
Abstract
Purpose
Community-based (CB) surgical training programs have traditionally been felt to offer an earlier operative experience than university-based programs (UB), with CB residents reporting higher levels of confidence to operate independently upon completion of residency. Greater autonomy during training may be one potential contributor of higher levels of confidence to operate independently, but this has not yet been evaluated. The purpose of this study was to compare resident operative autonomy ratings at different types of surgical training programs.
Methods
Surgical residents and faculty at 68 general surgery training programs used a workplace-based assessment app to assess the level of operative autonomy provided to residents. Ratings were collected using the Zwisch scale following cases that involved a categorical general surgery resident. Program type was determined based on designation in the American Medical Association’s Fellowship and Residency Electronic Interactive Database Access System (CB, UB, community-based university-affiliated (CBUA), or military). Linear mixed models were used to explore the association between program type and resident autonomy while accounting for differences in trainee post-graduate year (PGY) and other related factors.
Results
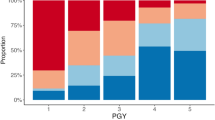
A total of 82,154 evaluations from 1,982 surgical faculty were included (CB: 3,409, CBUA: 12,629, and UB: 66,197). When adjusting for factors including PGY level, there was no significant difference in the adjusted resident autonomy ratings between program types by the end of training (CB = 2.54 (CI 2.44–2.64), CBUA = 2.48 (CI 2.43–2.53), UB = 2.49 (CI 2.45–2.52)). However, there was a difference in rate of change of autonomy, with CB programs reporting earlier operative autonomy.
Conclusions
There is no significant difference in the overall amount of operative autonomy provided to residents in university-based, community-based university-affiliated, or community-based general surgery training programs.


Similar content being viewed by others


References
Sullivan MC, Sue G, Bucholz E, Yeo H, Bell RH, Roman SA, et al. Effect of program type on the training experiences of 248 university, community, and US military-based general surgery residencies. J Am Coll Surg. 2012;214:53–60.
Bucholz EM. Our trainees’ confidence: results from a national survey of 4136 US general surgery residents. Arch Surg. 2011;146:907.
Vaughan A, Welling R, Boberg J. Surgical education in the new millennium: a community hospital perspective. Surg Clin North Am. 2004;84:1441–51.
Kearse LE, Zeineddin A, Schmiederer IS, Korndorffer JR, Lau JN. A 20-year review of surgical training case logs: is general surgery still general? Surgery. 2021. https://doi.org/10.1016/j.surg.2021.03.062.
Mattar SG, Alseidi AA, Jones DB, Jeyarajah DR, Swanstrom LL, Aye RW, et al. General surgery residency inadequately prepares trainees for fellowship: results of a survey of fellowship program directors. Ann Surg Sept. 2013;2013(258):440–9.
George BC, Bohnen JD, Williams RG, Meyerson SL, Schuller MC, Clark MJ, et al. Readiness of US general surgery residents for independent practice. Ann Surg. 2017;266:582–94.
Fronza JS, Prystowsky JP, DaRosa D, Fryer JP. Surgical residents’ perception of competence and relevance of the clinical curriculum to future practice. J Surg Educ. 2012;69:792–7.
Patel M, Bhullar JS, Subhas G, Mittal V. Present status of autonomy in surgical residency—a program director’s perspective. Am Surg. 2015;81:786–90.
Kim SC, Fisher JG, Delman KA, Hinman JM, Srinivasan JK. Cadaver-based simulation increases resident confidence, initial exposure to fundamental techniques, and may augment operative autonomy. J Surg Educ. 2016;73:e33-41.
DaRosa DA, Zwischenberger JB, Meyerson SL, George BC, Teitelbaum EN, Soper NJ, et al. A theory-based model for teaching and assessing residents in the operating room. J Surg Educ. 2013;70:24–30.
FREIDATM AMA Residency and Fellowship Programs Database. https://freida.ama-assn.org/. Accessed 12 Nov 2021.
Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67:1–48.
Kuznetsova A, Brockhoff PB, Christensen RHB. lmertest package: tests in linear mixed effects models. J Stat Softw. 2017;82:1–26.
Abbott KL, Krumm AE, Clark MJ, Kendrick DE, Kelley JK, George BC. Representativeness of workplace-based operative performance assessments for resident operative experience. J Surg Educ. 2022;S1931–7204(21):00377–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No authors report financial or non-financial interests that are related directly or indirectly to this work.
Supplementary Information
Below is the link to the electronic supplementary material.
44186_2022_26_MOESM2_ESM.docx
Table S2 Linear mixed model results for faculty evaluations of residents, when interaction term between program type and PGY level was included (DOCX 12 kb)
44186_2022_26_MOESM4_ESM.docx
Table S4 Linear mixed model results for resident evaluations of self, when interaction term between program type and PGY level was included (DOCX 12 kb)
Rights and permissions
About this article

Cite this article
Gates, R.S., Bidwell, S.S., Chen, X. et al. Resident operative autonomy: do community-based programs offer more than university-based programs?. Global Surg Educ 1, 26 (2022). https://doi.org/10.1007/s44186-022-00026-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44186-022-00026-z