version v1.0). Zenodo. 2021. https://doi.org/10.5281/zenodo.4589898.
Oksanen J, Blanchet FG, Kindt R, Legendre P, Minchin PR, O'Hara RB, Simpson GL, Solymos P, Stevens MHH, Wagner H: vegan: community ecology package. R package version 2.3–1. In. Oulu, Finland; 2015.
Kolde R: pheatmap: Pretty heatmaps. R package version 1.0.8. In.; 2015.
R Core Team: R: A language and environment for statistical computing. In.: R Foundation for Statistical Computing, Vienna, Austria; 2015.
Lozupone C, Knight R. UniFrac: a new phylogenetic method for comparing microbial communities. Appl Environ Microbiol. 2005;71(12):8228–35.
Lozupone C, Lladser ME, Knights D, Stombaugh J, Knight R. UniFrac: an effective distance metric for microbial community comparison. Isme J. 2011;5(2):169–72.
Funding
This work was generously funded by an intramural grant from the Center for Host-Microbial Interactions at the School of Veterinary Medicine, University of Pennsylvania.
Author information
Authors and Affiliations
Contributions
OAG, DB, and KM conceived, designed, and managed the study. KM, AB, JC, HC, RM, EK, EL, DL, CF, and RG recruited, collected, and submitted patient and control samples. SM and DB processed fecal samples and undertook 16S rRNA gene sequencing and initial analysis of data. P-YL and DX completed detailed analysis of the data and generated the figures. P-YL and OAG wrote the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All animal work was carried out in accordance with the guidelines of the Institutional Animal Care and Use Committees of the participating centers. Signed owner consent was obtained before the recruitment of case and control dogs to the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Figure S1
. Comparison of the diversity of gut microbiota between dogs receiving antimicrobials (22 samples from 15 diseased dogs collected at baseline, week 2, and week 8) and dogs not receiving antimicrobials (36 samples without record of antimicrobial administration during the study period). No statistically significant difference between the two groups was observed (p = 0.21 by PERMANOVA). Numbers on the symbols represent treatment duration (days). Figure S2 Baseline dogs’ gut microbiota profile at (A) phylum, (B) class, and (C) genus levels among healthy in-contact controls (Healthy, C), healthy non-in-contact controls (Healthy, NC), and IMHA and ITP dogs. IMHA: immune-mediated hemolytic anemia, ITP: immune thrombocytopenia. Figure S3 Treatment flow chart for IMHA. Figure S4 Treatment flow chart for ITP. Table S1 Immune-mediated hematological disease odds ratios of differentially abundant taxa between healthy and diseased dogs. Table S2 Inclusion/exclusion criteria applied in the study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, PY., **a, D., McGonigle, K. et al. Immune-mediated hematological disease in dogs is associated with alterations of the fecal microbiota: a pilot study. anim microbiome 5, 46 (2023). https://doi.org/10.1186/s42523-023-00268-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42523-023-00268-2