
Abstract
Introduction
Premenopausal women with hormone receptor positive (HR+) and human epidermal growth factor receptor-2-negative (HER2−) advanced breast cancer (aBC) often present with aggressive tumor types that lead to poor prognosis, high rates of recurrence, and mortality. Although clinical guidelines provide evidence-based recommendations for optimal treatment and monitoring, there is a dearth of information regarding treatment and monitoring patterns in clinical practice. In this study, we describe treatment and monitoring patterns among premenopausal women with HR+/HER2− aBC in real-world practice.
Methods
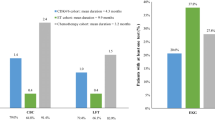
A large US claims database was used to describe treatment patterns for patients in first, second, and third lines of therapy. Treatment monitoring included complete blood count (CBC), liver function test (LFT), and electrocardiogram (EKG) monitoring, described for the first three lines of therapy, and separately for patients receiving endocrine monotherapy (ET) and chemotherapy.
Results
Among 3203 patients, chemotherapy was the most common treatment used in first-line (63.6%) and second-line therapy (66.9%). ET was used in 34.4, 30.1, and 73.6% of patients in first, second, and third lines of therapy, respectively. The two most common treatment sequences were a single line of ET (27.3%), and two consecutive lines of chemotherapy followed by a line of ET (19.3%). Patients receiving chemotherapy were monitored with CBC on average more than two times per month, and for LFT one to two times per month. Patients receiving ET were monitored with CBC and LFT on average once every 2–3 months. Overall, approximately 20% of patients were monitored with an EKG at some point during each line of therapy.
Conclusion
A considerable proportion of premenopausal women with aBC received first- and second-line chemotherapy, which appears inconsistent with current clinical guidelines. The observed treatment heterogeneity points to a lack real-world consensus on the management of premenopausal women with HR+/HER2− aBC.
Funding
Novartis Pharmaceuticals Corporation.

Similar content being viewed by others

References
Siegel RL, Miller KD, Jemal A. Cancer Statistics. CA Cancer J Clin. 2017;67(1):7–30.
Weide R, Feiten S, Friesenhahn V, Heymanns J, Kleboth K, Thomalla J, et al. Metastatic breast cancer: prolongation of survival in routine care is restricted to hormone-receptor- and Her2-positive tumors. Springerplus. 2014;3:535.
American Cancer Society. Breast cancer facts and figures 2017–2018. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2017-2018.pdf. Accessed 24 Nov 2017.
Chollet-Hinton L, Anders CK, Tse CK, Bell MB, Yang YC, Carey LA, et al. Breast cancer biologic and etiologic heterogeneity by young age and menopausal status in the carolina breast cancer study: a case-control study. Breast Cancer Res. 2016;18(1):79.
Gnerlich JL, Deshpande AD, Jeffe DB, Sweet A, White N, Margenthaler JA. Elevated breast cancer mortality in women younger than age 40 years compared with older women is attributed to poorer survival in early-stage disease. J Am Coll Surg. 2009;208(3):341–7.
Partridge AH, Hughes ME, Warner ET, Ottesen RA, Wong YN, Edge SB, et al. Subtype-dependent relationship between young age at diagnosis and breast cancer survival. J Clin Oncol. 2016;34(27):3308–14.
National comprehensive cancer network. Clinical practice guidelines in oncology (NCCN Guidelines). Breast cancer. Version 1.2017 2017. Available from: https://www.nccn.org. Accessed 3 Nov 2017.
Tripathy, D., Sohn, J., Im, S.-A., Franke, F., Bardia, A., Harbeck, N., et al.: editors. First-line ribociclib vs placebo with goserelin and tamoxifen or a non-steroidal aromatase inhibitor in premenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: Results from the randomized phase III MONALEESA-7 trial. San Antonio Breast Cancer Symposium; 2017; San Antonio.
Hansen, L.G., Chang, S., Health research data for the real world: the marketscan databases. Truven Health Analytics; 2011. Available from: http://truvenhealth.com/portals/0/assets/PH_11238_0612_TEMP_MarketScan_WP_FINAL.pdf. Accessed 5 Apr 2018.
Hurvitz S, Guerin A, Brammer M, Guardino E, Zhou ZY, Latremouille Viau D, et al. Investigation of adverse-event-related costs for patients with metastatic breast cancer in a real-world setting. Oncologist. 2014;19(9):901–8.
Ramsey SD, Martins RG, Blough DK, Tock LS, Lubeck D, Reyes CM. Second-line and third-line chemotherapy for lung cancer: use and cost. Am J Manag Care. 2008;14(5):297–306.
Seal BS, Sullivan SD, Ramsey S, Shermock KM, Ren J, Kreilick C, et al. Medical costs associated with use of systemic therapy in adults with colorectal cancer. J Manag Care Pharm. 2013;19(6):461–7.
Zhu J, Sharma DB, Gray SW, Chen AB, Weeks JC, Schrag D. Carboplatin and paclitaxel with vs without bevacizumab in older patients with advanced non-small cell lung cancer. JAMA. 2012;307(15):1593–601.
Burton T, Byfield SD, Smith GL, Zanotti G, Bell TJ, Perkins JJ, et al. Clinical and economic outcomes by first-line treatment among women with HR +/HER2- metastatic breast cancer in a large US health plan database. Curr Med Res Opin. 2016;32(8):1417–23.
Caldeira R, Scazafave M. Real-World treatment patterns for hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in Europe and the United States. Oncol Ther. 2016;4(2):189–97.
Swallow E, Zhang J, Thomason D, Tan RD, Kageleiry A, Signorovitch J. Real-world patterns of endocrine therapy for metastatic hormone-receptor-positive (HR+)/human epidermal growth factor receptor-2-negative (HER2−) breast cancer patients in the United States: 2002–2012. Curr Med Res Opin. 2014;30(8):1537–45.
Lin PL, Hao Y, Signorovitch JE, Macalalad AR, Wu EQ, Zhou Z, et al. Prescribing and monitoring patterns for HR +/HER2− advanced breast cancer: a survey of community-based oncologists. J Clin Oncol. 2014;32((15_suppl)):e11551-e.
Sledge GW, Neuberg D, Bernardo P, Ingle JN, Martino S, Rowinsky EK, et al. Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). J Clin Oncol. 2003;21(4):588–92.
Acknowledgements
Funding
Sponsorship for this study and article processing charges were funded by Novartis Pharmaceuticals Corporation. All authors had full access to all of the data in this study and take complete responsibility for the integrity and accuracy of the data analysis.
Medical Writing, Editorial, and Other Assistance
Medical writing assistance was provided by Sara Kaffashian, an employee of Analysis Group, Inc. Analysis Group received consulting fees from Novartis for the conduct of this study.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
All authors participated in the design and analytical approach of the study and contributed to the manuscript development. Results were summarized and interpreted in collaboration with all authors.
Disclosures
Anand A. Dalal is an employee of Novartis Pharmaceuticals Corporation and may own stock/stock options. Tania Small is an employee of Novartis Pharmaceuticals Corporation and may own stock/stock options. Geneviève Gauthier is an employee of Analysis Group Inc., which has received consultancy fees from Novartis Pharmaceuticals Corporation.Patrick Gagnon-Sanschagrin is an employee of Analysis Group Inc., which has received consultancy fees from Novartis Pharmaceuticals Corporation. Rebecca Burne is an employee of Analysis Group Inc., which has received consultancy fees from Novartis Pharmaceuticals Corporation. Annie Guérin is an employee of Analysis Group Inc., which has received consultancy fees from Novartis Pharmaceuticals Corporation. Polly Niravath received honoraria from Novartis as a consultant.
Compliance with Ethics Guidelines
Data are de-identified and comply with the confidentiality requirements outlined in the Health Insurance Portability and Accountability Act. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data Availability
The claims database (Truven Health Analytics MarketScan Commercial database) is proprietary, provided by a third-party vendor, and the authors do not have permission to disseminate the data without the vendor’s approval. The study sponsor has purchased access to the database (the authors have been granted access to the data on a contract per project use). Access to this data set is available to any other interested parties for a fee set by Truven Health Analytics MarketScan Commercial database (https://marketscan.truvenhealth.com/marketscanportal/).
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Content
To view enhanced digital content for this article go to https://doi.org/10.6084/m9.figshare.6871499.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Dalal, A.A., Gauthier, G., Gagnon-Sanschagrin, P. et al. Treatment and Monitoring Patterns Among Premenopausal Women with HR+/HER2− Advanced Breast Cancer. Adv Ther 35, 1356–1367 (2018). https://doi.org/10.1007/s12325-018-0764-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-018-0764-3