
Abstract
Background
Blood loss in posterior surgery patients with thoracolumbar metastasis posed a significant challenge to surgeons. This study aimed to explore the risk factors of blood loss in posterior surgery for patients with thoracolumbar metastasis.
Methods
One hundred forty-two patients were retrospectively reviewed. Their baseline characteristics were recorded. The Gross equation was used to calculate blood loss on a surgical day. Multivariate linear regression was used to analyze the risk factors.
Results
Mean blood loss of 142 patients were 2055 ± 94 ml. Hypervascular primary tumor (kidney, thyroid and liver) (P = 0.017), wide or marginal excision (en-bloc: P = 0.001), metastasis at the lumbar spine (P = 0.033), and the presence of extraosseous tumor mass (P = 0.012) were independent risk factors of blood loss in the posterior surgery. Sub-analysis showed that wide or marginal excision (en-bloc: P < 0.001) and metastasis at lumbar spine (P = 0.007) were associated with blood loss for patients with non-hyper vascular primary tumors. Wide or marginal excision (piece-meal: P = 0.014) and the presence of an extraosseous tumor mass (P = 0.034) were associated with blood loss for patients with hypervascular primary tumors.
Conclusion
Hypervascular primary tumor (kidney, thyroid, and liver) was an independent risk factor of blood loss in the posterior surgery. The presence of extraosseous tumor mass and wide or marginal excision (piece-meal) were independent risk factors for patients with hypervascular primary tumors. Metastasis at the lumbar spine and wide or marginal excision (en-bloc) were independent risk factors for patients with non-hyper vascular primary tumors.
Similar content being viewed by others

Background
The spine is the most common site of bone metastasis. The spine is the most common site of bone metastasis. The number of patients with spinal metastasis has increased significantly due to a growing population and prolonged survival of cancer patients [1]. Intractable pain and neurological dysfunction caused by spinal metastasis seriously affect patients’ quality of life. Some studies apply a new technique to treat these patients, such as minimally invasive surgery [2]. However, posterior surgery is still the first choice for rapidly progressing spinal cord and nerve root compression [3, 4].
Blood loss is a significant problem for patients with spinal metastasis receiving posterior surgery. A meta-analysis showed that the mean intraoperative blood loss of patients with spinal metastasis was 2180 ml [5], and the amount of blood loss had been proven to be closely related to the occurrence of perioperative complications [6]. Blood loss during surgery could be divided into dominant and recessive. The dominant blood loss mainly comes from tumor wounds, expanded epidural venous plexus, and cancellous bone surface, while recessive blood loss is mainly related to interstitial oozing and hemolysis. Some previous studies had explored the risk factors of blood loss of posterior surgery for patients with spinal metastasis but only based on the amount of blood loss recorded during the surgery, ignoring the amount of recessive blood loss [7,8,9]. The concept of recessive blood loss was popular among spinal and joint degeneration diseases. The mean recessive blood loss for patients with spinal degeneration was accounted for about 50% of the total blood loss and seriously affects patients’ postoperative rapid recovery [10]. There was still a lack of study about the total blood loss (dominant and recessive) posterior surgery for patients with spinal metastasis.
This study conducted a retrospective analysis of patients with thoracolumbar metastasis treated in our department. The Gross equation [11] was used to calculate the total blood loss on a surgical day. This study aimed to help the surgeon identify total blood loss risk factors on a surgical day. It is of great significance to identify patients at high risk of more blood loss and take necessary countermeasures to ensure patients’ safety and rapid recovery and reduce perioperative complications.
Methods
Study design and selection criteria
Inclusion: This was a single-centered retrospective study of patients with thoracolumbar metastasis who underwent posterior surgery in our department from January 2011 to December 2017. A total of 170 patients were included as our initial cases.
Exclusion: We excluded those patients with hematological tumors (19 cases), missing imaging data (5 cases) or laboratory tests (1 case), and primary tumors of unknown sources (3 cases). At last, 142 patients were included in this study.
All patients underwent a physical examination. X-ray and Magnetic Resonance Imaging (MRI) were performed to confirm the lesion’s location. Their blood samples were taken before surgery for a routine test. Surgical indications were intractable pain due to spinal instability and myelopathy caused by spinal cord compression. The surgery option was determined by multidisciplinary cooperation, an experienced neuro-radiologist, a spinal tumor surgeon, and an oncologist. Our institute’s research ethics boards approved the study protocol and required neither patient approval nor informed consent to review patients’ images and medical records. Moreover, this study was conducted following the declaration of Helsinki. The flow of patient enrolment is shown in Fig. 1.

The flowchart of patient inclusion
The Gross equation calculated the total blood loss on a surgical day.
Gross equation: total perioperative blood loss = theoretical total blood loss + allogeneic blood transfusion (the patients in this study did not use autologous blood transfusion during and after surgery)
[12]
Data collection
Among the clinical variables, we reviewed the medical record to assess demographic information, BMI (non-overweight < 25; overweight: ≥25), tumor-related information, surgery-related information, and HGB before the operation. Tumor-related information included primary type. The Blood supply of primary cancer was divided into hypervascular (liver cancer, kidney cancer, thyroid cancer) or non-hyper vascular [13]. Surgery-related information included surgical methods (palliative surgery: piece-meal resection, wide or marginal excision: piece-meal or en-bloc resection), surgical site (upper thoracic spine: T1-T6, lower thoracic spine: T7-T12, lumbar spine: L1-L5), the number of surgery segments (single, multiple), the presence of extraosseous tumor mass, and preoperative embolism.
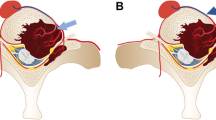
Surgical techniques and typical cases.
Experienced spinal surgeons under general anesthetic performed all operations. Surgery was performed via the median posterior approach, and paravertebral muscles were stripped to expose the lamina and facet joints. Pedicle screws were usually inserted into two levels of the upper and lower vertebra. Palliative surgery, wide or marginal excision, was performed. The intraoperative blood transfusion was considered when HGB dropped lower than 80.0 g/L. Typical cases are showed in Figs. 2 and 3.

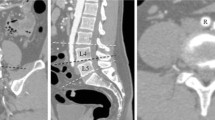
A 49-year-old woman with spine metastases of breast cancer. The patient underwent posterior marginal excision (en-bloc). The total blood loss was 4121 ml. A Preoperative sagittal thoracic vertebral MRI showed vertebral collapse at T6. Preoperative transversal MRI showed that the tumor involved the upper and lower adjacent vertebral bodies (T5 and T7); B Preoperative anteroposterior thoracic vertebral radiography; C Postoperative lateral anteroposterior thoracic vertebral radiography

A 57-year-old man with spine metastases of renal cell carcinoma. The patient underwent preoperative arterial embolism and posterior marginal excision (piece-meal). The total blood loss was 7429 ml. A Preoperative sagittal thoracic vertebral MRI showed vertebral collapse at T3. Preoperative transversal MRI showed an extraosseous tumor mass at T3; B Preoperative anteroposterior thoracic vertebral radiography; C Postoperative lateral anteroposterior thoracic vertebral radiography
Statistical analysis
Data results were analyzed with SPSS 25.0 statistical software (IBM Corporation, Armonk, NY.). Continuous variables were expressed as mean (standard deviation), and categorical variables were expressed as numbers. Differences were tested using one-way ANOVA between different groups. Multivariate analysis was performed by linear regression using a stepwise approach to identify independent predictors of blood loss in the posterior surgery. Partial correlation was used to analyze the related factors of blood transfusion. P < 0.05 was considered as statistically significant (two-sided test).
Results
Patient ‘s baseline characteristics and blood loss
The study included 142 patients with a mean age of 60.9 ± 0.9 years. There were 99 males and 43 females. The Mean blood loss of 142 patients was 2055 ± 94 ml. The mean blood loss of patients with primary tumors of different blood supply was divided as shown in Table 1. The patient’s baseline characteristics and feature-related mean blood loss are shown in Table 2. One-way ANOVA was used to detect the difference in mean blood loss between characteristics. Patients with hypervascular primary tumors (kidney, thyroid, and liver) had significantly more mean blood loss than other types of tumor (P = 0.004). Patients with extraosseous tumor mass (P = 0.035) and who underwent wide or marginal excision (P < 0.001) had significantly more mean blood loss than other patients.
Factors affecting blood loss on a surgical day
Univariate linear analysis showed that hypervascular primary tumor (P = 0.001, β = 683), wide or marginal excision (piece-meal: P = 0.001, β = 735; en-bloc: P < 0.001, β = 1775) and the presence of extraosseous tumor mass (P = 0.035, β = 446) were significantly associated with average blood loss. Further multivariate linear analysis showed that four factors were independent risk factors for blood loss in the posterior surgery. These factors included hypervascularprimary tumor (P = 0.017, β = 529), wide or marginal excision (en-bloc: P < 0.001, β = 2053), metastasis at lumbar spine (P = 0.033, β = 470), and the presence of extraosseous tumor mass (P = 0.012, β = 513) Table 3.
The sub-analysis showed that wide or marginal excision (en-bloc: P < 0.001, β = 2400) and metastasis at lumbar spine (P = 0.007, β = 619) were significantly associated with blood loss for patients with non-hypervascular primary tumor. For patients with hypervascular primary tumor, wide or marginal excision (piece-meal: P = 0.014, β = 1926) and the presence of extraosseous tumor mass (P = 0.034, β = 913) were significantly associated with blood loss in the posterior surgery Table 4.
Discussion
Patients with spinal metastasis have significant differences in individual blood loss during posterior surgery. The study of Kumar N et al. showed that the mean blood loss in posterior surgery for patients with metastasis was only 870 ± 720 ml [9], while most studies found that patients would suffer more blood loss during surgery. The Meta-analysis of Chen Y et al. showed that the mean intraoperative blood loss in posterior surgery for patients with metastasis was 2180 ml, and 12% of patients exceeded 5000 ml [5]. Gao X et al.’s study is roughly the same as Chen Y et al.’ study, with the mean blood loss of 1756 ± 1218 ml [8]. Although the amount of recessive blood loss during posterior surgery for patients with spinal metastasis was still uncertain, the amount of blood loss in the previous studies was based on the operation record, ignoring the amount of recessive blood loss and might underestimate the patient’s total blood loss.
We carried out this retrospective study, and the Gross equation was used to calculate the total blood loss on a surgical day. The results showed that the mean blood loss was 2055 ± 94 ml on the surgical day, similar to Chen Y et al. and Gao X et al.’s study. Hypervascular primary tumor (kidney, thyroid, and liver), wide or marginal excision, metastasis at the lumbar spine, and the presence of extraosseous tumor mass were significantly associated with blood loss. The results were partially consistent with previous studies except for the surgical method. Gao X et al.’s study showed that the risk factors for intraoperative blood loss in patients with spinal metastasis, including the primary tumor type, tumor location, exposed segment, decompression segment, and surgical method, in which En bloc resection had less intraoperative blood loss compared with piece-meal resection [8]. En bloc resection was one kind of wide or marginal excision, requiring extensive tissue separation. En bloc excision would reduce the intraoperative blood loss from tumor wounds independent of the primary tumor type. However, the extensive separation of normal tissue and longer surgery time would significantly increase the interstitial oozing (recessive blood loss). Patients who underwent palliative surgery were not the same as patients who underwent wide or marginal excision. Recessive blood loss consisted of a small part of total blood loss due to the more considerable amount of intraoperative blood loss. Based on our and previous study results, recessive blood loss had different effects in different surgical procedures. The surgeon should pay special attention to patients who underwent wide or marginal excision for massive recessive blood loss.
Patients with hypervascular primary tumors had significantly more blood loss than patients with other types in this study. Many studies confirmed preoperative embolization for patients with hypervascular primary tumors that could effectively reduce intraoperative blood loss [14, 15]. The present study did not find a correlation between preoperative embolization and blood loss. First, this might be related to the selection bias. Only 10 patients with renal cancer and 2 patients with liver cancer received preoperative embolization in our study. Second, the inclusion of recessive blood loss might weaken the effect of embolization on the control of bleeding. Preoperative embolization for spinal tumors had a risk of spinal ischemia [16]. Selective computed tomography angiography for detecting radiculomedullary arteries was an effective method to find radiculomedullary arteries and improve security [17].
Intraoperative blood loss for patients with spinal metastasis mainly comes from tumor wounds, especially those with hypervascular primary tumors. For these patients, the presence of extraosseous tumor mass significantly increased the intraoperative bleeding. It was necessary to remove all tumor tissue to control the bleeding from tumor wounds when patients underwent piece-meal resection. For patients with hypervascular primary tumors and who underwent piece-meal resection, proper strip** in normal tissues to minimize the blood supply of tumor masses could effectively reduce the intraoperative from tumor wounds. Treatment with bipolar electrocoagulation before piece-meal resection of tumor mass could also effectively reduce the intraoperative wound bleeding.
Tang X et al. reviewed 173 patients with sacral tumors. The results showed that tumor volume greater than 200 cm3 was a risk factor for more blood loss [18]. Tumor volume greater than 5 cm was considered a risk factor for excessive blood loss for bone tumors [19]. The volume of the lumbar spine is more significant than that of the upper thoracic spine [20], and the presence of extraosseous tumor mass also increases the tumor volume. Otherwise, the lumbar spine’s height is higher than that of the thoracic spine, so the surgical incision is longer than that of the thoracic spine, which increases the dissection range and interstitial space, and a result of more recessive blood loss in the interstitial space.
Recently, some surgeons have tried to apply minimally invasive spine surgery for patients with spinal metastasis. Minimally invasive spine surgery is performed through physiological tissue gaps. Less tissue strip** can effectively reduce intraoperative bleeding and postoperative interstitial oozing. Chou D et al. and Zhu X et al. showed that minimally invasive spine surgery could reduce intraoperative blood loss and postoperative drainage compared with conventional surgery [21, 22]. Even for patients who underwent en-bloc, minimally invasive spine surgery also had an advantage compared with conventional surgery [23]. Minimally invasive spine surgery might be a good choice characterized by less physiological insult and fewer postoperative complications, allowing early mobilization and rapid recovery.
There are limitations to the present study. First, it was limited by its retrospective nature, and there would be a particular bias in patient selection. Second, the period of this study was relatively long, and the learning curve of surgical skills was not included in the factors analyzed in this study. Last, for the relatively long-time span of the present study, the anesthesia protocol was not completely consistent during the study. This would have an impact on blood bleeding. However, this study provides important information regarding total blood loss risk factors in conventional surgery patients with thoracolumbar metastasis on a surgical day.
Conclusions
Hypervascular primary tumor (kidney, thyroid, and liver) was an independent risk factor of blood loss in the posterior surgery. The presence of extraosseous tumor mass and wide or marginal excision (piece-meal) were independent risk factors for patients with hypervascular primary tumor. Metastasis at the lumbar spine and wide or marginal excision (en-bloc) were independent risk factors for patients with non-hyper vascular primary tumors.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due privacy or ethical restrictions but are available from the corresponding author on reasonable request.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. https://doi.org/10.3322/caac.21551.
Hansen-Algenstaedt N, Kwan MK, Algenstaedt P, et al. Comparison Between Minimally Invasive Surgery and Conventional Conventional surgery for Patients With Spinal Metastasis: A Prospective Propensity Score-Matched Study. Spine (Phila Pa 1976). 2017;42(10):789–97. https://doi.org/10.1097/BRS.0000000000001893.
Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366(9486):643–8. https://doi.org/10.1016/S0140-6736(05)66954-1.
Jansson KÅ, Bauer HCF. Survival, complications and outcome in 282 patients operated for neurological deficit due to thoracic or lumbar spinal metastases. Eur Spine J. 2006;15(2):196–202. https://doi.org/10.1007/s00586-004-0870-6.
Chen Y, Tai BC, Nayak D, et al. Blood loss in spinal tumour surgery and surgery for metastatic spinal disease: a meta-analysis. Bone Joint J. 2013;95-B(5):683–8. https://doi.org/10.1302/0301-620X.95B5.31270.
Klineberg EO, Nguyen S, Kelly MP, et al. Estimated blood loss is a weak predictor of major complications in adult spinal deformity surgery. Spine J. 2016;16(10):S264. https://doi.org/10.3171/2019.3.SPINE181452.
René S, Gerhard RH, Florian D, et al. Surgical therapy of vertebral metastases. Are there predictive parameters for intraoperative excessive blood loss despite preoperative embolization? Tumori. 2011;97(1):66–73. https://doi.org/10.1177/030089161109700113.
Gao X, Fan T, He S, et al. A useful model for predicting intraoperative blood loss in metastatic spine tumor surgery. Clin Spine Surg. 2020;33(6):E256–62. https://doi.org/10.1097/BSD.0000000000000911.
Kumar N, Zaw AS, Khine HE, et al. Blood loss and transfusion requirements in metastatic spinal tumor surgery: evaluation of influencing factors. Ann Surg Oncol. 2016;23(6):2079–86. https://doi.org/10.1245/s10434-016-5092-8.
Smorgick Y, Baker KC, Bachison CC, et al. Hidden blood loss during posterior spine fusion surgery. Spine. 2013;13(8):877–87. https://doi.org/10.1016/j.spinee.2013.02.008.
Gross JB. Estimating allowable blood loss: corrected for dilution. Anesthesiology. 1983;58(3):277–80. https://doi.org/10.1097/00000542-198303000-00016.
Nadler SB, Hidalgo JU, Bloch T. Prediction of blood volume in normal human adults. Surgery. 1962;51(2):224–32.
Hong CG, Cho JH, Suh DC, et al. Preoperative embolization in patients with metastatic spinal cord compression: mandatory or optional? World J Surg Oncol. 2017;15(1):45. https://doi.org/10.1186/s12957-017-1118-3.
Kato S, Hozumi T, Takaki Y, et al. Optimal schedule of preoperative embolization for spinal metastasis surgery. Spine (Phila Pa 1976). 2013;38:1964–9. https://doi.org/10.1097/BRS.0b013e3182a46576.
Tan BWL, Zaw AS, Rajendran PC, et al. Preoperative embolization in spinal tumour surgery: enhancing its effectiveness. J Clin Neurosci. 2017;43:108–14. https://doi.org/10.1016/j.jocn.2017.05.021.
Houten JK, Swiggett SJ, Hadid B, et al. Neurologic complications of preoperative embolization of spinal metastasis: a systemic review of the literature identifying distinct mechanisms of injury. World Neurosurg. 2020;143:374–88. https://doi.org/10.1016/j.wneu.2020.08.006.
Chatani S, Haimoto S, Sato Y, et al. Preoperative Embolization of Spinal Metastatic Tumor: The Use of Selective Computed Tomography Angiography for the Detection of Radiculomedullary Arteries. Spine Surg Relat Res. 2021;5(4):284–91. https://doi.org/10.22603/ssrr.2020-0202.
Tang X, Guo W, Yang R, et al. Risk factors for blood loss during sacral tumor resection. Clin Orthop Relat Res. 2009;467:1599–604. https://doi.org/10.1007/s11999-008-0483-1.
Kawai A, Kadota H, Yamaguchi U, et al. Blood loss and transfusion associated with musculoskeletal tumor surgery. J Surg Oncol. 2005;92:52–8. https://doi.org/10.1002/jso.20375.
Limthongkul W, Karaikovic EE, Savage JW, Markovic A. Volumetric analysis of thoracic and lumbar vertebral bodies. Spine J. 2010;10(2):153–8. https://doi.org/10.1016/j.spinee.2009.11.018.
Chou D, Lu DC. Mini-open transpedicular corpectomies with expandable cage reconstruction. Technical note. J Neurosurg Spine. 2011;14(1):71–7. https://doi.org/10.3171/2010.10.SPINE091009.
Zhu X, Lu J, Xu H, et al. A comparative study between minimally invasive spine surgery and traditional open surgery for patients with spinal metastasis. Spine (Phila Pa 1976). 2021;46(1):62–8. https://doi.org/10.1097/BRS.0000000000003690.
Fang T, Dong J, Zhou X, et al. Comparison of mini-open anterior corpectomy and posterior total en bloc spondylectomy for solitary metastases of the thoracolumbar spine. J Neurosurg Spine. 2012;17(4):271–9. https://doi.org/10.3171/2012.7.SPINE111086.
Acknowledgements
Not applicable.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
Xd S conceived and designed the project. Yp C and Yx P collected and organized the data, analyzed and interpreted the data. Yp C and Xd S wrote the core of the manuscript. Hj L and Yf L coordinated the statistical analyses. C M and B W revised the manuscript. Xd S revised and approved the final version of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The local Ethics Committee of Peking University First Hospital approved this study (2017[1417]).
All participants in this study were above 16 years of age. The need for written informed consent was waived by the Peking University First Hospital ethics committee due to retrospective nature of the study.
Consent for publication
All authors read and approved the final manuscript. All authors agree to publish the article.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cui, Y., Shi, X., Mi, C. et al. Risk factors of total blood loss in the posterior surgery for patients with thoracolumbar metastasis. BMC Musculoskelet Disord 22, 898 (2021). https://doi.org/10.1186/s12891-021-04789-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-021-04789-2