
Abstract
Novel coronavirus pneumonia (NCP) has been widely spread in China and several other countries. Early finding of this pneumonia from huge numbers of suspects gives clinicians a big challenge. The aim of the study was to develop a rapid screening model for early predicting NCP in a Zhejiang population, as well as its utility in other areas. A total of 880 participants who were initially suspected of NCP from January 17 to February 19 were included. Potential predictors were selected via stepwise logistic regression analysis. The model was established based on epidemiological features, clinical manifestations, white blood cell count, and pulmonary imaging changes, with the area under receiver operating characteristic (AUROC) curve of 0.920. At a cut-off value of 1.0, the model could determine NCP with a sensitivity of 85% and a specificity of 82.3%. We further developed a simplified model by combining the geographical regions and rounding the coefficients, with the AUROC of 0.909, as well as a model without epidemiological factors with the AUROC of 0.859. The study demonstrated that the screening model was a helpful and cost-effective tool for early predicting NCP and had great clinical significance given the high activity of NCP.
Similar content being viewed by others

Introduction
Since December 2019, novel coronavirus pneumonia (NCP) emerged in Wuhan, Hubei, which was well known as the largest transportation hub in China. The pathogen has been proved to be a novel betacoronavirus that is currently named 2019 novel coronavirus (2019-nCoV)1. The disease has swept across China rapidly through human-to-human transmission2,3,4. Since February 27, 2020, more than 78,000 people were confirmed to be infected and more than 2700 were died in China5.
As the number of patients soaring, scholars have summarized the clinical characteristics of NCP6,7,8. Symptoms at onset of disease included fever, cough, headache, vomiting, diarrhea and so on. Normal or decreased leukocyte count was common. Radiologic abnormalities like ground-glass opacity and patchy shadowing on chest X-ray or computed tomography (CT) were marked characteristics. Acute respiratory distress syndrome, arrhythmia and shock could also occur in severe cases. Until now, to detect 2019-nCoV by the accurate real-time reverse transcription polymerase chain amplification (RT-PCR) assessment has been regarded as the golden diagnostic standard9.
Nevertheless, false negative results in initial RT-PCR examination existed in a number of casesFull size table
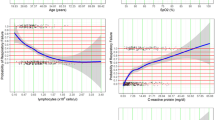
Model score without epidemiological history (model 3) = 0.6 (if having coexisting diseases) + 0.8 (if having fatigue) + 1.2 (if having dyspnea) + 2.4 (if feeling muscle soreness) − 0.3 * WBC count − 0.3 * Lymphocyte count + 1.6 * pulmonary imaging score. The AUROC was 0.859 (95% CI 0.833–0.884) (Fig. 2), with the optimal cutoff value of − 1, a sensitivity of 83.5% (95% CI 79.1–87.1%), a specificity of 76.0% (95% CI 72.1–79.4%), a diagnostic accuracy of 78.9% (95% CI 76.2–81.7%), and a Youden index of 0.595. Repeated fivefold Cross-Validation showed the average AUROC was 0.854, with the standard deviation of 0.027. The Hosmer–Lemeshow χ2 was 12.218 (P = 0.142), indicating no statistical difference from a perfect fit.
