
Abstract
Background
Interactive and experiential learning programs have proven effective to teach children safety and prevent child unintentional injury. However, previously-published programs were designed primarily to address safety concerns of children living in urban, well-resourced areas, and therefore might be less effective or economically infeasible to distribute to children in resource-limited areas, such as those living in rural areas or underdeveloped regions. This proposed study will evaluate the effectiveness of teaching children safety lessons to rural preschoolers in China through the preschool-based Safety Experience Room intervention that was developed based on relevant theories, the lessons of previous intervention research, the characteristics of child injuries in underdeveloped rural areas, and the needs and circumstances of rural families and preschools in China. The study will also evaluate the cost-effectiveness of delivering the program.
Methods and analysis
A single-blinded, 12-month follow-up, parallel-group cluster randomized controlled trial with a 1:1 allocation ratio will be implemented in two selected counties. In total, at least 2378 rural preschoolers aged 3–6 years old will be recruited from 12 preschools, 6 in Yang County and 6 in Shicheng County. Clusters will be randomized at the preschool level and allocated to the control group (routine school-based education) or the intervention group (routine school-based education plus the Safety Experience Room education). External support strategies will be implemented by local partners to minimize attrition. Data collection will be conducted at baseline and then every 3 months during a 12-month follow-up time period. Intention-to-treat (ITT) data analysis will be used. Generalized estimation equations (GEE) will evaluate the effectiveness of the program and generalized cost-effectiveness analysis (GCEA) will evaluate the cost-effectiveness of it. A per-protocol (PP) sensitivity analysis will assess the robustness of ITT results. Subgroup analyses will be performed to evaluate the impact of socio-demographic factors on the intervention effect, following the same strategies as the primary analyses.
Discussion
The newly-designed Safety Experience Room program is expected to be feasible, effective, and financially beneficial. If these hypotheses prove true, we will take steps to disseminate the program to rural preschools across China.
Trial registration
Chinese Clinical Trial Registry (http://www.chictr.org.cn), CHiCTR2000038025, registered on 8 September 2020.
Similar content being viewed by others


Background
Among the widely-disseminated child safety education topics are school-based lessons to children about how to interact in a safe way with their surroundings. Such efforts can improve children’s safety-related knowledge, skills, behaviors, and practices, and ultimately reduce the occurrence and severity of injury events [1,2,3]. Traditional school-based education programs where a teacher delivers safety information to children, however, show mixed effectiveness on reducing child injury. They are especially ineffective in transmitting knowledge, skills, and behavior change when lessons lack interactive aspects and are delivered in a monotonous and rote manner [3, 4].
Interactive education represents an educational approach that integrates traditional design, product design, and new media design to enrich the educational experience through communication and interchange among participants that facilitates learning and behavior change [5, 6]. Interactive education can stimulate the improvement of knowledge, attitudes, and behaviors [7] through immersive experiences and participatory learning in diverse forms, such as using miniatures [8], story-based toys or puzzles [9, 10], scenario-based storybooks [11], virtual reality [12], or interactive games [7, 13].
Several published studies report the effectiveness of interactive education interventions to improve children’s knowledge, behaviors, skills, and/or self-efficacy for safety promotion and injury prevention [8, 14,15,16]. For instance, young children exposed to interactive education programs were found to have improved knowledge, behaviors, skills, or self-efficacy for broad injury prevention [10], as well as specific safety domains like fire safety [17], dog bite prevention [18, 19], and street-crossing [24] or dog bites [18]), rather than the full array of risky situations and environments that children may face. Third, most previous studies examined changes in injury-related knowledge, attitudes, or simulated behaviors as study outcome measures rather than collecting data on actual injury incidents [25, 26]. This is partly the result of the short durations used to implement interventions with comparatively small sample sizes, making it infeasible to detect significant changes in injury incidence [18, 21,22,23, 27]. Last, a large portion of the existing studies conducted in low- and middle-income countries (LMICs) rely on pre-post or other non-experimental designs rather than more rigorous randomized controlled trials (RCTs).
To address these research limitations, we developed a standardized, affordable, replicable, and easy-to-implement interactive intervention, the “Safety Experience Room”, to train preschool-aged children in rural China on safety and injury prevention. The program is based on relevant educational theories, extends lessons learned from previous interactive learning intervention research, focuses especially on the characteristics of injuries in rural and resource-limited areas, and considers the specific contextual needs and circumstances of rural preschoolers and preschools in China. We propose a rigorous cluster randomized controlled trial that uses injury incidents as a study outcome to evaluate effectiveness and cost-effectiveness of the Safety Experience Room in preventing unintentional injury incidence among preschoolers living in rural China.
Methods and analysis
Study design
A single-blinded, 12-month follow-up, cluster randomized and controlled trial with a 1:1 allocation ratio will be implemented in Yang County, Shaanxi Province, and Shicheng County, Jiangxi Province, China. The trial was registered on September 8, 2020 in the Chinese Clinical Trial Registry (http://www.chictr.org.cn/showproj.aspx?proj=57719, registration number: ChiCTR2000038025).
Sample size
Based on a previous survey [28], we conservatively estimated that unintentional injury incidence among preschoolers aged 3–6 years old in the study sites over a 12-month period will be 30%. According to relevant reports [29], we estimated the effect size of the Safety Experience Room intervention will be 0.75 (incidence rate ratio) compared with a traditional educational intervention. An intra-class correlation (ICC) of 0.005 within a cluster size of 200 children per preschool was estimated [30, 31]. Nearly whole rural preschoolers stay enrolled in the same preschool throughout childhood, so we conservatively estimate a maximum attrition rate of 10% over the 12-month follow-up time period. Given these estimates, a minimum sample size of 2378 preschoolers is sufficient to achieve statistical power of 80% at the significance level of 0.05. Our preliminary surveys indicate most local rural preschools have 200 to 300 children, so 12 preschools will be adequate to recruit the needed sample size.
Preschool recruitment
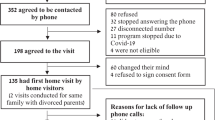
This study plans to recruit study participants from 12 preschools in China, 6 from Yang County in Shaanxi Province, and 6 from Shicheng County in Jiangxi Province (Figs. 1 and 2). Preschools that enroll more than 200 students and agree to participate in this study will be considered eligible preschools.

Flow diagram of selection of study participants

Timeline for participant enrollment, intervention implementation, and assessment
Each invited preschool will receive an official invitation letter along with relevant project materials. To avoid contamination between children within the same preschool, we will randomize the intervention and control programs at the school level. Consequently, 6 preschools will be randomly allocated to the intervention group, including 3 from Yang County and 3 from Shicheng County, while the other 6 preschools will be allocated to the control group, also including 3 from Yang County and 3 from Shicheng County.
Participant recruitment
All students attending participating preschools will be eligible to enroll in the study. Exclusion criteria include: (1) children who regularly attend preschools less than 3 full school days a week; (2) preschoolers who have mental or physical disabilities that prohibit valid participation in the learning activities of the Safety Experience Room; (3) preschoolers whose caregivers cannot cooperate with follow-up visits; and (4) preschoolers whose caregivers decline to sign informed consent.
In coordination with local governmental departments and agencies, we will recruit classroom teachers and school staff to help coordinate recruitment of study participants in each selected preschool. The teachers and staff members at each school will initially inform eligible preschoolers’ caregivers about the study via social media platforms (WeChat and QQ, the most popular applications in China), and then organize a caregiver-teacher meeting to communicate further about the study. Caregivers who agree to have their children participate in the study will be provided with an invitation letter that includes the benefits and responsibilities of participating in this study and be invited to read and sign an online informed consent.
Following consent processes, all participating caregivers will complete an online baseline survey to provide information on socio-demographic characteristics and details about unintentional injuries the children experienced in the prior 3 months, including the type and severity of each injury.
Randomization and masking
Once recruited, each enrolled preschool will be randomly allocated to a group by an independent (masked) researcher. Block randomization with a block size of 2 will be used to ensure balance between intervention and control groups. The allocation sequence will be generated by R version 4.0.4 software and the sequence will be sequentially numbered and opaque, stored in sealed envelopes until interventions are assigned. Group allocation will be concealed during data analysis.
Interventions
Both the intervention and control groups will receive routine school-based education on safety and injury prevention from their preschool. This education generally encompasses general health knowledge and skills, including injury prevention, and is performed by preschool teachers.
The intervention group will also receive the Safety Experience Room intervention. The Safety Experience Room involves creation of a space designed to teach safety and injury prevention. It can easily be renovated from typical Chinese preschool classrooms according to the standards in Table 1.
The Safety Experience Room will be flexibly divided into 3 zones, each with a specific function: a multi-media zone, a simulated scenario zone, and a spare zone (Fig. 3). The total cost of furnishing and decorating each Safety Experience Room will be controlled to a maximum cost of 13,200 CNY (approximately 1,970 USD), as detailed in Table 2.

Example interior design of the Safety Experience Room in a preschool
Consistent with stages of preschooler’s cognitive development [32, 33], we developed 3 sets of informative and entertaining instructional materials originally to teach children about each of the 6 safety themes. The lessons are designed to be engaging and easy-to-learn and are delivered through animation videos, interactive games with coherent game plots, and large-sized picture story books with corresponding story recordings. All teaching and learning materials were developed based on three overriding principles: (a) content to address risky scenarios that rural Chinese children commonly face in daily life and information to help preschoolers react safely in these situations; (b) content that teaches preschoolers to identify dangerous behaviors and recognize the potential for serious injurious consequences from the dangerous behaviors; and (c) a summarization of essential safety rules that children should obey and reminder to avoid dangerous behaviors at the end of each instructional material.
All content was developed properly with health behavior change theory in mind. In particular, the content had goals to alter peer norms by presenting safe behavior as normative; to instill in children a need to follow safety rules; to teach children about the risk and potential severity of injury at a developmentally-appropriate level; and to create some developmentally-appropriate levels of fear of injury in children. Some content is delivered using animals as characters to improve race, ethnicity, cultural, and gender identification among the children viewing it. The content will be delivered concretely through following primary mechanisms:
-
(1)
animation videos (Fig. 4A), which disseminate unintentional injury prevention knowledge that children should have in daily life through the activities of lively and entertaining cartoon characters;
-
(2)
interactive games (Fig. 4B), which are delivered by the multimedia touchscreen computer in the Safety Experience Room to offer children choice-points that involve safe or risky decisions and illustrate the health outcomes of distinct decisions. As children progress through the discrepant game plots, they become familiar with the consequences of potentially injurious decisions, both through the game plots and through reinforcing instructions from their teachers;
-
(3)
large-sized picture books and story recordings (Fig. 4C), which convey unintentional injury prevention knowledge and information through animal cartoon characters and voice-over story recordings.

Instructional materials of the Safety Experience Room intervention (A. animation videos; B. interactive games; C. large-picture story books)
For the two teaching themes of road traffic injury and drowning, we will utilize teaching props that simulate traffic and natural water environments in the simulated scenario zone. These lessons will convey relevant safety behaviors to children through learning tasks guided by their instructors.
To summarize, the Safety Experience Room offers five important educational aspects to impart safety under the guidance of the instructor (Table 1):
-
(1)
watching animation videos on a multimedia computer with touchscreen;
-
(2)
playing interactive games with coherent game plots using the large touchscreen multimedia computer;
-
(3)
experiencing scenarios in simulated traffic and natural water environments;
-
(4)
reading large-sized picture story books and listening to relevant story recordings related to the learning themes;
-
(5)
hearing summaries of the key safety behaviors from the teachers at the end of each course.
Instruction will be conducted over a six-week period, with one theme conveyed each week. To enhance learning among this young group of children, we will expose the children to a similar set of lessons a second time, over the next six weeks. Repetition of lessons should enhance learning and memory, which we expect to translate to safer behaviors outside the classroom [20].
If the Safety Experience Room intervention proves feasible and effective as hypothesized, we will deliver the intervention to children in the control group after completing the entire intervention, and then disseminate it broadly to other rural preschoolers across China.
Intervention implementation
An operation manual was developed to ensure standardized implementation of the Safety Experience Room intervention. The manual consists of eleven chapters which together introduce the design, facilities, and class schedule for the Safety Experience Room intervention; elaborate the lessons that teachers deliver; specify strategies to evaluate the intervention’s effectiveness using the evaluation version of the interactive games; and inform the management and maintenance staff at the facilities about the teaching materials in the Safety Experience Room.
Along with distributing the operation manual, we will organize a standardized training session for all instructors involved in the intervention group to improve compliance with the operation manual and ensure all instructors implement the Safety Experience Room education and evaluation program in a standard way.
Feasibility testing
Before the formal study begins, preschool teachers involved in the intervention group will undertake feasibility testing. The teachers will conduct pilot teaching sessions with all lessons in one class to familiarize themselves with the Safety Experience Room intervention and master the lesson delivery. Qualitative data will be collected from teachers and used to refine the teaching materials and teaching practices.
Fidelity of data collection
With the support from local partners including the local education bureau, the local office of the charitable foundation “World Vision,” and the preschools participating in this study, a coordinating group will be established for each enrolled preschool to assist the preschool teachers and staff in consistent delivery of the Safety Experience Room intervention in a manner consistent with the operation manual and to collect the survey data from preschoolers and their caregivers.
Outcome measures
Primary outcome measure
The primary outcome measure will be the unintentional injury incidence rate among preschoolers over the 12-month study period, which will be calculated by combining data from the four follow-up evaluations. Follow-up evaluations will be conducted quarterly to minimize caregiver’s recall bias for minor or moderate injuries experienced by the child [34].
We define an injury event as an incident meeting any of three criteria: (1) child receives a medical diagnosis or treatment by a doctor or other medical professional following an injury; (2) child receives first aid, takes any injury-related medication, or receives massage or cold/hot compress by a family member, preschool teacher, preschool staff member, or other individuals following an injury; or (3) child is restricted from school or other activities, or is forced to stay in bed or rest for more than a half-day following an injury. If a caregiver reports that a child experienced more than one unintentional injury event in the prior 3 months, we will record the number of injury events and then collect specific information regarding the most severe one.
The unintentional injury incidence rate will be calculated as the “number of preschoolers who experience new unintentional injury events over the past year divided by the total number of preschoolers×100%”.
Secondary outcome measures
We will collect data concerning several secondary outcome measures, as detailed below.
-
(1)
Preschooler’s unintentional injury prevention knowledge for road traffic injury, falls, and drowning. This knowledge will be evaluated based on the learning content of the 6 educational themes children are exposed to in the Safety Experience Room. Table 3 lists 18 key items we will use to measure children’s unintentional injury prevention knowledge.
-
(2)
Cost-effectiveness analysis (CEA). The calculation of CEA will follow the World Health Organization CHOosing Interventions that are Cost-Effective (WHO-CHOICE) approach to estimate population level effects of the interventions using a form of generalized cost-effectiveness analysis (GCEA) [35, 36].
For this study, the health effect of the Safety Experience Room intervention is the difference in the number of preschoolers experiencing unintentional injury events over the 12-month intervention period between the intervention and control groups. The costing of the intervention will include subsidies to the instructors paid from the project and costs for designing, furnishing and decorating each Safety Experience Room. The cost effectiveness ratio will be calculated as the total implementation costs of the intervention group divided by the health effect. Monte Carlo simulation (1000 runs using a truncated normal distribution) will be used to calculate a 95% uncertainty interval of the cost and outcome data.
Formal data collection
Survey data regarding the primary outcome for both groups, injury incidents, will be collected at baseline and every 3 months throughout the 12-month follow-up time period. In coordination with the local education bureau, the preschools will organize a caregiver-teacher meeting every 3 months. The class teacher will send the online survey link and ask all caregivers to complete the survey at the caregiver-teacher meeting. All primary outcome data will be collected through online survey. If caregivers fail to complete the online questionnaire, the classroom teacher will contact them to collect the survey data.
Collection of secondary outcome data will be carried out at baseline for both groups and after the intervention group completes each safety-related theme course designed for the intervention group. Secondary outcome data will be collected simultaneously from the control group to maintain comparison between two groups, but we will not disseminate any correct answers or teachings to the children in the control group before the study ends to avoid contamination in that group. All secondary outcomes data will be collected via preschoolers playing an evaluation version of the interactive games that has different story plots from the teaching version and permits retention of evaluation results. The evaluation version of the interactive games will not include any modules that disseminate injury prevention information or display evaluation results to children. Administration of the assessment will occur in a quiet environment. Each child will complete the tasks individually in the Safety Experience Room, with other classmates staying in the classroom respectively during the evaluation.
In order to assess children in the control group, relevant hardware and software (the multimedia touchscreen computer with the evaluation version of interactive games installed) will be delivered to control preschools accordingly. Staff members and teachers will help children start and reset the interactive games as well as maintain a quiet evaluation environment during the evaluation process.
Before formal data collection, teachers involved in both groups will learn to operate the evaluation games. Teachers will enter each child’s ID number and supervise individualized data collection but will not communicate with children or see children’s evaluation results. All data will be stored in the game backend database.
Data analysis plan
Primary data analysis will employ an intention-to-treat (ITT) approach. Descriptive statistics will be calculated for socio-demographic variables and primary and secondary outcomes, including mean (or median) and standard deviation (or range and interquartile range) for continuous variables, and frequency and proportion for categorical variables. At each time point, Chi-square test and two-sample t-test (or Wilcoxon rank sum test if data are skewed) will be used to examine the differences in outcome measures between intervention and control groups for categorical and continuous variables, respectively. Trend tests or analysis of variance (ANOVA) will be used to detect within-group differences across the four follow-up visits.
We will also use Generalized Estimating Equation (GEE) and Generalized Linear Mixed Models (GLMM) to evaluate the overall effectiveness of the intervention after adjusting for socio-demographic variables, engagement, and baseline injury events. Both binary outcomes (whether experienced unintentional injury during the study period) and quantitative count outcomes (number of unintentional injury events and injury prevention knowledge score) at the individual level will be analyzed using these models. Zero-inflation models will be used when needed.
Missing values will be imputed using either the Expectation Maximization (EM) algorithm or Markov Chain Monte Carlo, as appropriate for the data. A per-protocol (PP) sensitivity analysis will be conducted to validate ITT results. All statistical analyses will be performed using the up-to-date version of R. All statistical tests will be two-sided, with the level of 0.05 considered statistically significant.
Subgroup analyses will be performed to assess the impact of socio-demographic factors on the intervention effectiveness, including sex and age of children, grade level of preschoolers, education level of preschooler caregivers, and household income per capita in the prior 12 months. Subgroup analyses will follow the same statistical strategies for primary analyses.
This study will be rigorously conducted, analyzed, and reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 statement [37] and the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement [38].
Discussion
Interactive education has become increasingly popular worldwide given widespread availability of intelligent and multi-media devices at reasonable cost, plus the capacity to ground interactive interventions in educational and developmental theory and their proven efficacy [7, 39]. However, high-quality research evidence targeting child injury outcomes remains absent for interactive education interventions designed to prevent child unintentional injury in resource-limited areas like rural China.
We developed a standardized interactive education intervention that is easily replicated and generalized, the Safety Experience Room, and designed a 12-month RCT to assess the program’s effectiveness and cost-effectiveness in reducing child unintentional injury incidence rate in rural China. The intervention design relies on relevant theories, the lessons of previous intervention research, the characteristics of injuries in rural settings, and the cultural context of rural preschoolers and preschools in China.
This study will adhere strictly to recommended guidelines for design and implementation of randomized controlled trials [37, 38]. High-quality evidence will be generated to determine the effectiveness and cost-effectiveness of the Safety Experience Room intervention, and expand existing evidence on the effectiveness of interactive education interventions to prevent child unintentional injury in resource-limited areas.
If the Safety Experience Room education intervention proves effective as well as economically and technically feasible as we hypothesize, we will move to disseminate the standard, affordable, and easy-to-implement program broadly in rural China [7, 8, 40].
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Abbreviations
- ANOVA:
-
Analysis of variance
- CEA:
-
Cost-effectiveness analysis
- CONSORT:
-
Consolidated standards of reporting trials
- EM:
-
Expectation maximization
- GCEA:
-
Generalized cost-effectiveness analysis
- GEE:
-
Generalized estimation equations
- GLMM:
-
Generalized linear mixed model
- ICC:
-
Intra-class correlation
- ITT:
-
Intention-to-treat
- LMICs:
-
Low- and middle-income countries
- PP:
-
Per-protocol
- RCT:
-
Randomized controlled trial
- SPIRIT:
-
Standard protocol items, recommendations for interventional trials
- WHO-CHOICE:
-
World Health Organization choosing interventions that are cost-effective
References
Orton E, Whitehead J, Mhizha-Murira J, Clarkson M, Watson MC, Mulvaney CA, et al. School-based education programmes for the prevention of unintentional injuries in children and young people. Cochrane Database Syst Rev. 2016;12:CD010246. https://doi.org/10.1002/14651858.CD010246.pub2.
Duperrex O, Blackhall K, Burri M, Jeannot E. Education of children and adolescents for the prevention of dog bite injuries. Cochrane Database Syst Rev. 2009;2:CD004726. https://doi.org/10.1002/14651858.CD004726.pub2.
Ji Y, Ye Y, Lu Y, Li L, Yang G. An intervention to reduce bicycle injuries among middle school students in rural China. Int J Environ Res Public Health. 2017;14(7):690. https://doi.org/10.3390/ijerph14070690.
Duperrex O, Roberts I, Bunn F. Safety education of pedestrians for injury prevention. Cochrane Database Syst Rev. 2002;2:CD001531. https://doi.org/10.1002/14651858.cd001531.
Huang C. Designing high-quality interactive multimedia learning modules. Comput Med Imaging Graph. 2005;29(2):223–33. https://doi.org/10.1016/j.compmedimag.2004.09.017.
Li S. Zhenyu Gu. The 12th five-year plan textbook of industrial design in general higher education - interactive design. Bei**g: China water & power press; 2012.
Read JL, Shortell SM. Interactive games to promote behavior change in prevention and treatment. JAMA. 2011;305(16):1704–5. https://doi.org/10.1001/jama.2011.408.
McLaughlin CM, Barry WE, Barin EN, Mert M, Lowery C, Upperman JS, et al. Interactive education is associated with lower incidence of pedestrian-related injury in children. J Surg Res. 2019;244:57–62. https://doi.org/10.1016/j.jss.2019.06.015.
Xu X. Case analysis of interactive children’s paper toy based on story experience. Design. 2019;32(7):72–3.
Puspitasari I, Mulyono S, Kusumawati DN. The effect of interactive education with 3-Dimensional puzzles on the injury-prevention behaviours of school-age children. Compr Child Adolesc Nurs. 2019;42(sup1):173–8. https://doi.org/10.1080/24694193.2019.1578438.
De Droog SM, van Nee R, Govers M, Buijzen M. Promoting toddlers’ vegetable consumption through interactive reading and puppetry. Appetite. 2017;116:75–81. https://doi.org/10.1016/j.appet.2017.04.022.
Johnson NN, Carey J, Edelman BJ, Doud A, Grande A, Lakshminarayan K, et al. Combined rTMS and virtual reality brain-computer interface training for motor recovery after stroke. J Neural Eng. 2018;15(1):016009. https://doi.org/10.1088/1741-2552/aa8ce3.
Shin J-H, Ryu H, Jang SH. A task-specific interactive game-based virtual reality rehabilitation system for patients with stroke: a usability test and two clinical experiments. J Neuroeng Rehabil. 2014;11:32. https://doi.org/10.1186/1743-0003-11-32.
Schwebel DC, McClure LA, Severson J. Usability and feasibility of an internet-based virtual pedestrian environment to teach children to cross streets safely. Virtual Real. 2014;18(1):5–11. https://doi.org/10.1007/s10055-013-0238-5.
Schwebel DC, Gaines J, Severson J. Validation of virtual reality as a tool to understand and prevent child pedestrian injury. Accid Anal Prev. 2008;40(4):1394–400. https://doi.org/10.1016/j.aap.2008.03.005.
Kamel FAH, Basha MA. Effects of virtual reality and task-oriented training on hand function and activity performance in pediatric hand burns: a randomized controlled trial. Arch Phys Med Rehabil. 2021;102(6):1059–66. https://doi.org/10.1016/j.apmr.2021.01.087.
Morrongiello BA, Schwebel DC, Bell M, Stewart J, Davis AL. An evaluation of the great escape: can an interactive computer game improve young children’s fire safety knowledge and behaviors? Health Psychol. 2012;31(4):496–502. https://doi.org/10.1037/a0027779.
Schwebel DC, Li P, McClure LA, Severson J. Evaluating a website to teach children safety with dogs: a randomized controlled trial. Int J Environ Res Public Health. 2016;13(12):1198. https://doi.org/10.3390/ijerph13121198.
Schwebel DC, Morrongiello BA, Davis AL, Stewart J, Bell M. The Blue Dog: evaluation of an interactive software program to teach young children how to interact safely with dogs. J Pediatr Psychol. 2012;37(3):272–81. https://doi.org/10.1093/jpepsy/jsr102.
Schwebel DC, Wu Y, Li P, Severson J, He Y, **ang H, et al. Featured article: evaluating smartphone-based virtual reality to improve chinese schoolchildren’s pedestrian safety: a nonrandomized trial. J Pediatr Psychol. 2018;43(5):473–84. https://doi.org/10.1093/jpepsy/jsx147.
Schwebel DC, McClure LA. Using virtual reality to train children in safe street-crossing skills. Inj Prev. 2010;16(1):e1–e5. https://doi.org/10.1136/ip.2009.025288.
Arbogast H, Burke RV, Muller V, Ruiz P, Knudson MM, Upperman JS. Randomized controlled trial to evaluate the effectiveness of a video game as a child pedestrian educational tool. J Trauma Acute Care Surg. 2014;76(5):1317–21. https://doi.org/10.1097/TA.0000000000000217.
Ahmad H, Naeem R, Feroze A, Zia N, Shakoor A, Khan UR, et al. Teaching children road safety through storybooks: an approach to child health literacy in Pakistan. BMC Pediatr. 2018;18(1):31. https://doi.org/10.1186/s12887-018-0982-5.
Swartz L, Glang A, Schwebel DC, GeigerWolfe EG, Gau J, Schroeder S. Kee** baby safe: a randomized trial of a parent training program for infant and toddler motor vehicle injury prevention. Accid Anal Prev. 2013;60:35–41. https://doi.org/10.1016/j.aap.2013.07.026.
Lehtonen E, Sahlberg H, Rovamo E, Summala H. Learning game for training child bicyclists’ situation awareness. Accid Anal Prev. 2017;105:72–83. https://doi.org/10.1016/j.aap.2016.07.036.
Wong RS, Tung KT, Wong HT, Ho FK, Wong HS, Fu K, et al. A mobile game (Safe City) designed to promote children’s safety knowledge and behaviors: protocol for a randomized controlled trial. JMIR Res Protoc. 2020;9(6):e17756. https://doi.org/10.2196/17756.
Schwebel DC, Combs T, Rodriguez D, Severson J, Sisiopiku V. Community-based pedestrian safety training in virtual reality: a pragmatic trial. Accid Anal Prev. 2016;86:9–15. https://doi.org/10.1016/j.aap.2015.10.002.
Hu Y, Yu X, Liao Z. Incidence rate of unintentional-injury among leftover children in rural China: a meta-analysis. Mod Prev Med. 2015;42(23):4240–3.
Li L. Research of an experienced learning intervention on unintentional injury in school-aged children. Chin J Clin Psychol. 2018;26(4):826–30. https://doi.org/10.16128/j.cnki.1005-3611.2018.04.043.
Coupland C, DiGuiseppi C. The design and use of cluster randomised controlled trials in evaluating injury prevention interventions: part 2. Design effect, sample size calculations and methods for analysis. Inj Prev. 2010;16(2):132–6. https://doi.org/10.1136/ip.2009.023127.
Ning P, Cheng P, Schwebel DC, Yang Y, Yu R, Deng J, et al. An app-based intervention for caregivers to prevent unintentional injury among preschoolers: cluster randomized controlled trial. JMIR Mhealth Uhealth. 2019;7(8):e13519. https://doi.org/10.2196/13519.
Flavell JH. Cognitive development: children’s knowledge about the mind. Annu Rev Psychol. 1999;50:21–45. https://doi.org/10.1146/annurev.psych.50.1.21.
Vaskivska HO, Palamar SP, Kondratiuk SG, Zhelanova VV. Psychodidactic determinants of the development of children of preschool age. Wiad Lek. 2018;71(6):1207–14.
Warner M, Schenker N, Heinen MA, Fingerhut LA. The effects of recall on reporting injury and poisoning episodes in the National Health interview survey. Inj Prev. 2005;11(5):282–7. https://doi.org/10.1136/ip.2004.006965.
Bertram MY, Lauer JA, Stenberg K, Edejer TTT. Methods for the economic evaluation of health care interventions for priority setting in the health system: an update from WHO CHOICE. Int J Health Policy Manag. 2021;10(11):673–7. https://doi.org/10.34172/ijhpm.2020.244.
Ralaidovy AH, Bachani AM, Lauer JA, Lai T, Chisholm D. Cost-effectiveness of strategies to prevent road traffic injuries in eastern sub-saharan Africa and Southeast Asia: new results from WHO-CHOICE. Cost Eff Resour Alloc. 2018;16:59. https://doi.org/10.1186/s12962-018-0161-4.
Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. https://doi.org/10.1136/bmj.e7586.
Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomized trials. BMJ. 2010;340:c869. https://doi.org/10.1136/bmj.c869.
Theofanopoulou N, Isbister K, Edbrooke-Childs J, Slovák P. A smart toy intervention to promote emotion regulation in middle childhood: feasibility study. J Med Internet Res. 2019;6(8):e14029. https://doi.org/10.2196/14029.
Wehner DE, Sutton L. An interactive, hospital-based injury prevention program for first-, second-, and third-grade students. J Emerg Nurs. 2005;31(4):383–6. https://doi.org/10.1016/j.jen.2005.06.001.
Acknowledgements
The authors acknowledge the financial support from World Vision and the support of the local government departments for coordinating the participating schools.
Funding
The study was funded by the charitable non-governmental organization (NGO) “World Vision”. The study protocol underwent peer-review by the funding body. The funder had no role in the design of study, the collection, analysis, and interpretation of data, as well as in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
GH conceptualized this study, obtained funding, and will supervise the implementation and coordination of this intervention. JH and WW designed the intervention and are develo** the scripts for the instructional materials. JH and WW drafted the initial manuscript. PN, DCS, YY, PC, JL, NZ, WL, MZ, and HL reviewed the manuscript. YY edited the statistical methods and models. GH revised and finalized the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was obtained from the Ethics Committee of **angya School of Public Health, Central South University (No. XYGW-2020-58). This trial was registered on September 8, 2020 in the Chinese Clinical Trial Registry (http://www.chictr.org.cn/showproj.aspx?proj=57719, registration number: ChiCTR2000038025). All study participants will be preschoolers whose caregivers provide informed consent before participating in the study. Consent to participate in this study was obtained from local governmental departments and agencies, as well as the directors of the preschools at the study sites. All data will be collected and analyzed anonymously. This study will be rigorously conducted, analyzed, and reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 statement and the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement. Research protocols were designed under the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
He, J., Wang, W., Ning, P. et al. Evaluating the effectiveness of the safety experience room, an affordable interactive education intervention to prevent unintentional injury among rural preschoolers in China: protocol for a cluster randomized controlled trial. BMC Public Health 23, 531 (2023). https://doi.org/10.1186/s12889-023-15432-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15432-1