
Abstract
Background
The 2015 American Thyroid Association (ATA) guidelines proposed the use of the ATA Risk Stratification System and American Joint Committee on Cancer Tumor-Node-Metastasis (AJCC/TNM) Staging System for postoperative radioiodine decision-making. However, the management of patients with intermediate-risk differentiated thyroid carcinoma (DTC) is not well defined. In this study, we aimed to evaluate the therapeutic efficacy of radioactive iodine therapy (RAIT) among various subgroups of patients with intermediate-risk DTC after surgery.
Methods
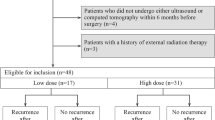
This was a retrospective study based on the Surveillance, Epidemiology, and End Results (SEER) database (2010–2015). The DTC patients with intermediate risk of recurrence were divided into two groups (treated or not treated with radioactive iodine (RAI)). As the treatment was not randomly assigned, stabilized inverse probability treatment weighting (sIPTW) was used to reduce selection bias. We used the Kaplan-Meier method and log-rank test to analyze overall survival (OS) and cancer-specific survival (CSS).
Results
Kaplan-Meier analysis after sIPTW found a significant difference in OS and CSS between no RAIT and RAIT (log-rank test, P < 0.0001; P = 0.0019, respectively). The Kaplan–Meier curves of CSS in age cutoff of 55 years showed a significant association between no RAIT and RAIT (log-rank test, P = 0.0045). Univariate and multivariate Cox regression showed RAIT was associated with a reduced risk of mortality compared with no RAIT (hazard ratio [HR] 0.59, 95% confidence interval [95% CI 0.44–0.80]). Age (≥ 55) years showed a worse CSS regardless of whether or not a patient was treated or not treated with RAI ([HR] 8.91, 95% confidence interval [95% CI 6.19–12.84]).
Conclusions
RAIT improves OS and CSS in patients with intermediate-risk DTC after surgery. 55 years is a more appropriate prognostic age cutoff for the relevant classification systems and is a crucial consideration in RAI decision-making. Therefore, we need individualized treatment plans.



Similar content being viewed by others


References
R.L. Siegel, K.D. Miller, H.E. Fuchs et al. Cancer statistics, 2022. CA Cancer J. Clin. 72(1), 7–33 (2022). https://doi.org/10.3322/caac.21708
K.D. Miller, L. Nogueira, T. Devasia et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J. Clin. 72(5), 409–436 (2022). https://doi.org/10.3322/caac.21731
U.C. Megwalu, P.K. Moon, Thyroid cancer incidence and mortality trends in the United States: 2000–2018. Thyroid 32(5), 560–570 (2022). https://doi.org/10.1089/thy.2021.0662
B. Aschebrook-Kilfoy, M.H. Ward, M.M. Sabra et al. Thyroid cancer incidence patterns in the United States by histologic type, 1992–2006. Thyroid 21(2), 125–134 (2011). https://doi.org/10.1089/thy.2010.0021
L. Dal Maso, A. Tavilla, F. Pacini et al. Survival of 86,690 patients with thyroid cancer: a population-based study in 29 European countries from EUROCARE-5. Eur. J. Cancer 77, 140–152 (2017). https://doi.org/10.1016/j.ejca.2017.02.023
R.M. Tuttle, S. Ahuja, A.M. Avram et al. Controversies, consensus, and collaboration in the use of (131)I therapy in differentiated thyroid cancer: a joint statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association. Thyroid 29(4), 461–470 (2019). https://doi.org/10.1089/thy.2018.0597
M.R. Haymart, M. Banerjee, A.K. Stewart et al. Use of radioactive iodine for thyroid cancer. JAMA 306(7), 721–728 (2011). https://doi.org/10.1001/jama.2011.1139
B.R. Haugen, E.K. Alexander, K.C. Bible et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 26(1), 1–133 (2016). https://doi.org/10.1089/thy.2015.0020
M.B. Amin, F.L. Greene, S.B. Edge et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 67(2), 93–99 (2017). https://doi.org/10.3322/caac.21388
L. Valerio, F. Maino, M.G. Castagna et al. Radioiodine therapy in the different stages of differentiated thyroid cancer. Best Pract. Res. Clin. Endocrinol. Metab. 2022;101703, https://doi.org/10.1016/j.beem.2022.101703
M. Schlumberger, S. Leboulleux, Current practice in patients with differentiated thyroid cancer. Nat Rev Endocrinol 17(3), 176–188 (2021). https://doi.org/10.1038/s41574-020-00448-z
E. Ruel, S. Thomas, M. Dinan et al. Adjuvant radioactive iodine therapy is associated with improved survival for patients with intermediate-risk papillary thyroid cancer. J Clin Endocrinol Metab 100(4), 1529–1536 (2015). https://doi.org/10.1210/jc.2014-4332
S.K. Kim, J.W. Woo, J.H. Lee et al. Radioactive iodine ablation may not decrease the risk of recurrence in intermediate-risk papillary thyroid carcinoma. Endocr Relat Cancer 23(5), 367–376 (2016). https://doi.org/10.1530/erc-15-0572
S. Xu, C. Ross, M.A. Raebel et al. Use of stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health 13(2), 273–277 (2010). https://doi.org/10.1111/j.1524-4733.2009.00671.x
S. Ballal, R. Soundararajan, A. Garg et al. Intermediate-risk differentiated thyroid carcinoma patients who were surgically ablated do not need adjuvant radioiodine therapy: long-term outcome study. Clin. Endocrinol. 84(3), 408–416 (2016). https://doi.org/10.1111/cen.12779
K. Han, H.M. Noh, H.M. Jeong et al. Is postoperative adjuvant radioactive iodine ablation therapy always necessary for intermediate-risk papillary thyroid cancer patients with central neck metastasis? Ann. Surg. Oncol. 28(12), 7533–7544 (2021). https://doi.org/10.1245/s10434-021-10164-1
J. Johar, H. Britton, S.M. Wiseman, Older patients with differentiated thyroid cancer exhibit more aggressive pathological characteristics than younger patients. Can. J. Surg. 63(1), E69–e70 (2020). https://doi.org/10.1503/cjs.017918
T.H. Kim, Y.N. Kim, H.I. Kim et al. Prognostic value of the eighth edition AJCC TNM classification for differentiated thyroid carcinoma. Oral. Oncol. 71, 81–86 (2017). https://doi.org/10.1016/j.oraloncology.2017.06.004
M. Kim, W.G. Kim, H.S. Oh et al. Comparison of the seventh and eighth editions of the American Joint Committee on cancer/union for international cancer control tumor-node-metastasis staging system for differentiated thyroid cancer. Thyroid 27(9), 1149–1155 (2017). https://doi.org/10.1089/thy.2017.0050
I.J. Nixon, L.Y. Wang, J.C. Migliacci et al. An international multi-institutional validation of age 55 years as a cutoff for risk stratification in the AJCC/UICC staging system for well-differentiated thyroid cancer. Thyroid 26(3), 373–380 (2016). https://doi.org/10.1089/thy.2015.0315
S.M. Chow, S. Yau, C.K. Kwan et al. Local and regional control in patients with papillary thyroid carcinoma: specific indications of external radiotherapy and radioactive iodine according to T and N categories in AJCC 6th edition. Endocr. Relat. Cancer 13(4), 1159–1172 (2006). https://doi.org/10.1677/erc.1.01320
I.J. Nixon, M.M. Whitcher, F.L. Palmer et al. The impact of distant metastases at presentation on prognosis in patients with differentiated carcinoma of the thyroid gland. Thyroid 22(9), 884–889 (2012). https://doi.org/10.1089/thy.2011.0535
A. Piccardo, F. Arecco, M. Puntoni et al. Focus on high-risk DTC patients: high postoperative serum thyroglobulin level is a strong predictor of disease persistence and is associated to progression-free survival and overall survival. Clin. Nucl. Med. 38(1), 18–24 (2013). https://doi.org/10.1097/RLU.0b013e318266d4d8
Funding
Natural Science Foundation of China (No. 82070878). Natural Science Foundation of Fujian Province (Grant No. 2020J011081, 2021J01381 and 2022J01521).
Author information
Authors and Affiliations
Contributions
J.W.: Conceptualization (lead); writing – original draft (lead); data curation (lead); formal analysis (lead); software (equal). Y.M.: Writing – original draft (supporting); formal analysis (supporting); software (equal);. L.L.: Methodology (lead); writing – original draft (supporting); writing – review and editing (equal). J.L.: Writing – review and editing (equal). H.H.: Writing – review and editing (equal). Wei Lin:Methodology (supporting); writing – review and editing (equal). G.C.:Writing – review and editing (equal). J.W.:Conceptualization (supporting); supervision (lead) ;writing – original draft (supporting); writing – review and editing (equal).
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: **wen Wang, Yaqian Mao, Liantao Li
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, J., Mao, Y., Li, L. et al. Survival benefit of postoperative radioiodine therapy among patients with intermediate-risk differentiated thyroid carcinoma. Endocrine (2024). https://doi.org/10.1007/s12020-024-03869-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12020-024-03869-2