
Abstract
Background
Tracking combinations of lifestyle behaviours during childhood (“lifestyle pattern trajectories”) can identify subgroups of children that might benefit from lifestyle interventions aiming to improve health outcomes later in life. However, studies on the critical transition period from early to middle childhood are limited. We aimed to describe lifestyle patterns trajectories in children from 2 to 8 years of age and evaluated their associations with cardiometabolic risk markers at age 8 years in a multi-ethnic Asian cohort.
Methods
Twelve lifestyle behaviours related to child’s diet, physical activity, screen use, and sleep were ascertained using questionnaires at ages 2, 5, and 8 years. Age-specific lifestyle patterns were derived using principal component analysis and trajectories were determined using group-based multi-trajectory modelling. Child cardiometabolic risk markers were assessed at age 8 years, and associations with trajectories examined using multiple regression, adjusted for confounders.
Results
Among 546 children, two lifestyle patterns “healthy” and “unhealthy” were observed at ages 2, 5, and 8 years separately. Three trajectory groups from 2 to 8 years were identified: consistently healthy (11%), consistently unhealthy (18%), and mixed pattern (71%). Children in the consistently unhealthy group (vs. mixed pattern) had increased odds of pre-hypertension (OR = 2.96 [95% CI 1.18–7.41]) and higher levels of diastolic blood pressure (β = 1.91 [0.27–3.55] mmHg), homeostasis model assessment of insulin resistance (β = 0.43 [0.13–0.74]), triglycerides (β = 0.11 [0.00-0.22] mmol/L), and metabolic syndrome score (β = 0.85 [0.20–1.49]), but not with BMI z-score or any anthropometric measurements. The consistently healthy group showed no differences in cardiometabolic outcomes compared to the mixed pattern group.
Conclusion
Three distinct lifestyle pattern trajectories were identified from early to middle childhood. Children in the consistently unhealthy lifestyle group did not have a raised BMI but was associated with several elevated cardiometabolic risk markers. These findings suggest the potential benefits of initiating holistic lifestyle interventions to improve children’s health and well-being from an early age.
Trial registration
Trial registration number: NCT01174875. Name of registry: ClinicalTrials.gov. URL of registry: https://classic.clinicaltrials.gov/ct2/show/NCT01174875. Date of registration: August 4, 2010. Date of enrolment of the first participant to the trial: June 2009.
Similar content being viewed by others

Background
The rising prevalence of adverse cardiometabolic profiles in children is concerning due to long-term health implications [1]. A meta-analysis of prospective cohort studies suggests that a holistic approach adopting multiple healthy lifestyle behaviours (e.g., better diet quality, increased physical activity, decreased sedentary time, and optimal sleep) acts synergistically to reduce cardiovascular risk, particularly in young adults [2]. However, these studies typically assess lifestyle behaviours at a single time point without quantifying the risk associated with lifestyle changes (or trajectories) over time.
Lifestyle changes can occur at any stage of life, even within the childhood period [3]. Establishment of lifestyle habits often happens before 3 years of age [3]. A sedentary-snacking pattern, characterized by high consumption of energy-dense or processed foods coupled with excessive screen time, is frequently observed and established as early as age 18 months [4,5,6]. When children enter primary school, around the age of 6–7 years, their lifestyle behaviours may remain stable or undergo changes due to peer influence and other environmental factors [3, 7]. Studying how combinations of lifestyle behaviours track over childhood (also known as lifestyle pattern trajectories) provides valuable insights into subgroups of children that might benefit from lifestyle interventions to improve health, including metabolic outcomes, later in life.
A growing number of studies have adopted the group-based multi-trajectory modelling approach [8, 9]. This method enables the identification of groups of children that follow similar lifestyle trajectories across multiple behaviours of interest. However, existing studies on trajectories of multiple lifestyle behaviours in children have primarily focused on either early childhood (4 to 60 months) [8, 9] or middle childhood to adolescence (7 to 19 years of age) [10,11,12,13,14], with limited research on the critical transition period from early to middle childhood [15, 16]. Furthermore, these studies predominantly focused on movement behaviours, such as physical activity and screen time, but did not study diet and movement behaviours collectively.
While most existing studies aim to characterise lifestyle pattern trajectories and identify their correlates [8,9,10,11,12, 16], fewer relate to risk markers for health outcomes [13,14,15]. Only one study in the UK observed that children following trajectories of high moderate-to-vigorous intensity physical activity and low sedentary behaviour from 7 to 15 years of age had lower fat mass index in late adolescence [14]. However, no previous studies have assessed associations with cardiometabolic risk markers like insulin sensitivity and paediatric metabolic syndrome score during childhood, which may provide further insights on the early origins of cardiometabolic diseases.
To address these gaps, we aimed to identify distinct lifestyle pattern trajectories from early to middle childhood (ages 2 to 8 years) and examine their associations with cardiometabolic risk markers at age 8 years in a multi-ethnic Asian cohort.
Methods
Study population
We studied children from the Growing Up in Singapore Towards healthy Outcomes (GUSTO) prospective mother-offspring cohort study. Briefly, 1450 pregnant women were recruited at 7 to 11 weeks of pregnancy from two public maternity units in Singapore between 2009 and 2010 [17]. Inclusion criteria were women aged 18 years and above, Singapore Citizens or Singapore Permanent Residents, willingness to donate cord, cord blood, and placenta, intending to deliver in the study hospitals and reside in Singapore for the next 5 years, and foetus with both sets of grandparents of the same ethnicity. Women on chemotherapy or with significant health conditions, such as type 1 diabetes and psychosis, were excluded. The study was approved by the National Health Care Group Domain Specific Review Board (D/09/021 and B/2014/00406) and the SingHealth Centralized Institutional Review Board (2018/2767/D and 2009/291/D). Informed written consent was obtained from all participants.
Lifestyle behaviours
We considered 12 lifestyle behaviours related to the child’s diet and movement behaviours based on existing studies examining lifestyle trajectories in children [8,9,10,11,12,13,14,15,16]. Movement behaviours include screen time, outdoor play, MVPA, participation in organized physical activity, and sleep duration.
Dietary intake
Caregivers (mostly mothers) reported the frequency of food items consumed by their child over the past month using validated food frequency questionnaires at ages 1.5 [18], 5 [19], and 7 years [20]. The data were converted to daily frequencies and categorized into seven food or drink groups, namely fruit, vegetables, processed meat, fast food, sweet snacks, savoury snacks, and sugar sweetened beverages (SSBs) at each time point.
Movement behaviours
At age 2 years, caregivers reported the amount of time their child spent on screen use (television, computers, mobile devices, and gaming consoles) and outdoor play on a typical weekday and weekend day over the past month [21, 22]. At ages 5.5 and 8 years, caregivers reported the amount of time their child spent on screen use, outdoor play, and MVPA on the most recent weekday and weekend day using validated preschool-age and school-age physical activity questionnaire [23]. The reported durations for weekdays and weekends were then weighted to calculate the daily average durations. Caregivers also reported the amount of time their child spent on organized physical activity during the week at age 5.5 and 8 years. Outdoor play at age 2 years was used as a surrogate marker for physical activity since there were no MVPA and organized physical activity data at such a young age. This proxy marker is commonly used in the literature [8].
At age 1.5 years, mothers reported day and night sleep durations of their child through the Brief Infant Sleep Questionnaire [24]. At ages 5.5 and 8 years, night sleep duration was reported on a typical weekday and weekend day over the past week through the Child Sleep Habits Questionnaire, weighted to an average day subsequently [25].
Identifying patterns of lifestyle behaviours
Principal component analysis (PCA) with varimax rotation was applied to derive lifestyle patterns at ages 2, 5, and 8 years separately. The method is detailed elsewhere [26]. In brief, PCA is a data reduction method that combines correlated standardised variables (here: the 12 lifestyle behaviours) into a smaller set of patterns (here: lifestyle patterns), while preserving as much information as possible. The Kaiser-Meyer-Olkin test statistics for sampling adequacy at Year 2, Year 5, and Year 8 were 0.70, 0.63, and 0.66, respectively. These indicate that the sampling was adequate for PCA. In addition, the Bartlett’s test of sphericity produced a statistically significant chi-square value to justify the application of PCA.
Two consistent lifestyle patterns were identified (See Supplementary Table 1, Additional File 1) and they were subsequently used to derive trajectories. Based on absolute PCA loadings > 0.20, the first pattern was characterized by high intakes of processed meat, fast food, sweet snacks, savoury snacks, SSBs, and screen time. The second pattern was characterized by high intakes of fruit and vegetables, low screen time, and high MVPA, outdoor play, and participation in organized physical activity. The pattern scores for each child was calculated by summing the standardized values of each lifestyle behaviour weighted to its PCA loading. A higher score on the first pattern suggests a less healthy lifestyle, while a higher score on the second pattern suggests a healthier lifestyle. For simplicity, we named them as “unhealthy” and “healthy” patterns.
Cardiometabolic outcomes at age 8 years
Anthropometrics
Trained research staff measured the standing height (seca 213 Stadiometer, seca GmbH & Co., Hamburg, Germany), weight (seca 803 weighing scale), abdominal circumference (measuring tape), and skinfold thicknesses (triceps, biceps, subscapular, and suprailiac skinfolds) from the right side of the body (Holtain skinfold calipers, Holtain Ltd, Pembrokeshire, UK). We calculated the sum of skinfold thicknesses measured at the four sites and derived the sex- and age-specific BMI z-scores using the World Health Organization growth standards [27].
Blood pressure
Peripheral systolic and diastolic blood pressure were measured from the right upper arm (Dinamap CARESCAPE V100, GE Healthcare, Milwaukee, WI). An average of two readings was calculated if the difference between readings was less than 10 mmHg; otherwise, a third reading was taken and the average of the three readings used instead. Pre-hypertension for children was defined as ≥ 110/70 mmHg, which has been shown to predict the risk of adult hypertension and subclinical cardiovascular disease [28].
Laboratory measures
Fasting blood was drawn to measure plasma glucose (Abbott Architect c8000 analyzer at KK Women’s and Children’s Hospital, and Beckman AU5800 analyzer at National University Hospital), serum insulin (Beckman DXL800 analyzer, Beckman Coulter, Brea, CA), high density lipoprotein cholesterol (Beckman AU5800 analyzer), triglycerides, and gamma-glutamyl-transferase (Beckman AU5800 analyzer). Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as follows [29]: fasting insulin (mU/L) * fasting glucose (mmol/L) / 22.5.
Prediction indices
Paediatric metabolic syndrome score was calculated based on a published approach using sex- and cohort-specific z-scores of abdominal circumference, systolic blood pressure, diastolic blood pressure, HOMA-IR, triglycerides, and high density lipoprotein cholesterol [30].
Fatty liver index was calculated based on a published algorithm using BMI, abdominal circumference, triglycerides, and gamma-glutamyl-transferase [31]. The index has been validated against ultrasonography and has shown good performance for predicting fatty liver.
Covariates
A priori determined covariates were selected as they have been identified as correlates of lifestyle behaviours [8, 9, 12, 15] and/or cardiometabolic outcomes in childhood [32, 33]. A detailed description of the covariates is presented in Supplementary Information, Additional File 1. In brief, covariates were either obtained from clinical records or collected by questionnaires administered during recruitment (7–11 weeks’ gestation), pregnancy (26–28 weeks’ gestation) and at different stages of the follow-up (from ages 3 months to 8 years). They were subsequently categorized into maternal, paternal, pregnancy, offspring, and postnatal characteristics.
Statistical analysis
We used group-based multi-trajectory modelling to identify lifestyle patterns trajectories across three time points at ages 2, 5, and 8 years [34]. Participants who had missing data for more than one time point were excluded. The optimal number of latent classes and trajectory shapes (i.e. linear, quadratic, cubic) were selected based on Bayesian Information Criteria, adequate sample size in each class, odds of correct classification, model parsimony, and distinctiveness and interpretability of trajectories via visual inspection. The model fit statistics for various trajectory shapes within 2- to 4-class solutions were shown in Supplementary Table 2, Additional File 1.
To understand the profile of children in the various trajectories, covariates (i.e., maternal, paternal, pregnancy, offspring, and postnatal characteristics) were summarised by trajectory groups. Fisher’s exact test and ANOVA were used to compare the differences in characteristics across trajectory groups.
Associations between lifestyle pattern trajectories and cardiometabolic outcomes were performed by linear regression for continuous outcomes and logistic regression for pre-hypertension. We adjusted for factors associated with both lifestyle behaviours and cardiometabolic outcomes in childhood (maternal age, ethnicity, educational attainment, household income, family history of cardiovascular disease, pre-pregnancy BMI, father’s BMI, child sex, birth order, preterm birth,). Blood pressure analyses were further adjusted for child height at the age of 8 years.
The percentage missing on confounders ranged from 0.4 to 9% and they were imputed using chained equations which included all exposures, outcomes, and covariates as predictors. We generated 20 imputed datasets and results of the pooled analyses were presented. We had missing data for cardiometabolic outcomes ranging from 2.9 to 30% owing to differential consent for anthropometrics, blood pressure, and laboratory measurements. Complete case and outcome analyses (participants without missing confounders and outcomes, n = 294) were performed as sensitivity analysis.
All statistical analyses were carried out using Stata 17 (StataCorp LP, USA). P < 0.05 was considered statistically significant.
Results
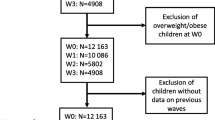
Among 1181 singleton deliveries, 169 children were lost to follow-up and 466 had incomplete lifestyle behaviour data for more than one timepoint, resulting in 546 children for the present analysis (Fig. 1). Children excluded from the analysis did not differ by sex, birth order, or birth size, however, they were more likely of Indian ethnicity, born preterm, to younger and less educated mothers (See Supplementary Table 3, Additional File1).

Flowchart of participants
Lifestyle pattern trajectories
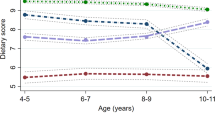
We identified three distinct lifestyle pattern trajectories from 2 to 8 years of age: consistently healthy (11%), consistently unhealthy (18%), and mixed pattern (71%) (Fig. 2). The consistently healthy group maintained a stable-low level for the unhealthy pattern and a high-increasing trend for the healthy pattern throughout the 6-year follow-up. Conversely, the consistently unhealthy group displayed a stable-low level for the healthy pattern and a high-increasing trend for the unhealthy pattern.

Identified three trajectory groups from two lifestyle patterns. Group 1: Consistently healthy; Group 2: Mixed pattern; Group 3: Consistently unhealthy. Abbreviations: PCA, Principal component analysis. Unhealthy pattern was characterized by high intakes of processed meat, fast food, sweet snacks, savoury snacks, sugar sweetened beverages, and screen time. Healthy pattern was characterized by high intakes of fruit and vegetables, low screen time, and high moderate-to-vigorous physical activity, outdoor play, and participation in organized physical activity. The consistently healthy group maintained a stable-low level for the unhealthy pattern, and a high-increasing trend for the healthy pattern. The consistently unhealthy group displayed a stable-low level for the healthy pattern, and a high-increasing trend for the unhealthy pattern. The mixed pattern revealed a stable-low trajectory for both healthy and unhealthy patterns
The mixed trajectory exhibited stable-low level for both patterns. A comparison of individual lifestyle behaviours by trajectory groups revealed that children in this group had lower intakes of fruit and vegetables and were less active compared to the consistently healthy group. However, they consumed less discretionary foods and had lower screen time compared to the consistently unhealthy group (See Supplementary Table 4, Additional File 1).
Characteristics of study population by trajectory groups
Children in the consistently unhealthy group tended to be of Malay ethnicity, had shorter breastfeeding duration, had parents with lower educational attainment and lower household income, and had mothers who exhibited suboptimal lifestyle during pregnancy (i.e., poor diet, physically inactive, poor sleep quality, higher television viewing time, and higher tobacco exposure). Conversely, children in the consistently healthy group tended to be breastfed longer, had higher proportion of parents with university degrees and higher household income, and born to mothers who had more optimal lifestyle during pregnancy (Table 1).
Association of childhood lifestyle pattern trajectories and cardiometabolic outcomes
After adjusting for confounders, children in the consistently unhealthy group (vs. mixed pattern) had increased odds of pre-hypertension (OR = 2.96 [95% CI 1.18–7.41]) and higher levels of diastolic blood pressure (β = 1.91 [0.27–3.55] mmHg), fasting insulin (β = 13.7 [4.24–23.2] pmol/L), HOMA-IR (β = 0.43 [0.13–0.74]), triglycerides (β = 0.11 [0.00-0.22] mmol/L), and metabolic syndrome score (β = 0.85 [0.20–1.49]), but not with any anthropometric measurements (Table 2). The consistently healthy group showed no differences in cardiometabolic outcomes compared to the mixed pattern group (Table 2).
Similar direction of associations were found between the consistently healthy and consistently unhealthy groups (Supplementary Table 5) and in complete-case and -outcome analyses (Supplementary Table 6).
Discussion
To our knowledge, this study is the first to identify lifestyle pattern trajectories from early to middle childhood and cardiometabolic risk factors in children. We found three distinct lifestyle pattern trajectories. Only 11% of the children were categorized in the consistently healthy group, whereas nearly one-fifth belonged to the consistently unhealthy group. The majority exhibited mixed healthy and unhealthy lifestyle pattern trajectories. Children in the consistently unhealthy group had increased odds of pre-hypertension and higher levels of diastolic blood pressure, fasting insulin, HOMA-IR, triglycerides, and metabolic syndrome score at 8 years of age.
The study identified distinct lifestyle pattern trajectories with variability in multiple lifestyle behaviours. Majority of children (71%) exhibited a mixed pattern trajectory, characterised by low physical activity, moderate screen time, and low intakes of fruit, vegetables, and discretionary foods. Consistent with longitudinal data of Spanish youth [11], 75% of the children had low MVPA and slight increase in sedentary behaviour over time. Only one study in Australia examined diet and movement behaviours collectively and they reported that 53% of children belonged to the trajectory group with healthy lifestyle patterns during a follow-up period from 18 to 60 months [9]. This reported percentage is notably higher than our findings (11%). However, it is important to note that the study in Australia primarily focused on early childhood and it is unclear whether the healthy pattern persist into middle childhood when children enter primary school. Further investigations are warranted, particularly in studies with extended follow-up periods, to gain deeper insights into the factors influencing the persistence of healthy lifestyle patterns in children over time.
We noted relatively lower PCA loadings for screen time and sleep variables during the identification of lifestyle patterns, suggesting that screen time and sleep make a smaller contribution to the overall lifestyle pattern. Notably, sleep duration in children has been shown to track poorly [35]. A study involving children aged 3 to 7 years revealed that sleep patterns in children are not particularly stable, showing considerable variation both within a week and across the years.
Children in the consistently unhealthy group exhibited a cluster of cardiometabolic risk markers at 8 years of age, despite having similar BMI and anthropometric measurements as children in the mixed trajectory group, which aligns with the Asian metabolic phenotype [36]. Previous studies have not assessed associations between trajectories of multiple lifestyle behaviours and cardiometabolic risk markers in childhood. Only one study in the UK reported that children with high MVPA and low sedentary time throughout 7 to 15 years of age had lower fat mass index in late adolescence, but no direct relationship with BMI was observed [14]. Studies assessing lifestyle behaviours at a single time point also showed inconsistent BMI results [37]. Younger children are hypothesized to have better energy compensation abilities than older children and adults [38], suggesting that children with unhealthy lifestyle may not always lead to weight gain. Therefore, our study underscores the importance of measuring various cardiometabolic risk markers, alongside BMI, to detect early cardiometabolic risk in children.
It is also noteworthy that certain cardiometabolic risk markers such as fasting glucose and liver fat were not elevated in the consistently unhealthy group; this may be because differences only emerge gradually over time and may be more pronounced after puberty [39]. Nonetheless, our study provides novel insights on the early development of metabolic abnormalities as we found concomitant increases in blood pressure, insulin resistance, triglycerides, and metabolic syndrome score among 8-year-old children. As cardiometabolic risk factor clustering is predictive of future cardiovascular disease [40], our results highlight the clinical significance of promoting healthy behaviours from a young age, especially in children with consistently unhealthy lifestyle behaviours, to prevent adverse metabolic outcomes later in life.
Consistent with previous studies [8, 9, 26], children in the consistently unhealthy group tended to be of Malay ethnicity, had shorter breastfeeding duration, had parents with lower educational attainment and lower household income, and had mothers who exhibited suboptimal lifestyle during pregnancy. The prenatal period has been recognised as a time when women may be more receptive to changing their health behaviours [41]. Targeting positive behaviour change during pregnancy, which often continues after childbirth and integrated into family routines, may be effective in promoting healthier lifestyles for children. Alongside individual-level interventions, it is crucial to incorporate structural measures, such as social and community support, to empower families, particularly those experiencing social disadvantage, to adopt healthy behavioural trajectories.
Strengths of our study include repeated measures of multiple lifestyle behaviours across early and middle childhood, the use of group-based multi-trajectory modelling to summarize complex longitudinal data, and the evaluation of a comprehensive panel of cardiometabolic risk markers at the age of 8 years to capture any early subclinical changes in cardiometabolic profile.
Some study limitations are worth noting. First, data on children’s lifestyle behaviours were caregiver-reported. Nevertheless, measurement errors are more likely non-differential since cardiometabolic outcomes were collected prospectively. Moreover, the tools for assessing these child behaviours have shown good validity and used in past research [18,19,20,21,22,23,24,25]. Second, the small sample size of the consistently healthy group (n = 59) may limit the power to detect associations with cardiometabolic risk markers. Third, a significant proportion of children in the mixed pattern trajectory (71%) could also be due to “regression to the mean” [42] where children tended to gravitate towards the mean if behaviours were measured repeatedly over time. Fourth, the evaluation of multiple cardiometabolic outcomes raises the possibility of false-positive results, but the consistency of associations across related outcomes reduces this concern. Fifth, children excluded from the analysis tended to be of Indian ethnicity, born preterm, to younger and less educated mothers. These characteristics may limit generalisability of our study. Sixth, although we adjusted for many confounders, our findings could still be influenced by residual and unmeasured covariates (e.g., environment and social factors). Last, causality cannot be claimed as in any single observational study, but the longitudinal design allowed us to establish temporality between the exposures and the outcomes.
Conclusions
In conclusion, we identified three distinct lifestyle pattern trajectories from early to middle childhood, with nearly one-fifth of the children belonging to a consistently unhealthy group. These children did not have a raised BMI but exhibited a cluster of cardiometabolic risk markers, characterized by increased odds of pre-hypertension and elevated levels of diastolic blood pressure, markers of insulin resistance, triglycerides, and metabolic syndrome score. Our findings suggest the potential benefits of initiating holistic lifestyle interventions, involving parents and families, to improve children’s health and well-being from an early age.
Data availability
Data described in the manuscript and analytic code can be made available upon request after approval from our study executives.
Abbreviations
- GUSTO:
-
Growing Up in Singapore Towards healthy Outcomes
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- MVPA:
-
Moderate-to-vigorous physical activity
- PCA:
-
Principal component analysis
- SSBs:
-
Sugar sweetened beverages
References
Noubiap JJ, Nansseu JR, Lontchi-Yimagou E, Nkeck JR, Nyaga UF, Ngouo AT, et al. Global, regional, and country estimates of metabolic syndrome burden in children and adolescents in 2020: a systematic review and modelling analysis. The Lancet Child & Adolescent Health. 2022;6(3):158–70.
Tsai M-C, Lee C-C, Liu S-C, Tseng P-J, Chien K-L. Combined healthy lifestyle factors are more beneficial in reducing cardiovascular disease in younger adults: a meta-analysis of prospective cohort studies. Sci Rep. 2020;10(1):18165.
Chong MF-F. Dietary trajectories through the life course: opportunities and challenges. Br J Nutr. 2022;128(1):154–9.
Lioret S, Campbell KJ, McNaughton SA, Cameron AJ, Salmon J, Abbott G et al. Lifestyle patterns begin in early childhood, persist and are socioeconomically patterned, confirming the importance of early life interventions. Nutrients. 2020;12(3).
Bel-Serrat S, Mouratidou T, Santaliestra-Pasías AM, Iacoviello L, Kourides YA, Marild S, et al. Clustering of multiple lifestyle behaviours and its association to cardiovascular risk factors in children: the IDEFICS study. Eur J Clin Nutr. 2013;67(8):848–54.
Lioret S, Touvier M, Lafay L, Volatier JL, Maire B. Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. J Nutr. 2008;138(1):101–7.
Padmapriya N, Chen B, Goh CMJL, Shek LPC, Chong YS, Tan KH, et al. 24-hour movement behaviour profiles and their transition in children aged 5.5 and 8 years– findings from a prospective cohort study. Int J Behav Nutr Phys Activity. 2021;18(1):145.
Downing KL, del Pozo Cruz B, Sanders T, Zheng M, Hnatiuk JA, Salmon J, et al. Outdoor time, screen time and sleep reported across early childhood: concurrent trajectories and maternal predictors. Int J Behav Nutr Phys Activity. 2022;19(1):160.
Zheng M, Lioret S, Hesketh KD, Spence A, Taylor R, Campbell KJ. Association between Longitudinal Trajectories of Lifestyle Pattern and BMI in early childhood. Obes (Silver Spring). 2021;29(5):879–87.
Gallant F, Thibault V, Hebert J, Gunnell KE, Bélanger M. One size does not fit all: identifying clusters of physical activity, screen time, and sleep behaviour co-development from childhood to adolescence. Int J Behav Nutr Phys Activity. 2020;17(1):58.
Parker K, Timperio A, Salmon J, Villanueva K, Brown H, Esteban-Cornejo I, et al. Correlates of dual trajectories of physical activity and sedentary time in youth: the UP & DOWN longitudinal study. Scand J Med Sci Sports. 2021;31(5):1126–34.
Hanson SK, Munthali RJ, Micklesfield LK, Lobelo F, Cunningham SA, Hartman TJ, et al. Longitudinal patterns of physical activity, sedentary behavior and sleep in urban South African adolescents, Birth-To-Twenty plus cohort. BMC Pediatr. 2019;19(1):241.
Zhang A, Fang J, Wan Y, Su P, Tao F, Sun Y. Joint trajectories of life style indicators and their links to psychopathological outcomes in the adolescence. BMC Psychiatry. 2021;21(1):407.
Farooq A, Basterfield L, Adamson AJ, Pearce MS, Hughes AR, Janssen X et al. Moderate-To-Vigorous intensity physical activity and sedentary Behaviour across Childhood and Adolescence, and their combined relationship with obesity risk: a multi-trajectory analysis. Int J Environ Res Public Health. 2021;18(14).
del Pozo-Cruz B, Perales F, Parker P, Lonsdale C, Noetel M, Hesketh KD, et al. Joint physical-activity/screen-time trajectories during early childhood: socio-demographic predictors and consequences on health-related quality-of-life and socio-emotional outcomes. Int J Behav Nutr Phys Activity. 2019;16(1):55.
Kwon S, Janz KF, Letuchy EM, Burns TL, Levy SM. Developmental trajectories of physical activity, sports, and television viewing during childhood to Young Adulthood: Iowa Bone Development Study. JAMA Pediatr. 2015;169(7):666–72.
Soh S-E, Tint MT, Gluckman PD, Godfrey KM, Rifkin-Graboi A, Chan YH, et al. Cohort Profile: growing up in Singapore towards healthy outcomes (GUSTO) birth cohort study. Int J Epidemiol. 2013;43(5):1401–9.
Lim HX, Toh JY, Tan KH, Chong Y-S, Yap F, Godfrey KM, et al. Validation of a semi-quantitative FFQ for 18-month-old toddlers: the growing up in Singapore towards healthy outcomes (GUSTO) study. Public Health Nutr. 2019;22(11):1990–2000.
Sugianto R, Chan MJ, Wong SF, Shek LP, Tan KH, Chong YS, et al. Evaluation of a quantitative food frequency questionnaire for 5-Year-old children in an Asian Population. J Acad Nutr Diet. 2020;120(3):437–44.
Lai JS, Loh J, Toh JY, Sugianto R, Colega M, Tan KH, et al. Evaluation of paper-based and web-based food frequency questionnaires for 7-year-old children in Singapore. Br J Nutr. 2022;128(8):1626–37.
Bernard JY, Padmapriya N, Chen B, Cai S, Tan KH, Yap F, et al. Predictors of screen viewing time in young Singaporean children: the GUSTO cohort. Int J Behav Nutr Phys Activity. 2017;14(1):112.
Chua SYL, Ikram MK, Tan CS, Lee YS, Ni Y, Shirong C, et al. Relative contribution of risk factors for early-onset myopia in young Asian children. Investig Ophthalmol Vis Sci. 2015;56(13):8101–7.
Chen B, Bernard JY, Padmapriya N, Yao J, Goh C, Tan KH, et al. Socio-demographic and maternal predictors of adherence to 24-hour movement guidelines in Singaporean children. Int J Behav Nutr Phys Activity. 2019;16(1):1–11.
Zhou Y, Aris IM, Tan SS, Cai S, Tint MT, Krishnaswamy G, et al. Sleep duration and growth outcomes across the first two years of life in the GUSTO study. Sleep Med. 2015;16(10):1281–6.
Tham EK, Xu H-Y, Fu X, Schneider N, Goh DY, Lek N, et al. Variations in longitudinal sleep duration trajectories from infancy to early childhood. Sleep Health. 2021;7(1):56–64.
Chia A, Descarpentrie A, Cheong RN, Toh JY, Natarajan P, Sugianto R, et al. Family-focused contextual factors associated with lifestyle patterns in young children from two mother-offspring cohorts: GUSTO and EDEN. Int J Behav Nutr Phys Activity. 2022;19(1):1–13.
Organization WH, Organization WH, WHO Multicentre Growth Reference Study Group.: WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva: WHO. 2006;2007.
** B, Zhang T, Li S, Harville E, Bazzano L, He J, et al. Can Pediatric Hypertension Criteria be simplified? A prediction analysis of Subclinical Cardiovascular outcomes from the Bogalusa Heart Study. Hypertension. 2017;69(4):691–6.
Matthews DR, Hosker JP, Rudenski AS, Naylor B, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9.
Ahrens W, Moreno L, Mårild S, Molnár D, Siani A, De Henauw S, et al. Metabolic syndrome in young children: definitions and results of the IDEFICS study. Int J Obes. 2014;38(2):4–S14.
Bedogni G, Bellentani S, Miglioli L, Masutti F, Passalacqua M, Castiglione A, et al. The fatty liver index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6:1–7.
Ong YY, Pang WW, Michael N, Aris IM, Sadananthan SA, Tint M-T, et al. Timing of introduction of complementary foods, breastfeeding, and child cardiometabolic risk: a prospective multiethnic Asian cohort study. Am J Clin Nutr. 2023;117(1):83–92.
Huang JY, Cai S, Huang Z, Tint MT, Yuan WL, Aris IM, et al. Analyses of child cardiometabolic phenotype following assisted reproductive technologies using a pragmatic trial emulation approach. Nat Commun. 2021;12(1):5613.
Nagin DS, Jones BL, Passos VL, Tremblay RE. Group-based multi-trajectory modeling. Stat Methods Med Res. 2018;27(7):2015–23.
Taylor RW, Williams SM, Farmer VL, Taylor BJ. The stability of sleep patterns in children 3 to 7 years of age. J Pediatr. 2015;166(3):697–702e1.
Bhardwaj S, Misra A. Obesity, diabetes and the Asian phenotype. Nutrition for the primary care provider. Volume 111. Karger Publishers; 2015. pp. 116–22.
D’Souza NJ, Kuswara K, Zheng M, Leech R, Downing KL, Lioret S, et al. A systematic review of lifestyle patterns and their association with adiposity in children aged 5–12 years. Obes Rev. 2020;21(8):e13029.
Cecil JE, Palmer CN, Wrieden W, Murrie I, Bolton-Smith C, Watt P, et al. Energy intakes of children after preloads: adjustment, not compensation. Am J Clin Nutr. 2005;82(2):302–8.
Maffeis C, Morandi A. Body composition and insulin resistance in children. Eur J Clin Nutr. 2018;72(9):1239–45.
Camhi SM, Katzmarzyk PT. Tracking of cardiometabolic risk factor clustering from childhood to adulthood. Int J Pediatr Obes. 2010;5(2):122–9.
Olander EK, Smith DM, Darwin Z. Health behaviour and pregnancy: a time for change. J Reproductive Infant Psychol. 2018;36(1):1–3.
Barnett AG, Van Der Pols JC, Dobson AJ. Regression to the mean: what it is and how to deal with it. Int J Epidemiol. 2005;34(1):215–20.
Acknowledgements
The authors would like to thank the GUSTO study group, which includes Airu Chia, Andrea Cremaschi, Anna Magdalena Fogel, Anne Eng Neo Goh, Anne Rifkin-Graboi, Anqi Qiu, Arijit Biswas, Bee Wah Lee, Birit Froukje Philipp Broekman, Candida Vaz, Chai Kiat Chng, Chan Shi Yu, Choon Looi Bong, Daniel Yam Thiam Goh, Dawn **n ** Koh, Dennis Wang, Desiree Y. Phua, E Shyong Tai, Elaine Kwang Hsia Tham, Elaine Phaik Ling Quah, Elizabeth Huiwen Tham, Evelyn Chung Ning Law, Evelyn Keet Wai Lau, Evelyn **u Ling Loo, Fabian Kok Peng Yap, Falk Müller-Riemenschneider, Franzolini Beatrice, George Seow Heong Yeo, Gerard Chung Siew Keong, Hannah Ee Juen Yong, Helen Yu Chen, Hong Pan, Huang Jian, Huang Pei, Hugo P S van Bever, Hui Min Tan, Iliana Magiati, Inez Bik Yun Wong, Ives Lim Yubin, Ivy Yee-Man Lau, Jacqueline Chin Siew Roong, Jadegoud Yaligar, Jerry Kok Yen Chan, Jia Xu, Johan Gunnar Eriksson, Jonathan Tze Liang Choo, Jonathan Y. Bernard, Jonathan Yinhao Huang, Joshua J. Gooley, Jun Shi Lai, Karen Mei Ling Tan, Keith M. Godfrey, Keri McCrickerd, Kok Hian Tan, Kothandaraman Narasimhan, Krishnamoorthy Naiduvaje, Kuan ** Lee, Li Chen, Lieng Hsi Ling, Lin Lin Su, Ling-Wei Chen, Lourdes Mary Daniel, Lynette Pei-Chi Shek, Maria De Iorio, Marielle V. Fortier, Mary Foong-Fong Chong, Mary Wlodek, Mei Chien Chua, Melvin Khee-Shing Leow, Michael J. Meaney, Michelle Zhi Ling Kee, Min Gong, Mya Thway Tint, Navin Michael, Neerja Karnani, Ngee Lek, Noor Hidayatul Aini Bte Suaini, Oon Hoe Teoh, Peter David Gluckman, Priti Mishra, Queenie Ling Jun Li, Sambasivam Sendhil Velan, Seang Mei Saw, See Ling Loy, Seng Bin Ang, Shang Chee Chong, Shiao-Yng Chan, Shirong Cai, Shu-E Soh, Stephen Chin-Ying Hsu, Suresh Anand Sadananthan, Swee Chye Quek, Tan Ai Peng, Varsha Gupta, Victor Samuel Rajadurai, Wee Meng Han, Wei Wei Pang, Yap Seng Chong, Yin Bun Cheung, Yiong Huak Chan, Yung Seng Lee, Zhang Han.
Funding
The study is supported by the National Research Foundation (NRF) under the Open Fund-Large Collaborative Grant (OF-LCG; MOH-000504) administered by the Singapore Ministry of Health’s National Medical Research Council (NMRC) and the Agency for Science, Technology and Research (A*STAR). In RIE2025, GUSTO is supported by funding from the NRF’s Human Health and Potential (HHP) Domain, under the Human Potential Programme. KMG is supported by the UK Medical Research Council (MC_UU_12011/4), the National Institute for Health Research (NIHR Senior Investigator (NF-SI-0515-10042) and NIHR Southampton Biomedical Research Centre (NIHR203319)) and the European Union (Erasmus + Programme ImpENSA 598488-EPP-1-2018-1-DE-EPPKA2-CBHE-JP).
The funders had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript. For the purpose of Open Access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Author information
Authors and Affiliations
Contributions
AC and MFFC designed the research;
YSC, KMG, LS, KHT, and JGE designed and led the GUSTO study;
JYT, PN, SC contributed to data collection and/or data processing;
AC performed the statistical analysis and drafted the manuscript;
All authors critically reviewed the manuscript; read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The GUSTO study was approved by the National Health Care Group Domain Specific Review Board (D/09/021 and B/2014/00406) and the SingHealth Centralized Institutional Review Board (2018/2767/D and 2009/291/D). All participants gave informed written consent upon recruitment.
Consent for publication
Not applicable.
Competing interests
KMG and YSC. are part of an academic consortium that has received research funding from Société Des Produits Nestlé S.A., Abbott Nutrition, Danone and BenevolentAI Bio Ltd, and are co-inventors on patents filed on nutritional factors and metabolic risk outside the submitted work. KMG has received reimbursement for speaking at a Nestle Nutrition Institute conference.
FMR and JYB are members of the Editorial Board of International Journal of Behavioral Nutrition and Physical Activity. They were not involved in the journal’s peer review process of, or decisions related to, this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chia, A., Toh, J.Y., Natarajan, P. et al. Trajectories of lifestyle patterns from 2 to 8 years of age and cardiometabolic risk in children: the GUSTO study. Int J Behav Nutr Phys Act 21, 9 (2024). https://doi.org/10.1186/s12966-024-01564-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-024-01564-z