
Abstract
Genetically modified mice models suggest an important role for G-protein-coupled receptor kinase 5 (GRK5) in the pathophysiology of obesity and related disorders. We investigated whether single nucleotide polymorphisms (SNPs) in the gene encoding GRK5 affect cardiometabolic traits in humans. We genotyped 3 common SNPs in intron 1 (rs1980030, rs10466210, rs9325562) and one SNP in intron 3 (rs10886471) of GRK5 in 2332 subjects at risk for type 2 diabetes. Total- and visceral fat mass were measured by magnetic resonance (MR) tomography and liver fat content by 1H-MR spectroscopy. Insulin secretion and sensitivity were estimated during an OGTT and measured during the euglycemic, hyperinsulinemic clamp (n = 498). Carriers of the minor allele of rs10466210 and rs1980030 had higher total- and LDL-cholesterol levels (p = 0.0018 and p = 0.0031, respectively, for rs10466210; p = 0.0035 and p = 0.0081, respectively, for rs1980030), independently of gender, age, BMI and lipid-lowering drugs. The effects of rs10466210 withstood Bonferroni correction. Similar associations were observed with apolipoprotein B levels (p = 0.0034 and p = 0.0122, respectively). Carriers of the minor allele of rs10466210 additionally displayed a trend for higher intima-media thickness of the carotid artery (p = 0.075). GRK5 may represent a novel target for strategies aiming at lowering LDL-cholesterol levels and at modifying cardiovascular risk.
Similar content being viewed by others


Introduction
The family of G-protein-coupled receptor kinases (GRKs) consists of seven serine/threonine kinases, which modulate several important intracellular signaling pathways. The main physiological action of GRKs is believed to be phosphorylation and thereby ‘desensitization’ (turn off) of G-protein-coupled receptors (GPCRs). GPCRs constitute the largest group of seven-transmembrane domain receptors, with more than 800 members, including the adrenergic, as well as several other hormone and cytokine receptors1,2. Phosphorylation of the activated GPCR leads to binding of β-arrestins, endocytosis of the receptor and ultimately to either receptor degradation or recycling and resensitization3. Other, kinase-independent, functions of GRKs have also been reported, including a role in inflammation (possibly by interacting with IκBα and inhibiting NFkB) and in regulating apoptosis4,5,6,7.
GRK5 was found to be most highly expressed in the heart and muscle as well as in the adipose tissue, but it is generally considered to be ubiquitously expressed in mammalian tissues1. High expression of GRK5 has been reported in several pathologies including cardiac hypertrophy and heart failure, hypertension, cancer, obesity and diabetes1,8,9,10,11,http://www.internationalgenome.org/1000-genomes-browsers). There are no other promoter regions in the gene, neither upstream nor downstream of the promoter. There are several putative promoter flanking sequences downstream of the GRK5 gene promoter, which have probably no significant relation to the core promoter (Supplemental Figs 1 and 2).
Based on publicly available phase II data of the International HapMap Project derived from Utah residents with Central European ancestry (release #24 November 2008, http://hapmap.ncbi.nlm.nih.gov/index.html.en), we identified 5 common SNPs (minor allele frequencies ≥0.05) in this intronic gene region, i.e., rs4752263, rs1980030, rs10466210, rs9325562, and rs10787932. Since rs4752263 and rs1980030, and also rs9325562 and rs10787932 were in linkage disequilibrium (r2 = 0.97 and r2 = 1, respectively) according to HapMap data, only the SNPs rs1980030, rs10466210 and rs9325562 were genotyped and further analysed. The HapMap linkage disequilibrium (r2) data of these five common SNPs are schematically shown in Fig. 1. Additionally, we genotyped rs10886471 in intron 3 of the GRK5 gene, because it was found in a genome-wide association study to be significantly associated with type 2 diabetes in Chinese Hans11. We could not find any data regarding LD among rs10886471 and the other SNPs in Europeans.

Genomic region of human chromosome 10 harboring the GRK5 gene. The HapMap linkage disequilibrium (r2) data of the 5 common (MAF ≥ 0.05) SNPs in intron 1 are shown. Since rs4752263 and rs190030, as well as rs10787932 and rs9325562, were in almost complete linkage disequilibrium, only the second member of the each pair was genotyped (framed). In addition the position of another common SNP (rs10886471) in intron 3 of the gene is depicted.
For genoty**, DNA was isolated from whole blood using a commercial DNA isolation kit (NucleoSpin, Macherey & Nagel, Düren, Germany). The 4 SNPs were genotyped using the Sequenom mass ARRAY system with iPLEX software (Sequenom, Hamburg, Germany). The genoty** success rates were 99.7%. The Sequenom results were validated by bidirectional sequencing in 50 randomly selected subjects, and both methods gave 100% identical results.
Statistical analyses
Since most of the variables were non-normally distributed, data are given as counts or medians [interquartile range]. For statistical analysis, data that were not normally distributed (Shapiro-Wilk W test) were logarithmically transformed. The univariate interrelationships (Pearson correlations) between the phenotypes tested are given in supplemental Table 1. To identify independent associations of the SNPs, we performed multiple linear regression analyses with the relevant metabolic traits set as dependent variables. BMI, waist circumference, TAT mass, VAT mass and liver fat content were adjusted for age and gender. The other traits were additionally adjusted for BMI. Lipid measurements (FFA, triglycerides, total-, HDL- and LDL-cholesterol levels, and apolipoproteins) were also adjusted for treatment with lipid-lowering medication and insulin secretion measurements also for insulin sensitivity (as estimated from the OGTT). The genotype was included in the analyses as an independent variable. For each dependent variable two models were applied. In the additive inheritance model, the effects of all genotypes on the dependent variable were compared and allele-dose effects were tested; in the dominant model, homozygotes for the major allele were compared to heterozygotes and homozygotes for the minor allele combined. The Hardy-Weinberg equilibrium was tested using a χ2-test (1 degree of freedom). The statistical software package JMP 11.0 (SAS Institute Inc, Cary, NC, USA) was used. We performed Bonferroni correction for the 4 SNPs tested and the following 4 physiologically unrelated traits: BMI (as being closely associated with body weight, waist circumference, total body, visceral and liver fat), insulin sensitivity and insulin secretion (as being strongly related to glucose, C-peptide and insulin levels, as well as HDL-cholesterol and triglyceride levels), and LDL-cholesterol, for the additional reason of being causally related to intima-media thickness, while it is physiologically not directly linked to insulin sensitivity. Accordingly, a p-value ≤ 0.0032 (Bonferroni corrected for 4 × 4 = 16 null hypotheses) was considered statistically significant. Associations with a p-value between 0.0032 and 0.05 were considered nominal.
Availability of materials and data
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Results
Demographic, anthropometric and metabolic characteristics of the subjects
The characteristics of the whole population, i.e. the 2332 subjects, are shown in the Table 1. All measurements covered a wide range, e.g. age 18–82 years, body weight 42–244 kg, BMI 16.30–86.45 kg/m2, waist circumference 38–185 cm, TAT mass 9.98–56.32 kg, VAT mass 0.36–8.90 kg, liver fat content 0.16–30.11%, fasting FFA 80–3756 μM, 2-hour FFA 10–1497 μM, total cholesterol 63–468 mg/dl, LDL-cholesterol 15–295 mg/dl, HDL-cholesterol 24–138 mg/dl, triglycerides 15–3202 mg/dl, apolipoprotein AI 54–316 mg/dl, apolipoprotein B 37–187 mg/dl, insulin sensitivity 2.19–85.37 1019 l2∙mol−2 as assessed by the OGTT, 0.008–0.472 106 l∙kg−1∙min−1 as measured by the clamp.
Genoty** of GRK5 tagging SNPs
The 2332 study participants were genotyped for the three SNPs rs1980030, rs10466210, rs9325562 in intron 1, and the SNP rs10886471 in intron 3 of GRK5. All SNPs were in Hardy-Weinberg equilibrium (all p > 0.05). The observed MAFs were 0.440 (rs1980030), 0.072 (rs10466210), 0.356 (rs9325562), 0.467 (rs10886471), and were similar to those provided by HapMap for the Central European population (0.369, 0.081, 0.283, and 0.455, respectively). According to the HapMap data (Fig. 1), the genetic linkage between the three SNPs in intron 1 was low or moderate with minimal r2 = 0.03 and maximal r2 = 0.67.
Associations of GRK5 SNPs with body fat compartments and liver fat content
After adjustment for age and gender, none of the four SNPs showed significant associations with BMI, waist circumference, TAT mass or VAT mass (Table 2 and Supplemental Table 2). A nominal association of the SNP rs10466210 with VAT mass (p = 0.022 in the additive, p = 0.018 in the dominant model, Table 2) was observed. Similarly, we found no significant association of any of the SNPs with liver fat content, as measured by 1H-MR spectroscopy (Table 2 and Supplemental Table 2).
Associations of GRK5 SNPs with glycemia, insulin sensitivity and insulin secretion
Neither fasting nor 2-hour post OGTT glycemia and insulinemia, or insulin sensitivity assessed by the HOMA-IR or during the OGTT, or measured by the clamp (adjusted for gender, age and BMI) were associated with any of the four SNPs. We observed a nominally significant association of the SNP rs10466210 with glycated hemoglobin: carriers of the minor A-allele had higher glycated hemoglobin levels (p = 0.0088 in the additive, p = 0.0057 in the dominant model, Table 2). However, no other SNP was significantly related to glycated hemoglobin levels. Likewise, the four SNPs were not associated with adjusted insulin secretion (Table 2 and Supplemental Table 2).
Associations of GRK5 SNPs with plasma lipids
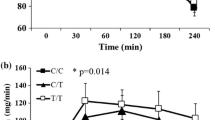
In contrast to the absence of any association or only rather sporadic associations of the GRK5 SNPs with body fat mass and body fat distribution, as well as glucose homeostasis, we found robust associations of two SNPs, rs10466210 and rs1980030, with total- and LDL-cholesterol, and apolipoprotein B levels, which is known to be the main protein of LDL-particles, but not with HDL-cholesterol or triglyceride levels (Table 2 and Fig. 2). In particular, the minor A-allele of rs10466210 was significantly associated with higher total cholesterol (p = 0.0018 in the additive and p = 0.0019 in the dominant model), LDL-cholesterol (p = 0.0031 in the additive model) and apolipoprotein B (p = 0.0034 in the additive and p = 0.0029 in the dominant model) levels, withstanding Bonferroni correction in all instances. The minor G-allele of rs1980030 was also related to higher total cholesterol, LDL-cholesterol and apolipoprotein B concentrations, but the associations fell very short from being significant after Bonferroni correction for total cholesterol (p = 0.0035 in the additive model and p = 0.0037 in the dominant model) and were only nominally significant for LDL-cholesterol and apolipoprotein B (p = 0.0081 and p = 0.0122, respectively in the additive model, and p = 0.036 and p = 0.032, respectively in the dominant model), presumably due to the lower effect size of the SNP (Table 2). We performed post hoc power analyses of the associations of the SNP with the lowest minor allele frequency, rs10466210, in the additive model with total cholesterol, LDL-cholesterol and apolipoprotein B, all adjusted for gender, age, BMI and lipid-lowering medication. Based on the Bonferroni-corrected α-level of 0.0032, our study was sufficiently powered (1-β > 0.8) to detect effect sizes as small as 3 mg/dl for all three traits (1-β = 0.83 for total cholesterol, 0.93 for LDL-cholesterol and 0.99 for apolipoprotein B). The other 2 SNPs, rs9325562 and rs10886471, were not related to any of the plasma lipids or lipoproteins (Supplemental Table 2). The phenome-wide association results for all 4 SNPs are also shown as Manhattan plots (Fig. 3). Although there was no association of the SNPs with weight or BMI, and in order to exclude the possibility that the significant associations were driven by extremely obese subjects, we repeated these analyses after excluding subjects with BMI ≥ 65 kg/m2 (n = 14). The results (p-values) were virtually the same (Supplemental Table 3).

Associations of total- and LDL-cholesterol, as well as apolipoprotein B levels with rs10466210 (A) and rs1980030 (B) SNPs in GRK5 gene in 2332 subjects. For statistical analyses, all lipid measurements were log-transformed and adjusted for gender, age, BMI and lipid-lowering medication. Adjusted back-transformed values and box blots (showing median sample values and the 75th and 25th quantiles) are depicted.

Manhattan plot of the phenome-wide association results. ISI, insulin sensitivity index; IGI, insulinogenic index; C-pep, C-peptide; glc, glucose; AUC, Area Under the Curve.
Associations of GRK5 SNPs with carotid intima-media thickness (IMT)
Having found significant associations of two SNPs with LDL-cholesterol and apolipoprotein B levels, we set out to explore whether these SNPs were associated with IMT of the common carotid artery, a known early marker of atherosclerosis. IMT measurements were available in a subgroup of 590 subjects. We observed a trend for an association of the SNP rs10466210 [GG: n = 514, IMT 0.535 (0.465–0.639) mm, median (interquartile range); GA: n = 75, IMT 0.575 (0.494–0.670) mm; AA: n = 1, IMT 0.750 mm] with IMT (p = 0.075 in the additive model and p = 0.10 in the dominant model). The minor allele A, which was significantly associated with higher total- and LDL-cholesterol, and apolipoprotein B levels in the whole study population, showed a trend for an association with higher carotid IMT in this smaller group. The SNP rs1980030 was not associated with IMT (p > 0.57 in both models), presumably due to its lower effect size.
Discussion
In this study, we investigated possible associations of selected common SNPs in GRK5 with body fat mass and distribution, and measurements of glucose and lipid metabolism. We found robust associations of the minor alleles of two SNPs, rs10466210 and rs1980030, with higher total- and LDL-cholesterol, as well as with higher apolipoprotein B (apoB) levels. We detected no association of either of the SNPs with HDL-cholesterol or triglyceride levels. Of particular note, the two aforementioned SNPs were not linked to each other (r2 = 0.15, Fig. 1).
A possible impact of GRK5 on atherosclerosis was suggested in in vitro and in vivo studies14,15,16. Our findings were somehow unexpected, because they are not completely in agreement with the results of studies in Grk5 knock-out mice9,10. With regard to plasma lipids, these animals had, under a high-fat diet, higher plasma triglyceride levels, but not significantly elevated total-, HDL- or LDL-cholesterol levels. However, these animals also displayed a higher insulin resistance and a higher liver fat content10, which may account for the higher plasma triglyceride levels (although, one would also expect them to have lower HDL-cholesterol levels29). Besides, under a standard diet there was no difference in plasma triglyceride levels between knock-out and wild-type mice. In our study none of the SNPs was related with insulin resistance. Thus, it is not surprising that the SNPs were not associated with triglycerides, either. Of note, LDL-cholesterol levels were higher in Grk5−/− mice, although this relationship was not statistically significant10. In any case, we do not believe that the data from knock-out mice can raise doubts about the robustness of our findings. In addition to the more or less expected differences between rodents and humans, the association of the two SNPs with LDL-cholesterol levels is, according to our analyses, strong, withstands correction for multiple testing (at least for rs10466210) and is virtually ‘replicated’ in the association of the SNPs with a separate measurement, apoB, which represents the main apoprotein of LDL-particles. In addition, the associations were significant independently of gender, BMI and lipid-lowering medication. In the Global Lipids Genetics Consortium the associations of the same two SNPs with total- and LDL-cholesterol levels were not significant, but adjustment was done only for age and sex, and not for BMI or medication (http://csg.sph.umich.edu/abecasis/public/lipids2013/)30.
It is very difficult to assume a mechanism by which GRK5 may affect LDL-cholesterol metabolism. This is of course due to the large number of GPCRs and the large diversity of their possible ligands. Furthermore, it is not known whether the two SNPs found to be associated with LDL-cholesterol and apoB levels are functional, or whether they may simply be linked to other functional SNPs. The risk alleles of the SNPs rs4752300 and rs10886471 were found to enhance GRK5 mRNA expression in peripheral blood cells and in adipose tissue, respectively11,31. According to HapMap, the SNP rs1980030 is in linkage disequilibrium with the SNP rs4752300 (r2 = 0.97, Fig. 1).
Following our main finding of associations of the two SNPs with LDL-cholesterol and apoB levels, we further tested whether there may be significant associations of the GRK5 SNPs with IMT, an early marker of atherosclerosis. We detected a trend for an association of the SNP rs10466210 with IMT. The reason why the association did not reach statistical significance may be the fact that measurements of IMT were only available in about a quarter of the participants. No significant association of SNP rs1980030 with IMT was found. This may be explained, in addition to the limited number of available IMT measurements, by the clearly smaller effect size of the association of this SNP with LDL-cholesterol and apoB concentrations (Table 2). Nevertheless, our findings regarding IMT point to an involvement of GRK5 in cholesterol metabolism with potential clinical relevance.
With the only exception of isolated nominal associations of the SNP rs10466210 with VAT mass and glycated hemoglobin, which probably represent chance findings, we found no significant associations of the four SNPs in GRK5 with body fat mass and distribution and measurements of glucose metabolism. In contrast, Grk5−/− mice were resistant to adipogenesis and adipocyte differentiation of WAT under a high fat diet, while they concomitantly developed fatty liver. They also had higher glucose and insulin levels, and were more insulin resistant9,10. Differences between the species constitute an obvious explanation for the apparent conflicting findings in knock-out mice and humans. Furthermore, since all SNPs we studied in humans were intronic, they may only slightly modulate gene expression, thereby, exerting a rather small effect on metabolism, while knocking-out of the whole gene in rodents may result in more potent and more complex effects. For instance, while insulin resistance may account for the higher insulin levels, and the higher insulin and glucose levels may account for liver fat accumulation, the reasons for insulin resistance and higher glucose levels in these animals are unknown.
To our knowledge, there are principally two studies in the literature linking GRKs with glucose metabolism in humans. The first was a genome-wide association study, which found a significant relationship of the SNP rs10886471 in GRK5 with type 2 diabetes. The risk allele was associated with higher insulin, but not with higher glucose levels11. The second study reported that the same SNP exerts its effect also by generating either an intronic (CA)16 STR, which was associated with an increased risk for prediabetes, or a (CA)15 to (CA)19 STR, which were all related to a decreased prediabetes risk12. Recently, a rather small case-control study confirmed the association of rs10886471 with prediabetes and type 2 diabetes, as well as with so-called differentiated symptoms of diabetes32. However, the association of the SNP rs10886471 with type 2 diabetes in the first study was found to be specific for East Asians, and the second and third studies were performed in only a Chinese Hainan Island population. It is, therefore, not surprising that we found no significant association of the SNP rs10886471 with measurements of glucose metabolism in our European cohort. A possible explanation for the ethnic differences may be that the risk allele frequency of the SNP rs10886471 in East Asians is much higher than in Europeans (0.786 in the HapMap CHB population and 0.455 in the HapMap CEU population, respectively) (http://grch37.ensembl.org/Homo_sapiens/Info/Index). Of note, whether there was an association of the particular SNP with lipid metabolism was not investigated in either of these two studies.
Our study has some limitations. First, it is unclear whether our findings and conclusions can be applied to other populations. Since there is no other study in the literature investigating the effect of GRK5 SNPs on cholesterol levels in humans, our results need replication in other ethnic groups. Second, our sample consisted of a cohort covering a wide range of age, adiposity, and insulin sensitivity. Thus, an impact of the SNPs in an older or a more insulin resistant population cannot be excluded. Finally, we studied only four common variants from selected gene regions and with MAFs ≥ 0.05, so that further SNPs in GRK5 with possible effect on cholesterol levels may exist.
To summarize, in this study we report robust associations of two SNPs in GRK5 gene with total and LDL-cholesterol as well as apoB levels. In our population, homozygotes for the minor (risk) allele had up to 20% higher cholesterol levels compared to homozygotes for the major allele. GRK5 may thus be involved in cholesterol metabolism. Furthermore, we detected a week association of one of the two SNPs with IMT. Although this association fell short from being statistically significant, it may be clinically relevant, because it is in line with data from in vitro and in vivo animal studies suggesting that GRK5 may have direct and indirect effects on atherosclerotic cardiovascular disease, and that apoB may be more predictive for the progression of cardiovascular disease than even oxidized LDL33. Thus, GRK5 represents a potential promising target for treatment strategies not only of total-, and particularly LDL-cholesterol levels, but possibly also of cardiovascular disease.
References
Hullmann, J., Traynham, C. J., Coleman, R. C. & Koch, W. J. The expanding GRK interactome: Implications in cardiovascular disease and potential for therapeutic development. Pharmacol. Res 110, 52–64 (2016).
Homan, K. T. et al. Identification and structure-function analysis of subfamily selective G protein-coupled receptor kinase inhibitors. ACS Chem. Biol 10, 310–319 (2015).
Ribas, C. et al. The G protein-coupled receptor kinase (GRK) interactome: role of GRKs in GPCR regulation and signaling. Biochim. Biophys. Acta 1768, 913–922 (2007).
Sorriento, D. et al. The G-protein-coupled receptor kinase 5 inhibits NFkappaB transcriptional activity by inducing nuclear accumulation of IkappaB alpha. Proc. Natl. Acad. Sci. USA 105, 17818–17823 (2008).
Chen, Y. et al. GRK5 promotes F-actin bundling and targets bundles to membrane structures to control neuronal morphogenesis. J. Cell Biol 194, 905–920 (2011).
Patial, S. et al. G-protein coupled receptor kinase 5 mediates lipopolysaccharide-induced NFkappaB activation in primary macrophages and modulates inflammation in vivo in mice. J. Cell Physiol 226, 1323–1333 (2011).
So, C. H., Michal, A. M., Mashayekhi, R. & Benovic, J. L. G protein-coupled receptor kinase 5 phosphorylates nucleophosmin and regulates cell sensitivity to polo-like kinase 1 inhibition. J Biol Chem 287, 17088–17099 (2012).
Gold, J. I., Gao, E., Shang, X., Premont, R. T. & Koch, W. J. Determining the absolute requirement of G protein-coupled receptor kinase 5 for pathological cardiac hypertrophy: short communication. Circ. Res 111, 1048–1053 (2012).
Wang, F., Wang, L., Shen, M. & Ma, L. GRK5 deficiency decreases diet-induced obesity and adipogenesis. Biochem. Biophys. Res. Commun 421, 312–317 (2012).
Wang, L., Shen, M., Wang, F. & Ma, L. GRK5 ablation contributes to insulin resistance. Biochem. Biophys. Res. Commun 429, 99–104 (2012).
Li, H. et al. A genome-wide association study identifies GRK5 and RASGRP1 as type 2 diabetes loci in Chinese Hans. Diabetes 62, 291–298 (2013).
**a, Z., Yang, T., Wang, Z., Dong, J. & Liang, C. GRK5 intronic (CA)n polymorphisms associated with type 2 diabetes in Chinese Hainan Island. PLoS. ONE 9, e90597 (2014).
Kim, J. I., Chakraborty, P., Wang, Z. & Daaka, Y. G-protein coupled receptor kinase 5 regulates prostate tumor growth. J. Urol 187, 322–329 (2012).
Chen, X. et al. G-protein-coupled receptor kinase 5 phosphorylates p53 and inhibits DNA damage-induced apoptosis. J Biol Chem 285, 12823–12830 (2010).
Martini, J. S. et al. Uncovering G protein-coupled receptor kinase-5 as a histone deacetylase kinase in the nucleus of cardiomyocytes. Proceedings of the National Academy of Sciences of the United States of America 105, 12457–12462 (2008).
Wu, J. H. et al. G protein-coupled receptor kinase-5 attenuates atherosclerosis by regulating receptor tyrosine kinases and 7-transmembrane receptors. Arterioscler. Thromb. Vasc. Biol 32, 308–316 (2012).
Freedman, N. J. et al. Phosphorylation and desensitization of human endothelin A and B receptors. Evidence for G protein-coupled receptor kinase specificity. J. Biol. Chem 272, 17734–17743 (1997).
Kantartzis, K. et al. High cardiorespiratory fitness is an independent predictor of the reduction in liver fat during a lifestyle intervention in non-alcoholic fatty liver disease. Gut 58, 1281–1288 (2009).
Kantartzis, K. et al. Dissociation between fatty liver and insulin resistance in humans carrying a variant of the patatin-like phospholipase 3 gene. Diabetes 58, 2616–2623 (2009).
Stefan, N. et al. Identification and characterization of metabolically benign obesity in humans. Arch. Intern. Med 168, 1609–1616 (2008).
Stefan, N., Fritsche, A., Schick, F. & Haring, H. U. Phenotypes of prediabetes and stratification of cardiometabolic risk. Lancet Diabetes Endocrinol 4, 789–798 (2016).
Stefan, N. et al. Inhibition of 11beta-HSD1 with RO5093151 for non-alcoholic fatty liver disease: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol 2, 406–416 (2014).
Machann, J. et al. Follow-up whole-body assessment of adipose tissue compartments during a lifestyle intervention in a large cohort at increased risk for type 2 diabetes. Radiology 257, 353–363 (2010).
Matsuda, M. & DeFronzo, R. A. Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 22, 1462–1470 (1999).
Matthews, D. R. et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Herzberg-Schafer, S. A. et al. Evaluation of fasting state-/oral glucose tolerance test-derived measures of insulin release for the detection of genetically impaired beta-cell function. PLoS. ONE 5, e14194 (2010).
Kantartzis, K. et al. Upstream transcription factor 1 gene polymorphisms are associated with high antilipolytic insulin sensitivity and show gene-gene interactions. J. Mol. Med 85, 55–61 (2007).
Balletshofer, B. M. et al. Early carotid atherosclerosis in overweight non-diabetic individuals is associated with subclinical chronic inflammation independent of underlying insulin resistance. Horm. Metab Res 37, 331–335 (2005).
Kantartzis, K. et al. Fatty liver is independently associated with alterations in circulating HDL2 and HDL3 subfractions. Diabetes Care 31, 366–368 (2008).
Willer, C. J. et al. Discovery and refinement of loci associated with lipid levels. Nat. Genet 45, 1274–1283 (2013).
Nica, A. C. et al. The architecture of gene regulatory variation across multiple human tissues: the MuTHER study. PLoS. Genet 7, e1002003 (2011).
Dou, H. Y. et al. Association between genetic variants and characteristic symptoms of type 2 diabetes: A matched case-control study. Chinese journal of integrative medicine 23, 415–424 (2017).
Wu, T. et al. Is plasma oxidized low-density lipoprotein, measured with the widely used antibody 4E6, an independent predictor of coronary heart disease among U.S. men and women? J. Am. Coll. Cardiol 48, 973–979 (2006).
Acknowledgements
The authors thank all study participants for their cooperation. We gratefully acknowledge the excellent technical assistance of Alke Guirguis, Roman-Georg Werner, Dorothee Neuscheler, Sieglinde Haug, and Elisabeth Metzinger. The study was supported in part by a grant from the German Federal Ministry of Education and Research (BMBF) to the German Center for Diabetes Research (DZD e.V.). We acknowledge support by the Deutsche Forschungsgemeinschaft and the Open Access Publishing Fund of the University of Tübingen.
Author information
Authors and Affiliations
Contributions
Study concept and design: H.S., A.U., M.F., S.Z.L., A.P., K.K. Data collection: S.Z.L., A.P., F.M., M.K., A.L.S., R.W., J.M., F.S., H.S., K.K. Analysis and interpretation of data: S.Z.L., A.P., F.M., E.R., A.F., N.S., H.S., H.U.H., K.K. Statistical analysis: H.S., N.S., K.K. Drafting of the manuscript: S.Z.L., H.U.H., N.S., H.S., K.K. Critical revision of the manuscript: A.F., M.F., M.H., N.S., H.S., A.U., H.U.H., K.K. Administrative, technical and material support: A.P., F.M., J.M., F.S., H.S., H.U.H. Study supervision: H.S., K.K., H.U.H.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lutz, S.Z., Falcenberg, M., Machicao, F. et al. Single Nucleotide Polymorphisms in the G-Protein Coupled Receptor Kinase 5 (GRK5) Gene are associated with Plasma LDL-Cholesterol Levels in Humans. Sci Rep 8, 7745 (2018). https://doi.org/10.1038/s41598-018-26055-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-26055-7
- Springer Nature Limited