
Abstract
Purpose
To assess the comparative efficacy of glucose-lowering drugs on liver steatosis as assessed by means of magnetic resonance imaging (MRI) in patients with T2D.
Methods
We searched several databases and grey literature sources. Eligible trials had at least 12 weeks of intervention, included patients with T2D, and assessed the efficacy of glucose-lowering drugs as monotherapies. The primary outcome of interest was absolute reduction in liver fat content (LFC), assessed by means of MRI. Secondary efficacy outcomes were reduction in visceral and subcutaneous adipose tissue. We performed random effects frequentist network meta-analyses to estimate mean differences (MDs) with 95% confidence intervals (CIs). We ranked treatments based on P-scores.
Results
We included 29 trials with 1906 patients. Sodium-glucose cotransporter-2 (SGLT-2) inhibitors (P-score 0.84) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) (0.71) were the most efficacious in terms of liver fat content reduction. Among individual agents, empagliflozin was the most efficacious (0.86) and superior to pioglitazone (MD -5.7, 95% CI -11.2 to -0.3) (very low confidence). GLP-1 RAs had also the most favorable effects on visceral and subcutaneous adipose tissue.
Conclusions
GLP-1 RAs and SGLT-2 inhibitors seem to be the most efficacious glucose-lowering drugs for liver steatosis in patients with T2D. Assessment of their efficacy on NAFLD in patients irrespective of presence of T2D is encouraged.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is the most common hepatic disorder worldwide [1, 2]. It encompasses a wide spectrum of liver disease ranging from simple steatosis to nonalcoholic steatohepatitis (NASH), and ultimately liver cirrhosis [3]. Owing to their common pathophysiologic background, type 2 diabetes mellitus (T2D) and NAFLD are two closely related conditions that often co-exist [4]. The prevalence of NAFLD in patients with T2D is approximately 70% [5]. Furthermore, T2D is considered an important driver of NAFLD progression. Therefore, early recognition and management of NAFLD in patients with T2D is of major importance.
Liver biopsy is currently considered the reference standard for NAFLD diagnosis [3, 4]. Moreover, the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) guidelines highlight the use of histological endpoints for conditional drug approval [6]. However, liver biopsy is an invasive procedure that may lead to severe complications, while it is impractical when it comes to patients’ follow-up. Moreover, its accuracy is undermined by sampling error and significant inter- and intra-observer variability concerning interpretation of the results [7]. As a result, novel imaging techniques are emerging as alternatives to liver biopsy for treatment response evaluation in patients with NAFLD. Among available modalities, magnetic resonance imaging (MRI)-derived proton density fat fraction (MRI-PDFF) is regarded as the most accurate for the assessment of liver fat content (LFC) [8]. Excessive fat accumulation can lead to liver necroinflammation and NASH progression. Recent meta-analyses support an association between a ≥ 30% relative decline in MRI-PDFF and histologic response in NAFLD [9, 10]. Consequently, the number of randomized controlled trials (RCTs) that use MRI techniques as an endpoint is greatly increasing.
Lifestyle modifications are the cornerstone for the management of NAFLD [3,4,5]. Up until recently, pioglitazone was the only glucose-lowering drug available for the management of NAFLD in patients with T2D [4]. Emerging evidence highlights the potentially beneficial role of other glucose-lowering drugs, including sodium-glucose cotransporter-2 inhibitors (SGLT-2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) in the management of NAFLD in the context of T2D [5, 11,12,13].
Given the increase of available medication options and the lack of head-to-head comparisons, we decided to perform a network meta-analysis in order to assess the comparative efficacy of available glucose-lowering drugs on liver steatosis in patients with T2D focusing on MRI-derived metrics. Previously published meta-analyses have addressed the efficacy of these agents in histological endpoints.
Materials and methods
The protocol for this systematic review and network meta-analysis has been registered in PROSPERO (CRD42022381704). We report our systematic review and network meta-analysis in line with the PRISMA Extension Statement for Reporting Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions (Table S1) [14].
Eligibility criteria
We included RCTs among adult patients with T2D that reported data on at least one outcome of interest and assessed glucose-lowering drugs currently approved by the FDA and/or EMA for the management of T2D. Eligible trials had a duration of treatment of at least 12 weeks and assessed the efficacy of drug monotherapies. Trials assessing agents that are not used in clinical practice, are no longer available, or have been withdrawn were not eligible for inclusion. Similarly, trials assessing non-pharmacologic interventions were excluded.
Literature search
We searched Medline, Embase, and the Cochrane Register of Controlled Trials (CENTRAL) up to July 2022 without restrictions. We updated our search strategy up to June 2023 in order to include recently published RCTs. Our search strategy comprised free text terms and medical subject headings describing T2D, eligible interventions, and primary outcome of interest (Table S2). Moreover, ClinicalTrials.gov and European Union Drug Regulating Authorities Clinical Trials Database (EudraCT) registries were searched up to September 2022 for additional completed trials with available results. Furthermore, we searched conference proceedings of the American Association for the Study of Liver Diseases, the American Diabetes Association, the European Association for the Study of the Liver, and the European Association for the Study of Diabetes from 2016 to 2022.
Study selection
Records from the electronic databases were imported into a literature review software (DistillerSR. Version 2.35). After duplicate removal, two reviewers working independently assessed record eligibility firstly at title and abstract level and subsequently in full text. Disagreements were arbitrated by a senior reviewer.
Data extraction
Two independent reviewers performed data extraction using a predesigned form. Multiple reports for the same trial were collated into a single entry based on the trial’s registration number, title, and baseline characteristics. For trials assessing multiple eligible doses for a given agent, we combined data from approved doses into a single intervention group [15]. In the case of several time points, we extracted data for the longest duration of intervention for each outcome. Data extraction items included trial characteristics, participants’ baseline characteristics, and outcome data. When needed, we imputed data using appropriate methodology [16, 17]. The primary outcome of interest was the absolute change from baseline in liver fat content (LFC) measured by means of MRI [MRI-PDFF or MR-spectroscopy (MRS)]. Both imaging techniques measure LFC as a percentage through the fat and water signals acquired during a magnetic resonance examination [18]. Secondary outcomes of interest were change from baseline in visceral adipose tissue (VAT), change from baseline in subcutaneous adipose tissue (SAT), and change from baseline in VAT/SAT ratio. Both VAT and SAT were measured in square centimeters (cm2) by means of MRI.
Risk of bias assessment
Risk of bias assessment was performed for all outcomes of interest by two independent reviewers with the revised Cochrane Risk of Bias tool (RoB) 2.0, assessing the following domains: randomization, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of reported results [19]. A trial was deemed at low risk of bias if all domains were at low risk. Trials were deemed at high risk of bias if at least one domain was at high risk or at least three domains aroused certain concerns. In any other case, a trial was considered to raise some concerns of bias.
Transitivity assessment
Conducting a network meta-analysis entails the transitivity assumption among eligible comparisons [20]. We evaluated transitivity by taking into consideration the distribution of major effect modifiers across pairwise comparisons, including diabetes duration and baseline hemoglobin A1C, serum lipids, body mass index (BMI), and LFC.
Data synthesis and analysis
We performed random effects, pairwise meta-analysis for each direct comparison with at least two trials. Subsequently, we performed frequentist random effects network meta-analysis and calculated mean differences (MDs) and 95% confidence intervals (CIs) for all outcomes of interest, assuming a common heterogeneity parameter across eligible comparisons [21, 22]. We ranked treatments by means of P-scores [23]. We evaluated statistical heterogeneity in the entire network based on the magnitude of the heterogeneity variance parameter (τ2), which derived from the network meta-analysis model. For our outcomes, we compared the estimated τ2 values with their expected values, as described by Turner et al.[24] We assessed inconsistency both locally with the side-splitting method and globally with the design-by-treatment model [25, 26].
For the primary outcome, eligible interventions were analyzed both as drug classes and as individual agents. For secondary outcomes and for all additional analysis, eligible interventions were analyzed as drug classes. We performed sensitivity analysis of trials with drug naïve or metformin monotherapy treated patients and trials that recruited patients with T2D and NAFLD at baseline. Moreover, we conducted sensitivity analyses including only trials at low RoB and trials where imputation methods were not performed for missing measures of dispersion. For all analyses, we used RevMan 5.4 and R statistical software.
Certainty of evidence
We assessed the confidence of effect estimates for our primary outcome with the CINeMA (Confidence In the results from Network Meta-Analysis) methodological approach and web application. We took into consideration the following domains: within-study bias, across-study bias, indirectness, imprecision, heterogeneity, and incoherence [27, 28].
Results
Overview of trials
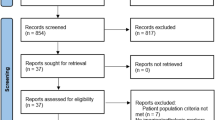
The study selection process is depicted in Fig. S1. After duplicate removal, we screened 2629 records and included 49 records for 29 RCTs with 1906 patients [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57]. Trial and participant baseline characteristics are presented in Table S3. Overall, eligible RCTs assessed 14 interventions from eight different drug classes (DPP-4 inhibitors, GLP-1 RAs, GIP/GLP-1 RAs, basal insulins, metformin, pioglitazone, SGLT-2i, and sulphonylureas). Most trials (n = 21) were funded by the pharmaceutical industry. Sixteen trials [30,31,32,33,34, 36,37,38, 40, 41, 44, 45, 47, 50, 51, 57] with 943 patients were placebo-controlled, whereas two trials compared active interventions to standard of care [55, 56]. Three trials with 467 patients were multi-arm [35, 36, 52]. The majority of the trials were either double or single blinded. Most trials (n = 20) had a duration of intervention greater than or equal to 24 weeks. Sample size ranged from 12 to 296 patients.
Approximately 60% of the overall population were male (n = 1143). Patients’ mean age ranged from 43.1 to 65.6 years. Fifty-two percent of all patients were on a structured diet program or received dietary counseling, while 46% were on a structured exercise program or received some form of exercise counseling. Patients’ mean BMI at baseline ranged from 23.9 to 41.6 kg/m2. More than half of the included trials (n = 16) included mainly obese patients (BMI > 30.0 kg/m2). Mean HbA1c at baseline ranged from 6.3% to 9.1%. A total of 665 patients (34.8%) were either drug naïve or treated solely with metformin at enrolment. Among the remaining patients, the background glucose-lowering treatment varied, mainly comprising metformin with at least one more glucose-lowering agent.
Risk of bias assessment
Risk of bias assessment for all outcomes is presented in Tables S4-S7. For the primary outcome, eight trials were at low risk and two trials to have some concerns of bias due to inadequate description of the randomization process and missing outcome data. The remaining trials were judged at high risk of bias because of suboptimal reporting of the analysis process and missing outcome data.
Transitivity assessment
The available number of trials for each comparison was limited and, consequently, a comprehensive evaluation of transitivity was not possible. In order to assess the transitivity assumption, we compared potential effect modifiers across included trials. Patients’ mean duration of diabetes at enrolment was at least 3.0 years in all trials except one, which included solely patients with newly diagnosed T2D. Mean HbA1c at baseline was > 7.0% (53 mmol/mol) in the majority of trials, suggesting suboptimal glycemic control among patients. Moreover, most trials included middle-aged patients with comparable serum lipid profiles at enrolment. Across all trials, the median LFC at baseline was 16.15% (interquartile range, 13.1% to 21.6%), suggesting that the majority of patients at baseline had NAFLD.
Pairwise meta-analyses
Results from pairwise meta-analyses are presented in Table S8. Sodium-glucose cotransporter-2 inhibitors (MD -3.06%, 95% CI -4.74 to -1.37) and GLP-1 RAs (-2.38%, -4.40 to -0.35) reduced LFC compared with placebo. Glucagon-like peptide-1 receptor agonists were superior to placebo in VAT (-23.4 cm2, -41.4 to -5.3) and SAT (-27.3 cm2, -38.0 to -16.7) reduction.
Network meta-analyses
Liver fat content
Network plots for change in LFC in terms of drug classes and individual agents are presented in Fig. 1 and Fig. 2, respectively. At drug class level, SGLT-2i (-3.27%, -4.99 to -1.56) and GLP-1 RAs (-2.22%, -3.87 to -0.57) reduced LFC compared to placebo. In comparisons between drug classes, GLP-1 RAs, SGLT-2i, and GIP/GLP-1 RAs were more efficacious compared to metformin, while compared to each other all three drug classes were equally efficacious (Table 1). Based on P-scores, GIP/GLP-1 RAs were ranked as the most efficacious treatment (P-score 0.87), followed by SGLT-2i (0.84) and GLP-1 RAs (0.71) (Table S9).

Network for change in liver fat content; drug classes. Each circle indicates a treatment node. Lines connecting two nodes represent direct comparisons between two treatments. The size of the nodes is proportional to the number of trials evaluating each treatment. The thickness of the lines is proportional to the number of trials directly comparing connected treatments. DPP-4 = dipeptidyl peptidase-4. GLP-1 = glucagon-like peptide-1. GIP = glucose-dependent insulinotropic polypeptide. SGLT-2 = sodium-glucose cotransporter-2. RA = receptor agonist

Network for change in liver fat content; agents. Each circle indicates a treatment node. Lines connecting two nodes represent direct comparisons between two treatments. The size of the nodes is proportional to the number of trials evaluating each treatment. The thickness of the lines is proportional to the number of trials directly comparing connected treatments
Among individual agents, only empagliflozin (-4.35%, -6.74 to -1.96) reduced LFC compared with placebo. Empagliflozin was also superior to pioglitazone (-5.78%, -11.21 to -0.34), metformin, insulin glargine, and sitagliptin (Table S10). There was no difference between canagliflozin, dapagliflozin, and empagliflozin. Empagliflozin was placed at the top of the hierarchy of competing treatments (0.86), followed by exenatide (0.77) and dulaglutide (0.73) (Table S11).
Visceral and subcutaneous adipose tissue
Network plots of trials assessing VAT and SAT reduction are presented in Fig. S2-S3. Compared to placebo, GLP-1 RAs reduced visceral (-25.0 cm2, -39.6 to -10.3) and subcutaneous ( -30.9 cm2, -44.6 to -17.2) adipose tissue. Glucagon-like peptide-1 receptor agonists and SGLT-2i were equally efficacious for both outcomes (Tables S12-S13). GLP-1 RAs were ranked as the best option for both outcomes (Tables S14-S15).
Data synthesis for VAT/SAT ratio was not feasible due to the limited number of trials reporting relevant data.
Additional analyses
All additional analyses were performed for the outcome of LFC reduction and for comparisons among drug classes. In sensitivity analysis of trials that recruited solely drug naïve or metformin monotherapy treated patients, only GLP-1 RAs reduced LFC compared with placebo (-4.54%, -7.56 to -1.51) (Table S16). Sensitivity analyses of trials that recruited patients with T2D and NAFLD and of trials at low risk of bias yielded similar results to our main analysis (Tables S17-S18). Results from additional analyses are presented in the supplementary appendix.
Heterogeneity and inconsistency and publication bias
For most networks, there was increased heterogeneity (Table S20). There was no evidence of inconsistency under the assumption of a full design-by-treatment interaction random effects model except for the VAT network (Table S21). Based on comparison-adjusted funnel plots, there was no evidence of small study effect bias.
Certainty of evidence
The confidence in estimates for reduction of LFC was low to very low across comparisons. This was mainly attributed to within-study bias and imprecision (Tables S22-S23).
Discussion
Summary of findings
The aim of this systematic review and network meta-analysis was to assess the comparative efficacy of glucose-lowering drugs on liver steatosis as assessed by means of MRI in patients with T2D. In terms of drug classes, GLP-1 RAs and SGLT-2 inhibitors were the most efficacious in reducing LFC based on MRI. Empagliflozin was ranked as the most efficacious glucose-lowering agent, followed by exenatide and dulaglutide. Tirzepatide, a novel agent recently licensed for the treatment of T2D, seems promising; nevertheless, results derive from a single trial and therefore firm statements regarding its effect on liver steatosis are rather challenging. Pioglitazone, a glucose-lowering agent with proven histologic efficacy in biopsy-confirmed NASH, performed poorly. The confidence in our estimates was low to very low. In terms of adipose tissue, either visceral or subcutaneous, GLP-1RAs were the most efficacious options.
Our results are generally in line with recently published guidelines supporting the use of GLP1-RAs and SGLT-2i in patients with T2D and NAFLD [5, 58]. Weight reduction and management of cardiovascular risk are the cornerstone for the management of NAFLD. Glucagon-like peptide-1 receptor agonists and SGLT-2i already have an established efficacy for weight reduction and management of aspects of metabolic syndrome [59, 60]. Our analysis corroborates findings from previous meta-analyses regarding the efficacy of GLP-1 RAs and SGLT-2 inhibitors on liver steatosis, as assessed by means of MRI [61, 62]. Given the fact that hepatic lipotoxocity is a major risk factor of fibrosis progression in NAFLD, our findings suggest that certain glucose-lowering drug classes and agents have the potential to reduce liver steatosis and possibly halt fibrosis in patients with T2D [8, 63]. Among existing glucose-lowering agents, pioglitazone is the most efficacious for NASH amelioration as assessed by means of liver biopsy. Discrepancies regarding the efficacy of pioglitazone on liver steatosis are probably attributable to the fact that we did not assess histological outcomes, for which the agent has proven efficacy, and that our population of interest comprised patients with T2D irrespective of the presence of NAFLD at baseline [4, 63].
In line with our findings, other meta-analyses highlight the efficacy of GLP-1RAs with regard to VAT and SAT reduction in patients with T2D [64]. Based on the ‘adipose tissue overflow’ hypothesis, fat storage begins primarily in the subcutaneous region. When the subcutaneous region exceeds its capacity, fat accumulates in deeper regions such as the viscera or liver [65]. These deeper fat deposits are more pathogenic, contributing to the inflammatory pathway related to NAFLD [66].
Strengths and limitations
In comparison to other meta-analyses [63, 67, 68], we focused on MRI-derived metrics based on the need for noninvasive assessment of liver steatosis. Glucose-lowering agents are currently at the epicenter of the NASH clinical trial landscape. Following the limited number of clinical trials comparing active interventions, we provide preliminary comparative efficacy estimates among promising agents and drug classes. Furthermore, we assessed both interclass and intraclass differences among treatments and synthesized available evidence using robust methodology.
Certain limitations should be acknowledged. Most trials were at high risk of bias and the confidence in our estimates among comparisons was low to very low. We did not evaluate a variety of pertinent clinically important outcomes (i.e., histological, biochemical, and safety related outcomes). On the other hand, histological and biochemical parameters as well as the safety of glucose-lowering agents have been addressed in previous meta-analyses [60,61,62,63]. Focusing on the presence of T2D as an inclusion criterion meant that we had to exclude RCTs that assessed the efficacy of glucose-lowering agents on liver steatosis in patients with stablished NAFLD, regardless of the presence of T2D [8, 69]. Results from these trials highlight the beneficial role of semaglutide in the reduction of intrahepatic fat, although the effects on fibrosis were not significant. In addition, heterogeneity is always a concern in evidence synthesis, especially in the context of network meta-analysis, thus limiting the validity of results [20]. Moreover, individual agent analysis was based on a limited number of trials per comparison; thus, results should be interpreted with caution. Furthermore, although treatment ranking by means of either SUCRA or p scores seems attractive, it can sometimes be misleading. Estimates of ranking probabilities are closely related to network structure and number of trials per comparison. The same number of trials per comparison can lead to biased ranking estimates for a given network [70]. In our analysis, the GIP/GLP1-RA tirzepatide has a p score of 0.87, suggesting high probability of being the best for the reduction of LFC among drug classes, although it failed to outperform placebo. This phenomenon can be partially addressed by taking into consideration the certainty of evidence when interpreting synthesis results.
Implication for practice and research
Our results provide supportive evidence on the use of GLP-1RAs and SGLT-2i as suggested by current practice guidelines [5, 58]. Among SGLT-2i, our results support the use of empagliflozin alongside semaglutide in patients with T2D and liver steatosis. Tirzepatide, a novel GIP/GLP1-RA, seems promising; however, its efficacy in terms of steatosis management remains to be established. As a result, future research should focus on the assessment of the above intervention in the context of NAFLD irrespective of the presence of diabetes. Furthermore, the efficacy of these interventions in patients with metabolic syndrome but without diabetes remains unclear. Whether glucose-lowering agents exert their beneficial effects on liver steatosis through body weight reduction is still a matter of controversy. In our study, drug classes with proven benefit in weight reduction were also the most efficacious in reducing liver steatosis, whereas treatment with pioglitazone, which has proven efficacy in histologic improvement of NASH but is also associated with an increased risk for weight gain, performed poorly. Further research should shed light on whether counterbalancing pioglitazone-induced weight gain by combination therapy with agents that induce weight loss could maximize benefits regarding liver steatosis. Nevertheless, several trials have demonstrated the beneficial effect of pioglitazone on NAFLD irrespective of the presence of diabetes [71, 72]. Moreover, the combined efficacy of GLP-1RAs and SGLT-2i in NAFLD remains unclear.
Biopsy is the reference standard for the diagnosis of NAFLD. However, it is an invasive procedure with inherent limitations that hamper the follow-up of patients in trials. Undoubtedly, noninvasive techniques are the future of research in the field of NAFLD. Among existing noninvasive candidates, MRI seems the most promising. Consequently, MRI-related outcomes should be taken into consideration in future trials. A more holistic approach including histological, MRI-related, biochemical, anthropometric, and safety outcomes could provide deeper insight.
Conclusion
Our results suggest that GLP-1 RAs and SGLT-2 inhibitors are the most efficacious glucose-lowering drug classes for amelioration of steatosis assessed by MRI-derived metrics in patients with T2D. Excluding semaglutide, empagliflozin is probably the best option among the available glucose-lowering agents. Conclusions must be interpreted with caution, since confidence in our estimates is very low, and, as such, large-scale, high-quality RCTs with MRI-related outcomes are needed.
Data Availability
Available on reasonable request from Dr Malandris.
References
Burra P, Becchetti C, Germani G (2020) NAFLD and liver transplantation: Disease burden, current management and future challenges. JHEP Rep 2:100192. https://doi.org/10.1016/j.jhepr.2020.100192
Riazi K, Azhari H, Charette JH, Underwood FE, King JA, Afshar EE et al (2022) The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 7:851–861. https://doi.org/10.1016/s2468-1253(22)00165-0
EASL-EASD-EASO (2016) Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 64:1388–402. https://doi.org/10.1016/j.jhep.2015.11.004
Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M et al (2018) The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 67:328–357. https://doi.org/10.1002/hep.29367
Cusi K, Isaacs S, Barb D, Basu R, Caprio S, Garvey WT et al (2022) American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract 28:528–562. https://doi.org/10.1016/j.eprac.2022.03.010
Harrison SA, Allen AM, Dubourg J, Noureddin M, Alkhouri N (2023) Challenges and opportunities in NASH drug development. Nat Med 29:562–573. https://doi.org/10.1038/s41591-023-02242-6
Caussy C, Alquiraish MH, Nguyen P, Hernandez C, Cepin S, Fortney LE et al (2018) Optimal threshold of controlled attenuation parameter with MRI-PDFF as the gold standard for the detection of hepatic steatosis. Hepatology 67:1348–1359. https://doi.org/10.1002/hep.29639
Flint A, Andersen G, Hockings P, Johansson L, Morsing A, Sundby Palle M et al (2021) Randomised clinical trial: semaglutide versus placebo reduced liver steatosis but not liver stiffness in subjects with non-alcoholic fatty liver disease assessed by magnetic resonance imaging. Aliment Pharmacol Ther 54:1150–1161. https://doi.org/10.1111/apt.16608
Tamaki N, Munaganuru N, Jung J, Yonan AQ, Loomba RR, Bettencourt R et al (2022) Clinical utility of 30% relative decline in MRI-PDFF in predicting fibrosis regression in non-alcoholic fatty liver disease. Gut 71:983–990. https://doi.org/10.1136/gutjnl-2021-324264
Stine JG, Munaganuru N, Barnard A, Wang JL, Kaulback K, Argo CK et al (2021) Change in MRI-PDFF and Histologic Response in Patients With Nonalcoholic Steatohepatitis: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol 19:2274–83.e5. https://doi.org/10.1016/j.cgh.2020.08.061
Ghosal S, Datta D, Sinha B (2021) A meta-analysis of the effects of glucagon-like-peptide 1 receptor agonist (GLP1-RA) in nonalcoholic fatty liver disease (NAFLD) with type 2 diabetes (T2D). Sci Rep 11:22063. https://doi.org/10.1038/s41598-021-01663-y
Mantovani A, Byrne CD, Targher G (2022) Efficacy of peroxisome proliferator-activated receptor agonists, glucagon-like peptide-1 receptor agonists, or sodium-glucose cotransporter-2 inhibitors for treatment of non-alcoholic fatty liver disease: a systematic review. Lancet Gastroenterol Hepatol 7:367–378. https://doi.org/10.1016/s2468-1253(21)00261-2
Shao SC, Kuo LT, Chien RN, Hung MJ, Lai EC (2020) SGLT2 inhibitors in patients with type 2 diabetes with non-alcoholic fatty liver diseases: an umbrella review of systematic reviews. BMJ Open Diabetes Res Care. 8. https://doi.org/10.1136/bmjdrc-2020-001956
Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C et al (2015) The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 162:777–784. https://doi.org/10.7326/m14-2385
Rücker G, Cates CJ, Schwarzer G (2017) Methods for including information from multi-arm trials in pairwise meta-analysis. Res Synth Methods 8:392–403. https://doi.org/10.1002/jrsm.1058
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors) (2022) Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane. Available from. www.training.cochrane.org/handbook.
Weir CJ, Butcher I, Assi V, Lewis SC, Murray GD, Langhorne P et al (2018) Dealing with missing standard deviation and mean values in meta-analysis of continuous outcomes: a systematic review. BMC Med Res Methodol 18:25. https://doi.org/10.1186/s12874-018-0483-0
Caussy C, Johansson L (2020) Magnetic resonance-based biomarkers in nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Endocrinol Diabetes Metab 3:e00134. https://doi.org/10.1002/edm2.134
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I et al (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj. 366:l4898. https://doi.org/10.1136/bmj.l4898
Cipriani A, Higgins JP, Geddes JR, Salanti G (2013) Conceptual and technical challenges in network meta-analysis. Ann Intern Med 159:130–137. https://doi.org/10.7326/0003-4819-159-2-201307160-00008
Rücker G, Schwarzer G (2014) Reduce dimension or reduce weights? Comparing two approaches to multi-arm studies in network meta-analysis. Stat Med 33:4353–4369. https://doi.org/10.1002/sim.6236
Rücker G (2012) Network meta-analysis, electrical networks and graph theory. Res Synth Methods 3:312–324. https://doi.org/10.1002/jrsm.1058
Rücker G, Schwarzer G (2015) Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol 15:58. https://doi.org/10.1186/s12874-015-0060-8
Turner RM, Davey J, Clarke MJ, Thompson SG, Higgins JP (2012) Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int J Epidemiol 41:818–827. https://doi.org/10.1093/ije/dys041
Higgins JP, Jackson D, Barrett JK, Lu G, Ades AE, White IR (2012) Consistency and inconsistency in network meta-analysis: concepts and models for multi-arm studies. Res Synth Methods 3:98–110. https://doi.org/10.1002/jrsm.1044
Dias S, Welton NJ, Caldwell DM, Ades AE (2010) Checking consistency in mixed treatment comparison meta-analysis. Stat Med 29:932–944. https://doi.org/10.1002/sim.3767
Nikolakopoulou A, Higgins JPT, Papakonstantinou T, Chaimani A, Del Giovane C, Egger M et al (2020) CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med 17:e1003082. https://doi.org/10.1371/journal.pmed.1003082
Papakonstantinou T, Nikolakopoulou A, Higgins JPT, Egger M, Salanti G (2020) CINeMA: Software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst Rev 16:e1080
Bi Y, Zhang B, Xu W, Yang H, Feng W, Li C et al (2014) Effects of exenatide, insulin, and pioglitazone on liver fat content and body fat distributions in drug-naive subjects with type 2 diabetes. Acta Diabetol 51:865–873. https://doi.org/10.1007/s00592-014-0638-3
Bizino MB, Jazet IM, de Heer P, van Eyk HJ, Dekkers IA, Rensen PCN et al (2020) Placebo-controlled randomised trial with liraglutide on magnetic resonance endpoints in individuals with type 2 diabetes: a pre-specified secondary study on ectopic fat accumulation. Diabetologia 63:65–74. https://doi.org/10.1007/s00125-019-05021-6
Bolinder J, Ljunggren Ö, Kullberg J, Johansson L, Wilding J, Langkilde AM et al (2012) Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J Clin Endocrinol Metab 97:1020–1031. https://doi.org/10.1210/jc.2011-2260
Cusi K, Bril F, Barb D, Polidori D, Sha S, Ghosh A et al (2019) Effect of canagliflozin treatment on hepatic triglyceride content and glucose metabolism in patients with type 2 diabetes. Diabetes Obes Metab 21:812–821. https://doi.org/10.1111/dom.13584
Eriksson JW, Lundkvist P, Jansson PA, Johansson L, Kvarnström M, Moris L et al (2018) Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: a double-blind randomised placebo-controlled study. Diabetologia 61:1923–1934. https://doi.org/10.1007/s00125-018-4675-2
Gaborit B, Ancel P, Abdullah AE, Maurice F, Abdesselam I, Calen A et al (2021) Effect of empagliflozin on ectopic fat stores and myocardial energetics in type 2 diabetes: the EMPACEF study. Cardiovasc Diabetol 20:57. https://doi.org/10.1186/s12933-021-01237-2
Gastaldelli A, Cusi K, Fernández Landó L, Bray R, Brouwers B, Rodríguez Á (2022) Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes Endocrinol 10:393–406. https://doi.org/10.1016/s2213-8587(22)00070-5
Guo W, Tian W, Lin L, Xu X (2020) Liraglutide or insulin glargine treatments improves hepatic fat in obese patients with type 2 diabetes and nonalcoholic fatty liver disease in twenty-six weeks: A randomized placebo-controlled trial. Diabetes Res Clin Pract 170:108487. https://doi.org/10.1016/j.diabres.2020.108487
Guzman CB, Zhang XM, Liu R, Regev A, Shankar S, Garhyan P et al (2017) Treatment with LY2409021, a glucagon receptor antagonist, increases liver fat in patients with type 2 diabetes. Diabetes Obes Metab 19:1521–1528. https://doi.org/10.1111/dom.12958
Harreiter J, Just I, Leutner M, Bastian M, Brath H, Schelkshorn C et al (2021) Combined exenatide and dapagliflozin has no additive effects on reduction of hepatocellular lipids despite better glycaemic control in patients with type 2 diabetes mellitus treated with metformin: EXENDA, a 24-week, prospective, randomized, placebo-controlled pilot trial. Diabetes Obes Metab 23:1129–1139. https://doi.org/10.1111/dom.14319
Jonker JT, Wang Y, de Haan W, Diamant M, Rijzewijk LJ, van der Meer RW et al (2010) Pioglitazone decreases plasma cholesteryl ester transfer protein mass, associated with a decrease in hepatic triglyceride content, in patients with type 2 diabetes. Diabetes Care 33:1625–1628. https://doi.org/10.2337/dc09-1935
Joy TR, McKenzie CA, Tirona RG, Summers K, Seney S, Chakrabarti S et al (2017) Sitagliptin in patients with non-alcoholic steatohepatitis: A randomized, placebo-controlled trial. World J Gastroenterol 23:141–150. https://doi.org/10.3748/wjg.v23.i1.141
Kahl S, Gancheva S, Straßburger K, Herder C, Machann J, Katsuyama H et al (2020) Empagliflozin Effectively Lowers Liver Fat Content in Well-Controlled Type 2 Diabetes: A Randomized, Double-Blind, Phase 4. Placebo-Controlled Trial Diabetes Care 43:298–305. https://doi.org/10.2337/dc19-0641
Kato H, Nagai Y, Ohta A, Ten** A, Nakamura Y, Tsukiyama H et al (2015) Effect of sitagliptin on intrahepatic lipid content and body fat in patients with type 2 diabetes. Diabetes Res Clin Pract 109:199–205. https://doi.org/10.1016/j.diabres.2015.04.008
Liu L, Yan H, **a M, Zhao L, Lv M, Zhao N et al (2020) Efficacy of exenatide and insulin glargine on nonalcoholic fatty liver disease in patients with type 2 diabetes. Diabetes Metab Res Rev 36:e3292. https://doi.org/10.1002/dmrr.3292
Macauley M, Hollingsworth KG, Smith FE, Thelwall PE, Al-Mrabeh A, Schweizer A et al (2015) Effect of vildagliptin on hepatic steatosis. J Clin Endocrinol Metab 100:1578–1585. https://doi.org/10.1210/jc.2014-3794
Matikainen N, Söderlund S, Björnson E, Pietiläinen K, Hakkarainen A, Lundbom N et al (2019) Liraglutide treatment improves postprandial lipid metabolism and cardiometabolic risk factors in humans with adequately controlled type 2 diabetes: A single-centre randomized controlled study. Diabetes Obes Metab 21:84–94. https://doi.org/10.1111/dom.13487
Ridderstråle M, Andersen KR, Zeller C, Kim G, Woerle HJ, Broedl UC (2014) Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: a 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol 2:691–700. https://doi.org/10.1016/s2213-8587(14)70120-2
Sathyanarayana P, Jogi M, Muthupillai R, Krishnamurthy R, Samson SL, Bajaj M (2011) Effects of combined exenatide and pioglitazone therapy on hepatic fat content in type 2 diabetes. Obesity (Silver Spring) 19:2310–2315. https://doi.org/10.1038/oby.2011.152
Smits MM, Tonneijck L, Muskiet MH, Kramer MH, Pouwels PJ, Pieters-van den Bos IC et al (2016) Twelve week liraglutide or sitagliptin does not affect hepatic fat in type 2 diabetes: a randomised placebo-controlled trial. Diabetologia 59:2588–2593. https://doi.org/10.1007/s00125-016-4100-7
Tang A, Rabasa-Lhoret R, Castel H, Wartelle-Bladou C, Gilbert G, Massicotte-Tisluck K et al (2015) Effects of Insulin Glargine and Liraglutide Therapy on Liver Fat as Measured by Magnetic Resonance in Patients With Type 2 Diabetes: A Randomized Trial. Diabetes Care 38:1339–1346. https://doi.org/10.2337/dc14-2548
van Eyk HJ, Paiman EHM, Bizino MB, de Heer P, Geelhoed-Duijvestijn PH, Kharagjitsingh AV et al (2019) A double-blind, placebo-controlled, randomised trial to assess the effect of liraglutide on ectopic fat accumulation in South Asian type 2 diabetes patients. Cardiovasc Diabetol 18:87. https://doi.org/10.1186/s12933-019-0890-5
Vanderheiden A, Harrison LB, Warshauer JT, Adams-Huet B, Li X, Yuan Q et al (2016) Mechanisms of Action of Liraglutide in Patients With Type 2 Diabetes Treated With High-Dose Insulin. J Clin Endocrinol Metab 101:1798–1806. https://doi.org/10.1210/jc.2015-3906
Yan J, Yao B, Kuang H, Yang X, Huang Q, Hong T et al (2019) Liraglutide, Sitagliptin, and Insulin Glargine Added to Metformin: The Effect on Body Weight and Intrahepatic Lipid in Patients With Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease. Hepatology 69:2414–2426. https://doi.org/10.1002/hep.30320
Zhang LY, Qu XN, Sun ZY, Zhang Y (2020) Effect of liraglutide therapy on serum fetuin A in patients with type 2 diabetes and non-alcoholic fatty liver disease. Clin Res Hepatol Gastroenterol 44:674–680. https://doi.org/10.1016/j.clinre.2020.01.007
Hiruma S, Shigiyama F, Kumashiro N (2023) Empagliflozin versus sitagliptin for ameliorating intrahepatic lipid content and tissue-specific insulin sensitivity in patients with early-stage type 2 diabetes with non-alcoholic fatty liver disease: A prospective randomized study. Diabetes Obes Metab 25:1576–1588. https://doi.org/10.1111/dom.15006
Kuchay MS, Krishan S, Mishra SK, Farooqui KJ, Singh MK, Wasir JS et al (2018) Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 41:1801–1808. https://doi.org/10.2337/dc18-0165
Kuchay MS, Krishan S, Mishra SK, Choudhary NS, Singh MK, Wasir JS et al (2020) Effect of dulaglutide on liver fat in patients with type 2 diabetes and NAFLD: randomised controlled trial (D-LIFT trial). Diabetologia 63:2434–2445. https://doi.org/10.1007/s00125-020-05265-7
Elhini SH, Wahsh EA, Elberry AA, El Ameen NF, Abdelfadil Saedii A, Refaie SM, et al (2022) The Impact of an SGLT2 Inhibitor versus Ursodeoxycholic Acid on Liver Steatosis in Diabetic Patients. Pharmaceuticals (Basel). 15. https://doi.org/10.3390/ph15121516
Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D et al (2023) AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 77:1797–1835. https://doi.org/10.1097/hep.0000000000000323
Tsapas A, Karagiannis T, Kakotrichi P, Avgerinos I, Mantsiou C, Tousinas G et al (2021) Comparative efficacy of glucose-lowering medications on body weight and blood pressure in patients with type 2 diabetes: A systematic review and network meta-analysis. Diabetes Obes Metab 23:2116–2124. https://doi.org/10.1111/dom.14451
Tsapas A, Avgerinos I, Karagiannis T, Malandris K, Manolopoulos A, Andreadis P et al (2020) Comparative Effectiveness of Glucose-Lowering Drugs for Type 2 Diabetes: A Systematic Review and Network Meta-analysis. Ann Intern Med 173:278–286. https://doi.org/10.7326/m20-0864
Mantovani A, Petracca G, Csermely A, Beatrice G, Targher G (2020) Sodium-Glucose Cotransporter-2 Inhibitors for Treatment of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials. Metabolites. 11. https://doi.org/10.3390/metabo11010022
Mantovani A, Petracca G, Beatrice G, Csermely A, Lonardo A, Targher G (2021) Glucagon-Like Peptide-1 Receptor Agonists for Treatment of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: An Updated Meta-Analysis of Randomized Controlled Trials. Metabolites. 11. https://doi.org/10.3390/metabo11020073
Majzoub AM, Nayfeh T, Barnard A, Munaganuru N, Dave S, Singh S et al (2021) Systematic review with network meta-analysis: comparative efficacy of pharmacologic therapies for fibrosis improvement and resolution of NASH. Aliment Pharmacol Ther 54:880–889. https://doi.org/10.1111/apt.16583
Liu F, Yang Q, Zhang H, Zhang Y, Yang G, Ban B et al (2022) The effects of glucagon-like peptide-1 receptor agonists on adipose tissues in patients with type 2 diabetes: A meta-analysis of randomised controlled trials. PLoS One 17:e0270899. https://doi.org/10.1371/journal.pone.0270899
Iliodromiti S, McLaren J, Ghouri N, Miller MR, Dahlqvist Leinhard O, Linge J et al (2023) Liver, visceral and subcutaneous fat in men and women of South Asian and white European descent: a systematic review and meta-analysis of new and published data. Diabetologia 66:44–56. https://doi.org/10.1007/s00125-022-05803-5
Hanlon CL, Yuan L (2022) Nonalcoholic Fatty Liver Disease: The Role of Visceral Adipose Tissue. Clin Liver Dis (Hoboken) 19:106–110. https://doi.org/10.1002/cld.1183
Wei Q, Xu X, Guo L, Li J, Li L (2021) Effect of SGLT2 Inhibitors on Type 2 Diabetes Mellitus With Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials. Front Endocrinol (Lausanne) 12:635556. https://doi.org/10.3389/fendo.2021.635556
Luo Q, Wei R, Cai Y, Zhao Q, Liu Y, Liu WJ (2022) Efficacy of Off-Label Therapy for Non-alcoholic Fatty Liver Disease in Improving Non-invasive and Invasive Biomarkers: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Front Med (Lausanne) 9:793203. https://doi.org/10.3389/fmed.2022.793203
Newsome PN, Buchholtz K, Cusi K, Linder M, Okanoue T, Ratziu V et al (2020) A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N Engl J Med 384:1113–1124. https://doi.org/10.1056/NEJMoa2028395
Kibret T, Richer D, Beyene J (2014) Bias in identification of the best treatment in a Bayesian network meta-analysis for binary outcome: a simulation study. Clin Epidemiol 6:451–460. https://doi.org/10.2147/clep.S69660
Lavynenko O, Abdul-Ghani M, Alatrach M, Puckett C, Adams J, Abdelgani S et al (2022) Combination therapy with pioglitazone/exenatide/metformin reduces the prevalence of hepatic fibrosis and steatosis: The efficacy and durability of initial combination therapy for type 2 diabetes (EDICT). Diabetes Obes Metab 24:899–907. https://doi.org/10.1111/dom.14650
Della Pepa G, Russo M, Vitale M, Carli F, Vetrani C, Masulli M et al (2021) Pioglitazone even at low dosage improves NAFLD in type 2 diabetes: clinical and pathophysiological insights from a subgroup of the TOSCA.IT randomised trial. Diabetes Res Clin Pract 178:108984. https://doi.org/10.1016/j.diabres.2021.108984
Funding
Open access funding provided by HEAL-Link Greece. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KM, SP, PP, TK, EB, AL, ES, and AT conceived and designed the study. KM, SP, IA, TK, and TM conducted the literature search. KM, SP, PP, AL, TM, and EB carried out the study selection. KM, SP, PP, and AL extracted data. PP, IA, AL, and TM assessed methodological quality of included studies. IA, KM, TK, and SP did the statistical analyses. KM, SP, IA, ES, and TK prepared the first draft of the report, which was critically revised and approved by all authors.
Corresponding author
Ethics declarations
Conflicts of interest
A.T. has received research support from Boehringer Ingelheim. E.B. and E.S. have received research support from Novo Nordisk.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Malandris, K., Papandreou, S., Avgerinos, I. et al. Comparative efficacy of glucose-lowering drugs on liver steatosis as assessed by means of magnetic resonance imaging in patients with type 2 diabetes mellitus: systematic review and network meta-analysis. Hormones 22, 655–664 (2023). https://doi.org/10.1007/s42000-023-00493-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42000-023-00493-z