
Abstract
Objective
To describe 20-year risk factor trajectories according to initial weight/health status and investigate the extent to which baseline differences explain greater mortality among metabolically healthy obese (MHO) individuals than healthy non-obese individuals.
Methods
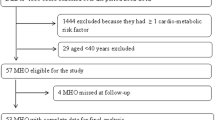
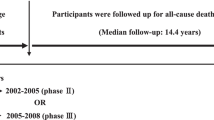
The sample comprised 6529 participants in the Whitehall II study who were measured serially between 1991–1994 and 2012–2013. Baseline weight (non-obese or obese; body mass index (BMI) ≥30 kg/m2) and health status (healthy or unhealthy; two or more of hypertension, low high-density lipoprotein cholesterol (HDL-C), high triglycerides, high glucose, and high homeostatic model assessment of insulin resistance (HOMA-IR)) were defined. The relationships of baseline weight/health status with 20-year trajectories summarizing ~25,000 observations of systolic and diastolic blood pressures, HDL-C, triglycerides, glucose, and HOMA-IR were investigated using multilevel models. Relationships of baseline weight/health status with all-cause mortality up until July 2015 were investigated using Cox proportional hazards regression.
Results
Trajectories tended to be consistently worse for the MHO group compared to the healthy non-obese group (e.g., glucose by 0.21 (95% CI 0.09, 0.33; p < 0.001) mmol/L at 20-years of follow-up). Consequently, the MHO group had a greater risk of mortality (hazard ratio 2.11 (1.24, 3.58; p = 0.006)) when the referent group comprised a random sample of healthy non-obese individuals. This estimate, however, attenuated (1.34 (0.85, 2.13; p = 0.209)) when the referent group was matched to the MHO group on baseline risk factors.
Conclusions
Worse baseline risk factors may explain any difference in mortality risk between obese and non-obese groups both labelled as healthy, further challenging the concept of MHO.
Similar content being viewed by others

Introduction
Obesity is a major public health problem because of its adverse consequences for long-term health and well-being [1]. Clearly, however, not all obese individuals have the same cardio-metabolic disease risk factor (e.g., blood pressure and fasting glucose levels) profiles. The concept that someone can be obese yet metabolically healthy, most commonly called “metabolically healthy obesity (MHO)”, has been highly controversial and widely debated [2, 3]. In particular, two main types of epidemiological studies have questioned whether or not MHO is truly a benign condition, relative to metabolically healthy non-obese (MHNO). The first has investigated the progression of the MHO phenotype over time, demonstrating that this group tends to develop risk factors and transition to being unhealthy more frequently than their non-obese counterparts [4,5,6,7,8,9,10,11]. Hamer et al. [10] for example, demonstrated that, over 8 years of follow-up in the English Longitudinal Study of Ageing, 45% of MHO participants transitioned to an unhealthy state compared to 17% of MHNO participants [10]. The second type of study has investigated disease prognosis or mortality, demonstrating a ranking of risk according to both weight and health status [12,13,14,12,13,14,13]. While many of these studies present baseline differences in cardio-metabolic disease risk factors between these two groups, which manifest from dichotomizing continuous variables, few discuss the impact of these baseline differences on the reported relationships.
To illustrate the fact that applying binary cutoffs to define weight/health status induces differences in cardio-metabolic disease risk factors between MHO vs MHNO groups (and between MUO vs MUNO groups) we also present 20-year trajectories. For HDL-C and triglycerides, higher average values among MHO than MHNO individuals remained remarkably similar in magnitude across follow-up, thereby suggesting that accounting for baseline differences (as in our mortality analyses) is approximately the same as accounting for cumulative differences over time. The differences for SBP and DBP reduced marginally over time, but those for glucose and HOMA-IR increased (e.g., from ~0.0 mmol/L at baseline to 0.2 mmol/L at 20-years for glucose). These findings are in agreement with previous Whitehall II study analyses showing that, relative to MHNO, the incidence of MHO individuals develo** insulin resistance (incidence ratio 3.78 (95% CI 2.38, 5.99)) or high blood glucose (2.27 (1.43, 3.61)) over 20-years is higher than that for hypertension (1.35 (1.03, 1.77)) [5]. It appears that impairment of the glucose-insulin regulatory system might be the main factor driving transition to an unhealthy state, which would explain why the meta-analysed association of MHO with incident type 2 diabetes (relative risk ~4.0) is stronger than that for cardiovascular disease (relative risk ~1.2) [29, 32].
Importantly, our results do not mean that a person cannot be obese and have no complications. Key principles of normal variation mean that two obese individuals, even with exactly the same BMI, can (and most likely do) have different levels of cardio-metabolic disease risk factors. The idea that some people demonstrate some level of “resilience to obesity” is statistically plausible. And experimental studies in animal models [35, 36], in addition observational studies in humans [37], have started to reveal possible biological mechanisms (e.g., a genetic variant in humans near ISR1 has been shown to be related to both increased percentage body fat and a favourable metabolic profile [38]) beyond the obvious (e.g., high BMI due to high fat-free mass). The problem is that MHO is a crude way of capturing heterogeneity in health among individuals with the same BMI level. For this reason, the concept of MHO may have limited clinically utility. In a meta-analysis of nearly 150,000 participants from 14 cohort studies, Lotta et al., for example, found that binary definitions of metabolic health only had satisfactory sensitivity (0.81 (95% CI 0.76, 0.86)) and low specificity (0.42 (0.35, 0.49) for predicting incident type 2 diabetes in obese individuals [33]. Despite these limitations, a large part of the field has not moved on from asking whether or not people can be obese yet healthy. In particular, we think that more research is needed on (1) the joint distributions of BMI and cardio-metabolic disease risk factors and (2) the life course exposures that might modify the relationship of BMI with incident disease or mortality. Such investigation would help us better understand the proportion and type of people who develop a high BMI without any adverse consequences.
The main strength of the present article is the thorough analysis of longitudinal data collected on a relatively large sample over 20 years of follow-up to address a novel research question. In terms of limitations, (1) the Whitehall II study sample is not representative of the wider UK population, although standard risk factor-cardiovascular disease associations in Whitehall II are comparable to those found in nationally representative studies [39], (2) we only used one definition of MHO, which does not incorporate other measures/indicators of adiposity (e.g., waist circumference), (3) the estimated relationships might be subject to residual confounding, and (4) there were not enough cases to investigate cause-specific mortality. While these types of considerations are important when trying to infer causality from observational data, we believe they are less important for our given research aim to demonstrate why other studies (which are subject to the same limitations) find what they find. The results we present are a demonstration of some of the possible consequences of converting continuous variables to binary concepts, and may be relevant to discussions on other related phenomena, such as the “fat but fit” paradigm [40].
Conclusion
This paper demonstrates how dichotomising continuous variables results in different levels of cardio-metabolic disease risk factors at baseline and over 20 years of follow-up between MHO and MHNO individuals, despite both groups having the same label of “healthy”, and to a lesser extent between MUO and MUNO individuals. The greater disease and mortality risk of MHO compared to MHNO individuals, observed in large-scale epidemiological studies, is likely largely explained by the more deleterious risk factor trajectories (in the MHO group) that result from crude stratification. Future research needs to better quantify heterogeneity in disease and mortality risk among people with the same BMI, and investigate the characteristics and life-course factors that explain why some people develop a disease or die while other people with the same BMI do not.
References
GBD 2015 Obesity Collaborators, Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N Engl J Med. 2017;377:13–27.
Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37:2315–81.
Stefan N, Haring HU, Schulze MB Metabolically healthy obesity: the low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol. 2017. https://doi.org/10.1016/S2213-8587(17)30292-9.
Appleton SL, Seaborn CJ, Visvanathan R, Hill CL, Gill TK, Taylor AW, et al. Diabetes and cardiovascular disease outcomes in the metabolically healthy obese phenotype: a cohort study. Diabetes Care. 2013;36:2388–94.
Bell JA, Hamer M, Batty GD, Singh-Manoux A, Sabia S, Kivimaki M. Incidence of metabolic risk factors among healthy obese adults: 20-year follow-up. J Am Coll Cardiol. 2015;66:871–3.
Bell JA, Hamer M, Sabia S, Singh-Manoux A, Batty GD, Kivimaki M. The natural course of healthy obesity over 20 years. J Am Coll Cardiol. 2015;65:101–2.
Bobbioni-Harsch E, Pataky Z, Makoundou V, Laville M, Disse E, Anderwald C, et al. From metabolic normality to cardiometabolic risk factors in subjects with obesity. Obesity. 2012;20:2063–9.
den Engelsen C, Gorter KJ, Salome PL, Rutten GE. Development of metabolic syndrome components in adults with a healthy obese phenotype: a 3-year follow-up. Obesity. 2013;21:1025–30.
Guo F, Garvey WT. Cardiometabolic disease risk in metabolically healthy and unhealthy obesity: Stability of metabolic health status in adults. Obesity. 2016;24:516–25.
Hamer M, Bell JA, Sabia S, Batty GD, Kivimaki M. Stability of metabolically healthy obesity over 8 years: the English Longitudinal Study of Ageing. Eur J Endocrinol. 2015;173:703–8.
Soriguer F, Gutierrez-Repiso C, Rubio-Martin E, Garcia-Fuentes E, Almaraz MC, Colomo N, et al. Metabolically healthy but obese, a matter of time? Findings from the prospective Pizarra study. J Clin Endocrinol Metab. 2013;98:2318–25.
Aung K, Lorenzo C, Hinojosa MA, Haffner SM. Risk of develo** diabetes and cardiovascular disease in metabolically unhealthy normal-weight and metabolically healthy obese individuals. J Clin Endocrinol Metab. 2014;99:462–8.
Caleyachetty R, Thomas GN, Toulis KA, Mohammed N, Gokhale KM, Balachandran K, et al. Metabolically healthy obese and incident cardiovascular disease events among 3.5 million men and women. J Am Coll Cardiol. 2017;70:1429–37.
Fan J, Song Y, Chen Y, Hui R, Zhang W. Combined effect of obesity and cardio-metabolic abnormality on the risk of cardiovascular disease: a meta-analysis of prospective cohort studies. Int J Cardiol. 2013;168:4761–8.
Gunter MJ, **e X, Xue X, Kabat GC, Rohan TE, Wassertheil-Smoller S, et al. Breast cancer risk in metabolically healthy but overweight postmenopausal women. Cancer Res. 2015;75:270–4.
Hinnouho GM, Czernichow S, Dugravot A, Nabi H, Brunner EJ, Kivimaki M, et al. Metabolically healthy obesity and the risk of cardiovascular disease and type 2 diabetes: the Whitehall II cohort study. Eur Heart J. 2015;36:551–9.
Lassale C, Tzoulaki I, Moons KGM, Sweeting M, Boer J, Johnson L et al. Separate and combined associations of obesity and metabolic health with coronary heart disease: a pan-European case-cohort analysis. Eur Heart J. 2017. https://doi.org/10.1093/eurheartj/ehx448.
Murphy N, Cross AJ, Abubakar M, Jenab M, Aleksandrova K, Boutron-Ruault MC, et al. A nested case-control study of metabolically defined body size phenotypes and risk of colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). PLoS Med. 2016;13:e1001988
Hinnouho GM, Czernichow S, Dugravot A, Batty GD, Kivimaki M, Singh-Manoux A. Metabolically healthy obesity and risk of mortality: does the definition of metabolic health matter? Diabetes Care. 2013;36:2294–300.
Sung KC, Ryu S, Cheong ES, Kim BS, Kim BJ, Kim YB, et al. All-cause and cardiovascular mortality among Koreans: effects of obesity and metabolic health. Am J Prev Med. 2015;49:62–71.
Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, et al. Health inequalities among British civil servants: the Whitehall II study. Lancet. 1991;337:1387–93.
Bouillon K, Singh-Manoux A, Jokela M, Shipley MJ, Batty GD, Brunner EJ, et al. Decline in low-density lipoprotein cholesterol concentration: lipid-lowering drugs, diet, or physical activity? Evidence from the Whitehall II study. Heart. 2011;97:923–30.
Goldberg DP The Detection of Psychiatric Illness by Questionnaire. London: Oxford University Press; 1972.
Stringhini S, Sabia S, Shipley M, Brunner E, Nabi H, Kivimaki M, et al. Association of socioeconomic position with health behaviors and mortality. JAMA. 2010;303:1159–66.
Wildman RP, Muntner P, Reynolds K, McGinn AP, Rajpathak S, Wylie-Rosett J, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999-2004). Arch Intern Med. 2008;168:1617–24.
Johnson W. Analytical strategies in human growth research. Am J Hum Biol. 2015;27:69–83.
Johnson W, Balakrishna N, Griffiths PL. Modeling physical growth using mixed effects models. Am J Phys Anthropol. 2013;150:58–67.
Leckie G, Charlton C. runmlwin: a program to run the MLwiN multilevel software from within Stata. J Stat Softw. 2012;52:1–40.
Bell JA, Kivimaki M, Hamer M. Metabolically healthy obesity and risk of incident type 2 diabetes: a meta-analysis of prospective cohort studies. Obes Rev. 2014;15:504–15.
Eckel N, Meidtner K, Kalle-Uhlmann T, Stefan N, Schulze MB. Metabolically healthy obesity and cardiovascular events: a systematic review and meta-analysis. Eur J Prev Cardiol. 2016;23:956–66.
Jokela M, Hamer M, Singh-Manoux A, Batty GD, Kivimaki M. Association of metabolically healthy obesity with depressive symptoms: pooled analysis of eight studies. Mol Psychiatry. 2014;19:910–4.
Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions?: a systematic review and meta-analysis. Ann Intern Med. 2013;159:758–69.
Lotta LA, Abbasi A, Sharp SJ, Sahlqvist AS, Waterworth D, Brosnan JM, et al. Definitions of metabolic health and risk of future type 2 diabetes in BMI categories: a systematic review and network meta-analysis. Diabetes Care. 2015;38:2177–87.
Zhang J, Jiang H, Chen J. Combined effect of body mass index and metabolic status on the risk of prevalent and incident chronic kidney disease: a systematic review and meta-analysis. Oncotarget. 2017;8:35619–29.
Gavrilova O, Marcus-Samuels B, Graham D, Kim JK, Shulman GI, Castle AL, et al. Surgical implantation of adipose tissue reverses diabetes in lipoatrophic mice. J Clin Invest. 2000;105:271–8.
Medina-Gomez G, Gray SL, Yetukuri L, Shimomura K, Virtue S, Campbell M, et al. PPAR gamma 2 prevents lipotoxicity by controlling adipose tissue expandability and peripheral lipid metabolism. PLoS Genet. 2007;3:e64
Primeau V, Coderre L, Karelis AD, Brochu M, Lavoie ME, Messier V, et al. Characterizing the profile of obese patients who are metabolically healthy. Int J Obes. 2011;35:971–81.
Kilpelainen TO, Zillikens MC, Stancakova A, Finucane FM, Ried JS, Langenberg C, et al. Genetic variation near IRS1 associates with reduced adiposity and an impaired metabolic profile. Nat Genet. 2011;43:753–60.
Batty GD, Shipley M, Tabak A, Singh-Manoux A, Brunner E, Britton A, et al. Generalizability of occupational cohort study findings. Epidemiology. 2014;25:932–3.
Kennedy AB, Lavie CJ, Blair SN. Fitness or fatness: which is more important? JAMA. 2018;319:231–2.
Acknowledgements
We thank all participants in the Whitehall II Study, Whitehall II researchers, and support staff who make the study possible. Please refer to the Whitehall II data sharing policy at http://www.ucl.ac.uk/whitehallII/data-sharing. Whitehall II data are available to bona fide researchers for research purposes
Funding
This work was supported by the UK Medical Research Council (WJ New Investigator Research Grant: MR/P023347/1). W.J. and M.H. acknowledge support from the National Institute for Health Research (NIHR) Leicester Biomedical Research Centre, which is a partnership between University Hospitals of Leicester NHS Trust, Loughborough University, and the University of Leicester. J.A.B. is supported by a Cancer Research UK programme grant (C18281/A19169). The UK Medical Research Council (MR/K013351/1; G0902037), British Heart Foundation (RG/13/2/30098, PG/11/63/29011), and the US National Institutes of Health (R01HL36310, R01AG013196) have supported collection of data in the Whitehall II Study. M.K. was additionally supported by NordForsk and a Helsinki Institute of Life Science fellowship. All the funding sources had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author contributions
W.J. conceptualized the study, carried out the analyses, and drafted the initial manuscript. W.J., J.A.B., E.R., T.N., M.K., and M.H. made substantial contributions to the interpretation of the data, revised the manuscript critically for important intellectual content, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Johnson, W., Bell, J.A., Robson, E. et al. Do worse baseline risk factors explain the association of healthy obesity with increased mortality risk? Whitehall II Study. Int J Obes 43, 1578–1589 (2019). https://doi.org/10.1038/s41366-018-0192-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-018-0192-0
- Springer Nature Limited