
Abstract
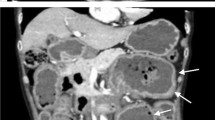
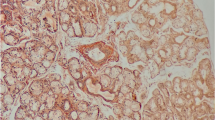
Secondary amyloidosis is a rare complication of chronic inflammatory diseases, such as collagen diseases, and is often difficult to treat. In addition, the gastrointestinal tract is frequently involved in amyloid deposition that often results in various disorders and symptoms. A 70-year-old woman was admitted to our hospital with refractory diarrhea and hypoalbuminemia. Abdominal computed tomography demonstrated extensive edematous wall thickening of the small intestine and colon. Video capsule endoscopy revealed multiple ulcerations with a white mossy appearance of the ileum. Double-balloon endoscopy showed severe circumferential ulcers in the entire ileum. Histological examination of ileum biopsy samples revealed severe amyloid deposition in the lamina propria and perivascular areas of the submucosa. The patient was diagnosed with gastrointestinal AA amyloidosis. The cause of AA amyloid deposition was presumed to be chronic pyelonephritis due to ureteral stones that had been left untreated for 35 years. After treatment with ureteral drainage and antibiotics, the patient’s symptoms and serological abnormalities improved dramatically. Here, we describe a case of severe gastrointestinal AA amyloidosis secondary to chronic pyelonephritis. Clinicians should thoroughly investigate the entire gastrointestinal tract in patients with refractory diarrhea and severe hypoalbuminemia considering the possibility of gastrointestinal amyloidosis.






Similar content being viewed by others

References
Choi JH, Ko BM, Kim C, et al. A case of localized amyloid light-chain amyloidosis in the small intestine. Intest Res. 2014;12:245–50.
Ebert EC, Nagar M. Gastrointestinal manifestations of amyloidosis. Am J Gastroenterol. 2008;103:776–87.
Naiki H, Sekijima Y, Ueda M, et al. Human amyloidosis, still intractable but becoming curable: the essential role of pathological diagnosis in the selection of type-specific therapeutics. Pathol Int. 2020;70:191–8.
Cowan AJ, Skinner M, Seldin DC, et al. Amyloidosis of the gastrointestinal tract: a 13-year, single-center, referral experience. Haematologica. 2013;98:141–6.
Shiratori Y, Fukuda K, Ikeya T, et al. Primary gastrointestinal amyloidosis with gastrointestinal hemorrhage and intestinal pseudo-obstruction: a report of a rare case. Clin J Gastroenterol. 2019;12:258–62.
Iida T, Yamano H, Nakase H. Systemic amyloidosis with gastrointestinal involvement: diagnosis from endoscopic and histological views. J Gastroenterol Hepatol. 2018;33:583–90.
Tada S, Iida M, Yao T, et al. Endoscopic features in amyloidosis of the small intestine: clinical and morphologic differences between chemical types of amyloid protein. Gastrointest Endosc. 1994;40:45–50.
Briggs GW. Amyloidosis. Ann Intern Med. 1961;55:943–57.
Gal R, Korzets A, Schwartz A, et al. Systemic distribution of beta 2-microglobulin-derived amyloidosis in patients who undergo long-term hemodialysis. Report of seven cases and review of the literature. Arch Pathol Lab Med. 1994;118:718–21.
Lachmann HJ, Goodman HJ, Gilbertson JA, et al. Natural history and outcome in systemic AA amyloidosis. N Engl J Med. 2007;356:2361–71.
Tsuchiya Y, Ubara Y, Suwabe T, et al. AA-amyloidosis in autosomal dominant polycystic kidney disease caused by chronic cyst infections lasting for 30 years. Intern Med. 2013;52:791–4.
Gillmore JD, Lovat LB, Persey MR, et al. Amyloid load and clinical outcome in AA amyloidosis in relation to circulating concentration of serum amyloid A protein. Lancet. 2001;358:24–9.
Nienhuis HL, Bijzet J, Hazenberg BP. The prevalence and management of systemic amyloidosis in western countries. Kidney Dis. 2016;2:10–9.
Acknowledgements
This research was partially supported by AMED under Grant Numbers JP21fk0210077, JP21fk0210047, JP21fk0210058.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human rights
All procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and its later amendments.
Informed consent
Informed consent was obtained from the patient included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tanaka, T., Naito, T., Midori, Y. et al. Gastrointestinal AA amyloidosis secondary to chronic pyelonephritis presenting with refractory diarrhea and severe hypoalbuminemia. Clin J Gastroenterol 14, 1642–1648 (2021). https://doi.org/10.1007/s12328-021-01508-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-021-01508-1