
Abstract
In the context of an ongoing and worsening drug overdose epidemic in the USA, increases in free support services like self-help groups may be expected. We estimated differences in self-help use by age, period, or cohort among people who may have needed treatment. We included N = 92,002 adults from the 2002–2018 National Surveys on Drug Use and Health who met past-year DSM-IV substance use disorder criteria or received alcohol/drug treatment in any location. We used hierarchical age-period-cohort (HAPC) modeling to estimate average age-period-cohort associations with self-help. Level-1 covariates included age, race and ethnicity, household income, and sex. We quantified level-2 variance components using the median odds ratio (MOR). We found small positive HAPC period effects for alcohol/drug self-help that were driven by alcohol-specific effects. Birth cohort differences were observed starting at age 48. Younger birth cohorts, especially among Black adults, were less likely to report self-help use than older birth cohorts. MOR was consistently elevated for cohort effects (MOR = 1.17; covariance parameter: 0.15; 95% CI [0.11, 0.23]) but not for period effects. Overall, self-help use did not increase in the context of substantial treatment needs and worsening overdose racialized disparities. Instead, cohort effects explained trends in alcohol/drug self-help. Findings could indicate that younger birth cohorts may need additional supports, especially services tailored for Black and Hispanic people.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Substance use disorders (SUDs) are associated with significant morbidity and mortality (Kariisa et al., 2022; Mattson et al., 2021; Townsend et al., 2022), and yet treatment utilization in the USA is low across substances and demographic groups (Askari et al., 2021; Krasnova et al., 2021; Mauro et al., 2022a, b). In 2018, 7.8% of adults had a past-year SUD, but only 11.2% of those with SUD reported receiving any past-year services (Substance Abuse & Mental Health Services Administration, 2019b). Treatment use can range by type of SUD, with lower past-year treatment for alcohol use disorders than drug use disorders (i.e., 8% and 14%, respectively) (Grant et al., 2015, 2016). Age-related patterns in SUD treatment have been consistently observed across substances, with middle adulthood and middle age being positively associated treatment despite the highest burden of SUDs being in young adulthood (Morgan Snell et al., 2020). Many structural and individual barriers impede access and use of evidence-based services to reduce SUD-related burden in the USA, including lack of insurance coverage, limited or no access to providers, and low perceived need for treatment (Tomko et al., 2022; Verissimo & Grella, 2017).
Self-help programs are among the most common type of services used to achieve or maintain abstinence from alcohol or drugs among people who report any SUD-related services (Grant et al., 2015, 2016; Wu et al., 2016). Self-help programs are free and readily available around the USA (Kelly et al., 2020), which could reduce logistical and financial barriers hindering specialty SUD treatment use (Ali et al., 2017), and could be particularly useful in resource-limited settings where SUD treatment provider availability is insufficient (Paquette et al., 2019). General guidelines indicate that self-help groups can support individuals seeking services when combined health professionally led treatment (National Institute on Alcohol Abuse & Alcoholism, 2014). SUD treatment programs can integrate professionally led 12-step facilitation or encourage participation in self-help groups (National Institute on Drug Abuse, 2018). Starting with Alcoholics Anonymous (AA) in the 1930s (Gross, 2010), the 12-step model has been extended to include Narcotics Anonymous (NA) (Bog, 2017), various drug-specific self-help programs (Donovan & Wells, 2007) and target membership subgroups (Hillhouse & Fiorentine, 2001; Hoffman, 1994).
While NA/AA has been studied for years, program effects have been mixed. Some study findings indicate positive effects (Gamble & O'Lawrence, 2016; Kelly et al., 2020). For example, AA or 12-step facilitation engagement has been associated with abstinence or reduced alcohol use (Kelly et al., 2020), while NA programs have been associated with treatment retention, adherence to medications for opioid use disorder, and abstinence (Lookatch et al., 2019; Monico et al., 2015). However, other studies indicate NA/AA is not more efficacious than other psychosocial interventions or no interventions in increasing abstinence (Bog, 2017; Miller, 2008). In the context of these mixed findings, national trends over time in self-help group participation across subgroups are poorly understood. A recent review of racial and ethnic disparities in mutual help group participation found inconsistent findings signaling potential disparities in use among Hispanic and Black people, and called for updated and methodologically rigorous studies examining self-help use (Zemore et al., 2021).
Trends over time in self-help use are likely influenced by a combination of several factors including period, cohort, and age effects. Period effects would include changes in the prevalence over time that are common across all in the target population. Cohort effects would include specific birth cohorts that have higher or lower rates of self-help use across the life course. Age effects would include consistent developmental variation in self-help use (e.g., higher rates of use in middle age). Assessing this variation is critical to understanding temporal patterns of self-help use, including highlighting those cohorts and age groups at highest need for targeted intervention. However, age, period, and cohort effects of self-help use in the USA have not been directly examined.
Current Study
In this study, we conducted an age-period-cohort analysis of self-help group use in the USA between 2002 and 2018. We aimed to disentangle the expected period effects from age effects and potential cohort effects associated with self-help use in the context of an overdose epidemic driven by opioids (Wilson et al., 2020) and gaps in access to specialized treatment facilities (Hadland et al., 2020). Consistent with low SUD treatment use, we hypothesized that self-help use would be low throughout the study period, but anticipated higher uptake in recent years due to increases in overdose events contributing to period effects, particularly drug self-help use, as attention to the overdose epidemic increased in the USA. Our study also responds to calls to improve the evidence base examining racial and ethnic disparities in self-help (Zemore et al., 2021). We assessed whether observed relationships varied by sociodemographic characteristics, including race and ethnicity, sex, education, and income. Findings could inform whether specific cohorts or subgroups could need additional supports to increase engagement in SUD services broadly, if self-help use can increase engagement in other services (Klein & Seppala, 2019), and whether tailored interventions are needed to engage marginalized groups who are systematically excluded from services.
Methods
Data Source and Sample
The National Survey on Drug Use and Health (NSDUH) is an annual cross-sectional US study of community-based people. The survey sampled people ages 12 and older in households in all 50 states, including homeless shelters and nursing homes, and excluding people who were institutionalized or in correctional settings. In-person computer-assisted data collection included audio computer assisted self-interviewing (ACASI) to increase reporting of sensitive health behaviors. Weighted interview rates were 78.6% in 2002 and 66.6% in 2018; additional methodological information is reported elsewhere (Substance Abuse & Mental Health Services Administration, 2003, 2019a).
The 2002–2018 NSDUH public use files included N = 949,285 community-based people ages 12 and older. Of the n = 664,152 respondents ages 18 + , we included n = 92,983 adults who may have needed alcohol/drug treatment in 2002–2018. Consistent with NSDUH definitions, treatment need was defined as meeting past-year SUD criteria or past-year use of alcohol/drug treatment services in any location. Past-year SUD was based on DSM-IV criteria for alcohol/drug abuse or dependence (American Psychiatric Association, 1994), as DSM-5 criteria released in 2013 were not collected. Among people reporting lifetime treatment (i.e., “Have you ever received treatment or counseling for your use of alcohol or any drug, not counting cigarettes?”), past-year treatment included people reporting any alcohol or drug treatment within the past 12 months (i.e., “How long has it been since you were last in treatment or counseling for your alcohol or drug use, not counting cigarettes?”). After excluding n = 981 with missing birth cohort or age, our final analytic sample included n = 92,002 adults in the 2002–2018 NSDUH.
Measures
Self-Help Group Use
Our primary outcome was past-year self-help group use, defined as any past-year 12-step or peer support services use for alcohol or drug use. Respondents were asked, “During the past 12 months, have you received treatment for your [alcohol/drug use] in a self-help group such as Alcoholics Anonymous or Narcotics Anonymous?” “Was the treatment you received in a self-help group for your alcohol use, your drug use, or both?” Responses from these two questions were combined to capture self-help groups for alcohol use, drug use, or either alcohol or drug (i.e., alcohol/drug) use.
Period, Age, and Cohort
Period was defined as the survey calendar year. As exact year of age was not provided in the public NSDUH files, we used alternative questions to compute an approximate age, as described elsewhere (Miech et al., 2013). Briefly, respondents were asked both age and the calendar year when they first used each substance reported (e.g., alcohol, cannabis). We derived birth year to estimate birth cohort by subtracting the year of the first reported substance use from the age that they reported being at first use. For example, if a respondent reported first consuming alcohol at age 15 in the year 2000, then we assigned 1985 as that respondent’s birth year. We performed reliability checks on this approach by comparing each estimated birth year of respondents based on the age and year of first use of each substance for those with more than one substance available (15 maximum substances). Cronbach’s alpha across birth cohort measures derived from different self-reported substance use onset was high (α = 0.98). Imputed birth cohort combined years 1904–1945 and had single-year birth cohorts thereafter. Imputed age was assigned to each respondent as the survey year minus imputed birth year, and then categorized into the following age groups: 12–17, 18–25, 26–34, 35–49, 50–64, and 65 or older. Cronbach’s alpha comparing age categories provided by NSDUH and imputed age categories was high (α = 0.9967).
Socio-Demographics
Individual characteristics included race and ethnicity, sex, education, and income. Public use files which combined all Hispanic people into one category, regardless of racial group. Among people not identified as Hispanic, we were able to distinguish the following racial subgroups: Black/African American, white, Asian/Pacific Islander/Native Hawaiian, and all other non-Hispanic groups including multiracial/multiethnic/Native American/Alaskan Native. Sex was measured with a binary variable (male, female); gender identity was not collected. Education was categorized as less than high school, high school, some college, or college grad. Household income categories included $0–19,999, $20,000–49,999, $50,000–74,999, and $75,000 + .
Statistical Analysis
We first estimated the survey-weighted prevalence of alcohol/drug self-help use for people who may have needed alcohol/drug treatment by age categories and birth cohorts in 2002–2018. Next, we used a hierarchical age-period-cohort (HAPC) statistical model to estimate the average association of age, period, and cohort and self-help group use. Statistical modeling of age-period-cohort effects encounters identification problems due to the collinearity between age, period, and cohort (Cohort = Period-Age). Assumptions underlying various statistical models have been the subject of long debate (Glenn, 1976). We used an HAPC model; a cross-classified random effects model in which the level-1 association between age and the outcome was assessed with an age fixed effect, and the intercept was allowed to vary across two level-2 components (i.e., year and birth cohort as random intercept variables) that were correlated but non-nested (Yang, 2006; Yang & Land, 2008, 2013; Yang et al., 2004). We estimated logistic HAPC models with level-1 covariates of age, race and ethnicity, household income, and sex, with any past-year self-help group use for alcohol/drugs as a binary outcome. We then graphed the log odds of self-help distinguishing period effects and cohort effects adjusted for level-1 covariates. Estimates and confidence intervals overlap** the null (graph line marking log odds of zero) were consistent with no adjusted period effects when controlling for age and cohort effects and vice versa.
The level-2 variance components were quantified using the median odds ratio (MOR) (Merlo et al., 2006) to capture the amount of variance in the outcome that differed by the level-2 random components. The MOR is conceptually similar to the intra-class correlation statistic that estimated the amount of variance explained by the level-2 covariates in the model. The higher the MOR, the more that differences across level-2 variance components explained differences in the outcome. For example, a high MOR for cohort effects would indicate that there are large differences in self-help prevalence across cohorts.
We then repeated procedures estimating subgroup HAPC models stratified by race and ethnicity, sex, education, and household income. Finally, we examined alcohol self-help and drug self-help as separate outcomes among people who may have needed alcohol treatment (n = 73,628) or drug treatment (n = 34,853).
Data management was conducted in STATA (StataCorp, 2017), figures in R (R Core Team, 2020), and HAPC analyses in SAS software, Version 9.4 of the SAS System (SAS Institute In, Cary, NC, USA).
Results
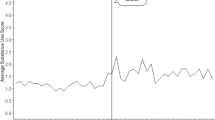
Figure 1 shows the weighted prevalence of past-year self-help use among adults who may have needed alcohol-only, drug-only, or either alcohol/drug treatment, respectively. Alcohol self-help use had a peak prevalence of 9.76% among adults who may have needed alcohol treatment in 2009. Drug self-help use prevalence among adults who may have needed drug treatment was consistently higher than alcohol self-help and generally decreased over time, peaking at 17.00% in 2006 and declining to 11.37% by 2018. Supplemental Fig. 1 reports self-help use prevalence among all community-based adults regardless of whether individuals may have needed alcohol/drug treatment, and indicates that self-help use prevalence was low overall, peaking around 2009–2010.

Prevalence of past-year self-help use for alcohol, drug, and alcohol/drug use among adults 18 and older who may have needed treatment, NSDUH 2002–2018. Note: Treatment need included people who met criteria for a substance use disorder (DSM-IV abuse or dependence) or reported receiving treatment for their alcohol or drug use in any location in the past year. N = 73,628 for alcohol use treatment need; N = 34,853 for drug use treatment need; N = 92,002 for alcohol/drug use treatment need
Figure 2 shows past-year alcohol/drug self-help use prevalence (Y axis) across age categories (X axis) among adults who may have needed treatment, with each line representing a different birth cohort with data observable in the 2002–2018 NSDUH. Self-help use peaked at approximately age 60. Cohort effects can be observed by comparing points in the life course when multiple birth cohorts have data. Differences by birth cohort are most observable for those in mid-life into older adulthood, starting in ages 48–52. Younger birth cohorts overall had lower self-help use than those in middle adulthood.

Age- and birth cohort-specific prevalence of past-year alcohol/drug self-help use among adults 18 and older who may have needed treatment, NSDUH 2002–2018 (N = 92,002). Note: Treatment need included people who met criteria for a substance use disorder (DSM-IV abuse or dependence) or reported receiving treatment for their alcohol or drug use in any location in the past year
Figure 3 provides the log odds and 95% confidence intervals (CI) of the period effects and cohort effects for alcohol/drug self-help use adjusted for sex, race and ethnicity, education, and household income. For period effects (left panel), the X axis indicates calendar year, while for cohort effects (right panel) the X axis indicates birth cohort year. Compared to other years, the period effect was lower in 2002 (β = − 0.19; 95% CI − 0.25, − 0.14), and elevated in 2017 (β = 0.18; 95% CI 0.13, 0.24). However, overall trends in alcohol/drug self-help were predominately driven by cohort effects, as evidenced by the larger magnitude of association in the right panel. Self-help use was highest for people from cohorts born in the 1950s through the early 1970s (i.e., positive log odds of self-help use), and lower in more recent birth cohorts (i.e., negative log odds of self-help use) starting in the early to mid-1990s. Unadjusted alcohol/drug self-help use period and cohort effects (Supplemental Fig. 2A) were similar to adjusted results and mirrored patterns for alcohol self-help (Supplemental Fig. 2B). Period and cohort effects for drug self-help contrast these findings, indicating only cohort effects for drug self-help (Supplemental Fig. 2C). Drug self-help was generally higher among cohorts born before 1965, and lower for younger cohorts born after 1990.

Adjusted period and cohort effects of receiving self-help services for alcohol/drug use among adults 18 and older who may have needed treatment, NSDUH 2002–2018 (N = 92,002). Note: Treatment need included people who met criteria for a substance use disorder (DSM-IV abuse or dependence) or reported receiving treatment for their alcohol or drug use in any location in the past year. Estimates were derived from hierarchical age-period-cohort models adjusting for sex, race and ethnicity, education, and household income
Period effects for alcohol/drug self-help use by race and ethnicity were largely consistent across subgroups, as shown in the overlap** lines in the left panel of Fig. 4. Some differences in cohort effects emerged, specifically higher alcohol/drug self-help use among cohorts of Black adults born between 1904 and 1950 that contrasted lower, yet highly variable, self-help use in Hispanic and other/multiracial/multiethnic/Native American/Alaskan Native respondents. There were generally no cohort effects among non-Hispanic white adults born before 1995. The declining alcohol/drug self-help use among the youngest cohorts observed across racial and ethnic groups, however, was most evident among Black and Hispanic adults (Fig. 4). There was little variation in period and cohort effects by sex (Supplemental Fig. 3), education (Supplemental Fig. 4), and household income (Supplemental Fig. 5).

Racial and ethnic group-stratified period and cohort effects of receiving self-help services for alcohol/drug use among adults 18 and older who may have needed treatment, adjusted for covariates, NSDUH 2002–2018 (N = 89,466). Treatment need included people who met criteria for a substance use disorder (DSM-IV abuse or dependence) or reported receiving treatment for their alcohol or drug use in any location in the past year, including non-Hispanic Black/African American (n = 9955), Hispanic (n = 13,330), non-Hispanic white (n = 60,689), and non-Hispanic other race (n = 5492) adults. Non-Hispanic Asian/Pacific Islander adults were excluded (n = 2536) due to model convergence issues. Estimates were derived from hierarchical age-period-cohort models stratified by race and ethnicity adjusting for sex, education, and household income
Finally, we examined the MOR to assess the extent to which cohort and period effects described variance in alcohol/drug self-help use over time and found substantial evidence for cohort effects in alcohol/drug self-help use (Table 1). The overall cohort effect MOR of 1.17 (covariance parameter: 0.15; 95% CI [0.11, 0.23]) indicated that the odds of two datapoints with similar outcomes being in the same birth cohort was higher than null. Further, the cohort-level MOR was higher than the period effects MOR (1.07 (covariance parameter 0.01, 95% CI [0.01, 0.03]), indicating that there was more group-level clustering by cohort than by period. The cohort effect MOR was consistently elevated when adjusting for sex, race and ethnicity, education, or household income. Among models that converged with stratified data by sex, race and ethnicity, education, or household income, the cohort effect MOR ranged from 1.15 (covariance parameter: 0.12; 95% CI [0.09, 0.18]) among adults who completed high school but not college, to 1.93 (covariance parameter 2.39, 95% CI [1.64, 3.84]) among adults reporting other racial or ethnic groups. Period effects explained minimal variance in alcohol/drug self-help across strata. Supplemental Table 1 provides separate MORs for alcohol self-help, which were consistent with Table 1, and drug self-help, which had strata with additional convergence issues related to smaller sample sizes.
Discussion
We estimated age-period-cohort effects of alcohol/drug self-help use in a national sample of US adults between 2002 and 2018. We found that small positive period effects in alcohol/drug self-help were driven by alcohol self-help, but not drug self-help, in the context of an ongoing drug overdose epidemic (Mattson et al., 2021). We found larger cohort effects in self-reported self-help group use, with Baby Boomers and earlier cohorts reporting higher past-year self-help use, and lower self-help use among younger cohorts, particularly among Black and Hispanic adults. Recent cohort declines in self-help may signal broader changes in individuals’ preferences and practices in the recovery community. Our findings could reflect cohort differences in self-identifying treatment need and influence decisions to use support services. Indeed, it can take decades from onset of symptoms for people to seek services for alcohol or drug use disorders (Blanco et al., 2015). If lower self-help use is indicative of reductions in problem identification, one would expect similar cohort differences in other SUD treatment use, which could contribute to worsening racial and ethnic inequities in SUD-related outcomes. Future studies should estimate whether the cohort effects are specific to self-help or also evident in other SUD service use patterns.
Contrary to expectations, there were no period effects in drug self-help from 2002 to 2018 after accounting for cohort and age effects, and drug self-help use was not higher in more recent years when the overdose epidemic worsened in the US. Self-help groups’ reliance on abstinence from all substances, often including medication, could contribute to reductions in self-help group as opioid-related burden increased. One potential explanation is stigma towards medications to treat drug use disorders. Stigma could act as a barrier for drug self-help engagement because people in NA programs are often not considered abstinent if they are using medication to treat the disorder (Krawczyk et al., 2018; Monico et al., 2015). Drug use stigma also permeates interactions with the healthcare system more broadly, evidenced by most adults who use drugs not discussing drug use with their care providers, even if drug use discussions are positively associated with drug treatment (Mauro et al., 2020). In contrast, more than half of adults who use alcohol report discussing alcohol with the providers, though these interactions are also racially patterned (Mauro et al., 2022b). Poor healthcare interactions and gaps in care could further contribute to the structural marginalization and vulnerability that people with drug use disorders experience, contributing to the concentration of overdoses or other negative substance-related outcomes in areas with higher economic disadvantage (Pear et al., 2019).
The null period effects and negative cohort effects in younger cohorts could indicate that drug self-help participation will decline in future years. However, patterns could also differ by type of drug use disorder. For example, recent findings indicate that an average of 6% of people with cannabis use disorder received any past-year treatment between 2002 and 2019, including self-help, with trends indicating reductions over time (Askari et al., 2021). In contrast, any treatment services (including self-help) among people with opioid use disorder seems to have remained constant. In a study using 2005–2013 data, 26.2% of people with opioid use disorder reported any alcohol/drug services, of whom more than half reported using self-help services (Wu et al., 2016). When using a 2019 sample, 26.1% of people with opioid use disorder reported any services, which included self-help, office-based interventions and medication (Mauro et al., 2022a). Due to sample size limitations, we could not examine age-period-cohort effects within distinct drug use disorders, particularly for marginalized groups of people using drugs with substantial stigma (e.g., heroin) who are often missed in general population surveys (Midgette et al., 2021; Nesoff et al., 2022; Reuter et al., 2021). Therefore, we could not determine if people with drug use disorders most strongly associated with drug overdoses (e.g., opioid use disorders) had distinct cohort and period effects. Future studies should explore drug-specific differences in larger samples oversampling hard to reach populations.
Differences in effects by racial and ethnic subgroups have important clinical implications. Larger cohort effects among younger Black Americans indicate that they are less likely to use peer support services than their non-Hispanic white counterparts. Our findings help clarify mixed results reported in a recent review of racial and ethnic disparities in mutual help participation (Zemore et al., 2021), specifically identifying racialized patterns of self-help use in the youngest cohorts. Because self-help engagement could have potential benefits (Kelly et al., 2020), cohort differences in self-help use among Black Americans could then translate to differences in SUD-related outcomes and worsening disparities in the USA. In a recent study, increases in opioid-related overdose deaths in the USA between 2007 and 2019 were more than three times higher among Black people than among white people (575% vs. 184%), and were five time higher for stimulant-related overdose deaths (16,200% vs. 3200%) (Townsend et al., 2022). Access to medication for opioid use disorder also appears to be racially patterned, with 31% of white people needing treatment reporting medication use in 2019, compared to 20% of Black and 15% of Hispanic people (Mauro et al., 2022a). At the same time, higher rates of coercive treatment among racial minoritized groups that are systematically criminalized due to racism could translate to lower access to evidenced based services. For example, opioid use disorder treatment episodes referred through the criminal legal system are more likely than self-referrals to rely on self-help without medication (Wen et al., 2020), and less likely to receive medication that other referrals (Mantha et al., 2020). Future studies should disentangle whether lower self-help use across subgroups of more recent birth cohorts is related to changes in coercive treatment.
Importantly, we did not seek to determine who should or should not engage in peer support, which should be an individual and clinical decision, or to estimate the effectiveness of self-help use. In a 2020 Cochrane review, AA and 12-step facilitation engagement was associated with abstinence from alcohol and sustained reductions in alcohol use (Kelly et al., 2020). Similarly, NA programs have been found to enhance treatment retention, including adherence to medications for opioid use disorder, as well as abstinence (Lookatch et al., 2019; Monico et al., 2015). Self-help groups have been associated with SUD treatment attendance (Vogel et al., 2020) and other positive clinical outcomes (Kelly et al., 2020), but other studies found no effects of these programs (Bog, 2017; Miller, 2008). Cohort declines in self-help use could be yet another signal of needed investments in the SUD treatment system to increase treatment uptake both in primary care and specialty settings.
Our findings have implications for SUD service access and engagement during the COVID-19 pandemic, as many people may have chosen or been forced to forego in-person health-related services, including substance-related services. In response to COVID-19, many 12-step programs moved online (Galanter et al., 2022), relying on free versions of video communication platforms to maintain social distance. However, these support networks would be limited to people having internet access in a private place; anonymity and non-disclosure may not be possible for people in shared spaces and may be inaccessible to people without access to reliable internet. This could lead to worsening socioeconomic disparities in self-help program engagement reflective of gaps in alcohol/drug treatment access. Future studies should estimate the effects of the COVID-19 pandemic on self-help use as well as broader SUD treatment engagement.
Limitations included approximations of chronological age, which was estimated by triangulating data in the survey. However, this approach was necessary to complement the public-use imputed age categories. While ACASI could reduce social desirability bias, recall bias could affect all self-reported measures. Our secondary data analysis of the NSDUH used DSM-IV measures, so findings may not generalize to everyone meeting SUD criteria using the DSM-5 SUD thresholds. Future findings should aim to reproduce our findings using DSM-5 SUD measures. The public use NSDUH combined race and ethnicity into one categorical measure that did not allow us to distinguish racial group membership among people who identified as Hispanic. As people identifying as Hispanic or Latinx are a widely heterogeneous group (Krogstad et al., 2022), future studies with restricted data access should replicate our approach further disaggregating by racial and ethnic subgroups. As NSDUH systematically excluded people who were institutionalized or in correctional settings, people disproportionately affected by institutional racism and mass incarceration, such as young Black men, may be under-represented in our study. The 2015 NSDUH redesign changed certain substance use questions that could affect which individuals were asked about drug self-help use. The null period effects in our study for drug self-help use mitigate concerns about comparability of survey estimates before and after 2015. The public data did not include geographic measures (e.g., state), so future studies should test for differences in service availability by location.
In conclusion, self-help use trends among people who may have needed alcohol/drug treatment were largely explained by cohort differences; self-help use was lower among younger cohorts than older cohorts, especially among Black adults. Our findings call for studies assessing challenges in SUD service engagement as USA overdose-related deaths increasingly involve stimulants, for which there are currently no pharmacological treatments. Decreasing self-help use could indicate a need to invest in public health resources to increase SUD treatment availability and engagement both in primary and specialty settings. Future studies should assess if our HAPC findings are specific to self-help services or generalize to specialty treatment in various settings.
Data Availability
Data are publicly available at https://www.datafiles.samhsa.gov/.
Abbreviations
- AA:
-
Alcoholics Anonymous
- ACASI:
-
Audio computer assisted self-interviewing
- DSM-IV:
-
Diagnostic and Statistical Manual of Mental Disorders fourth edition
- HAPC:
-
Hierarchical age-period-cohort
- MOR:
-
Median odds ratio
- NA:
-
Narcotics anonymous
- NSDUH:
-
National Survey on Drug Use and Health
- SUD:
-
Substance use disorder
References
Ali, M. M., Teich, J. L., & Mutter, R. (2017). Reasons for not seeking substance use disorder treatment: Variations by health insurance coverage. The Journal of Behavioral Health Services & Research, 44(1), 63–74. https://doi.org/10.1007/s11414-016-9538-3
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed). Washington, DC: American Psychiatric Association.
Askari, M. S., Keyes, K. M., & Mauro, P. M. (2021). Cannabis use disorder treatment use and perceived treatment need in the United States: time trends and age differences between 2002 and 2019. Drug Alcohol Depend, 229, 109154. https://doi.org/10.1016/j.drugalcdep.2021.109154
Blanco, C., Iza, M., Rodriguez-Fernandez, J. M., Baca-Garcia, E., Wang, S., & Olfson, M. (2015). Probability and predictors of treatment-seeking for substance use disorders in the U.S. Drug and Alcohol Dependence, 149, 136–144. https://doi.org/10.1016/j.drugalcdep.2015.01.031
Bog, M., Filges, T., Brannstrom, L., Jorgensen, A. M. K, Fredrikkson, M. K. (2017). 12-step programs for reducing illicit drug use: a systematic review. Campbell Systematic Reviews, 2. https://doi.org/10.4073/csr.2017.2
Center for Behavioral Health Statistics and Quality. (2019). 2018 National Survey on Drug Use and Health: Methodological Resource Book, Section 8: Data Collection Final Report. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Donovan, D. M., & Wells, E. A. (2007). “Tweaking 12-Step”: The potential role of 12-Step self-help group involvement in methamphetamine recovery. Addiction, 102(Suppl 1), 121–129. https://doi.org/10.1111/j.1360-0443.2007.01773.x
Galanter, M., White, W. L., & Hunger, B. (2022). Virtual twelve step meeting attendance during the COVID-19 period: a study of members of Narcotics Anonymous. J Addict Med, 16(2), 381-e86. https://doi.org/10.1097/ADM.0000000000000852
Gamble, J., & O'Lawrence, H. (2016). An Overview of the Efficacy of the 12-Step Group Therapy for Substance Abuse Treatment. J Health Hum Serv Adm, 39(1), 142–160.
Glenn, N. D. (1976). Cohort analysts’ futile quest: Statistical attempts to separate age, period and cohort effects. American Sociological Review, 41(5), 900–904.
Grant, B. F., Goldstein, R. B., Saha, T. D., Chou, S. P., Jung, J., Zhang, H., & Hasin, D. S. (2015). Epidemiology of DSM-5 alcohol use disorder: results from the national epidemiologic survey on alcohol and related conditions III. JAMA Psychiatry, 72(8), 757–766. https://doi.org/10.1001/jamapsychiatry.2015.0584
Grant, B. F., Saha, T. D., Ruan, W. J., Goldstein, R. B., Chou, S. P., Jung, J., & Hasin, D. S. (2016). Epidemiology of DSM-5 drug use disorder: results from the national epidemiologic survey on alcohol and related conditions-III. JAMA Psychiatry, 73(1), 39–47. https://doi.org/10.1001/jamapsychiatry.2015.2132
Gross, M. (2010). Alcoholics anonymous: Still sober after 75 years. American Journal of Public Health, 100(12), 2361–2363. https://doi.org/10.2105/AJPH.2010.199349
Hadland, S. E., Jent, V. A., Alinsky, R. H., Marshall, B. D. L., Mauro, P. M., & Cerda, M. (2020). Opioid use disorder treatment facilities with programs for special populations. American Journal of Preventive Medicine, 59(3), e125–e133. https://doi.org/10.1016/j.amepre.2020.03.022
Hillhouse, M. P., & Fiorentine, R. (2001). 12-step program participation and effectiveness: do gender and ethnic differences exist? Journal of Drug Issues, 31(3), 767–780. https://doi.org/10.1177/002204260103100313
Hoffman, F. (1994). Cultural adaptations of alcoholics anonymous to serve Hispanic populations. The International Journal of the Addictions, 29(4), 445–460. https://doi.org/10.3109/10826089409047392
Kariisa, M., Davis, N. L., Kumar, S., Seth, P., Mattson, C. L., Chowdhury, F., & Jones, C. M. (2022). Vital signs: drug overdose deaths, by selected sociodemographic and social determinants of health characteristics — 25 states and the District of Columbia, 2019–2020. MMWR Morb Mortal Wkly Rep, 71, 940–947. https://doi.org/10.15585/mmwr.mm7129e2
Kelly, J. F., Humphreys, K., & Ferri, M. (2020). Alcoholics anonymous and other 12-step programs for alcohol use disorder. Cochrane Database Syst Rev, 3, CD012880. https://doi.org/10.1002/14651858.CD012880.pub2
Klein, A. A., & Seppala, M. D. (2019). Medication-assisted treatment for opioid use disorder within a 12-step based treatment center: Feasibility and initial results. Journal of Substance Abuse Treatment, 104, 51–63. https://doi.org/10.1016/j.jsat.2019.06.009
Krasnova, A., Diaz, J. E., Philbin, M. M., & Mauro, P. M. (2021). Disparities in substance use disorder treatment use and perceived need by sexual identity and gender among adults in the United States. Drug and Alcohol Dependence, 226, 108828. https://doi.org/10.1016/j.drugalcdep.2021.108828
Krawczyk, N., Negron, T., Nieto, M., Agus, D., & Fingerhood, M. I. (2018). Overcoming medication stigma in peer recovery: A new paradigm. Subst Abus, 39(4), 404–409. https://doi.org/10.1080/08897077.2018.1439798
Krogstad, J. M., Passel, J. S., & Noe-Bustamante, L. (2022). Key facts about U.S. Latinos for National Hispanic Heritage Month. Pew Research Center. https://www.pewresearch.org/fact-tank/2022/09/23/key-facts-about-u-s-latinos-for-national-hispanic-heritage-month/. Accessed 30 Nov 2022.
Lookatch, S. J., Wimberly, A. S., & McKay, J. R. (2019). Effects of social support and 12-step involvement on recovery among people in continuing care for cocaine dependence. Substance Use and Misuse, 54(13), 2144–2155. https://doi.org/10.1080/10826084.2019.1638406
Mantha, S., Mauro, P. M., Mauro, C. M., & Martins, S. S. (2020). State criminal justice policy context and opioid agonist treatment delivery among opioid treatment admissions, 2015. Drug Alcohol Depend, 206, 107654. https://doi.org/10.1016/j.drugalcdep.2019.107654
Mattson, C. L., Tanz, L. J., Quinn, K., Kariisa, M., Patel, P., & Davis, N. L. (2021). Trends and geographic patterns in drug and synthetic opioid overdose deaths - United States, 2013–2019. MMWR Morb Mortal Wkly Rep, 70(6), 202–207. https://doi.org/10.15585/mmwr.mm7006a4
Mauro, P. M., Gutkind, S., Annunziato, E. M., & Samples, H. (2022a). Use of medication for opioid use disorder among US adolescents and adults with need for opioid treatment, 2019. JAMA Netw Open, 5(3), e223821. https://doi.org/10.1001/jamanetworkopen.2022.3821
Mauro, P. M., Kane, J. C., Askari, M. S., Iwamoto, D., & Martins, S. S. (2022b). Mind the gap: Differences in alcohol use screening and discussions among adults comparing Asian American and other racial and ethnic subgroups in the United States, 2015–2019. Alcohol and Alcoholism. https://doi.org/10.1093/alcalc/agac050
Mauro, P. M., Samples, H., Klein, K. S., & Martins, S. S. (2020). Discussing drug use with health care providers is associated with perceived need and receipt of drug treatment among adults in the United States: We Need to Talk. Medical Care, 58(7), 617–624. https://doi.org/10.1097/MLR.0000000000001340
Merlo, J., Chaix, B., Ohlsson, H., Beckman, A., Johnell, K., Hjerpe, P., & Larsen, K. (2006). A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health, 60(4), 290–297. https://doi.org/10.1136/jech.2004.029454
Midgette, G., Caulkins, J. P., & Reuter, P. (2021). Pathways to drug prevalence estimation: synthesizing three comments on triangulation. Addiction, 116(10), 2615–2616. https://doi.org/10.1111/add.15607
Miech, R. A., London, A. S., Wilmoth, J. M., & Koester, S. (2013). The effects of the military’s antidrug policies over the life course: The case of past-year hallucinogen use. Substance Use and Misuse, 48(10), 837–853. https://doi.org/10.3109/10826084.2013.800120
Miller, J. C. (2008). 12-step treatment for alcohol and substance abuse revisited: Best available evidence suggests lack of effectiveness or harm. Int J Ment Health Addiction, 6, 568–576.
Monico, L. B., Gryczynski, J., Mitchell, S. G., Schwartz, R. P., O’Grady, K. E., & Jaffe, J. H. (2015). Buprenorphine treatment and 12-step meeting attendance: Conflicts, compatibilities, and patient outcomes. Journal of Substance Abuse Treatment, 57, 89–95. https://doi.org/10.1016/j.jsat.2015.05.005
Morgan Snell, L., Barnes, A. J., & Cunningham, P. (2020). Epidemiology of substance use disorders: Opioid use disorder epidemic. Oxford University Press. https://doi.org/10.1093/med/9780190920197.003.0001
National Institute on Alcohol Abuse and Alcoholism. (2014). Treatment for Alcohol Problems: Finding and Getting Help. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/treatment-alcohol-problems-finding-and-getting-help
National Institute on Drug Abuse. (2018). Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). National Institute on Drug Abuse; National Institutes of Health; US Department of Health and Human Services. https://www.drugabuse.gov/download/675/principles-drug-addiction-treatment-research-based-guide-third-edition/preface
Nesoff, E. D., Martins, S. S., & Palamar, J. J. (2022). Caution is necessary when estimating treatment need for opioid use disorder using national surveys. American Journal of Public Health, 112(2), 199–201. https://doi.org/10.2105/AJPH.2021.306624
Paquette, K. L., Pannella Winn, L. A., Wilkey, C. M., Ferreira, K. N., & Donegan, L. R. W. (2019). A framework for integrating young peers in recovery into adolescent substance use prevention and early intervention. Addict Behav, 99, 106080. https://doi.org/10.1016/j.addbeh.2019.106080
Pear, V. A., Ponicki, W. R., Gaidus, A., Keyes, K. M., Martins, S. S., Fink, D. S., & Cerdá, M. (2019). Urban-rural variation in the socioeconomic determinants of opioid overdose. Drug and Alcohol Dependence, 195, 66–73. https://doi.org/10.1016/j.drugalcdep.2018.11.024
R Core Team. (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/
Reuter, P., Caulkins, J. P., & Midgette, G. (2021). Heroin use cannot be measured adequately with a general population survey. Addiction, 116(10), 2600–2609. https://doi.org/10.1111/add.15458
StataCorp. (2017). Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC.
Substance Abuse and Mental Health Services Administration. (2003). Results from the 2002 National Survey on Drug Use and Health: National Findings. Office of Applied Studies, NHSDA Series H-22, DHHS Publication No. SMA 03-3836. Rockville, MD.
Substance Abuse and Mental Health Services Administration. (2019a). 2018 National Survey on Drug Use and Health: Methodological summary and definitions. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/
Substance Abuse and Mental Health Services Administration. (2019b). Results from the 2018 National Survey on Drug Use and Health: Detailed Tables. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/
Tomko, C., Olfson, M., & Mojtabai, R. (2022). Gaps and barriers in drug and alcohol treatment following implementation of the affordable care act. Drug and Alcohol Dependence Reports, 5, 100115. https://doi.org/10.1016/j.dadr.2022.100115
Townsend, T., Kline, D., Rivera-Aguirre, A., Bunting, A. M., Mauro, P. M., Marshall, B. D. L., & Cerdá, M. (2022). Racial/ethnic and geographic trends in combined stimulant/opioid overdoses, 2007–2019. American Journal of Epidemiology, 191(4), 599–612. https://doi.org/10.1093/aje/kwab290
Verissimo, A. D. O., & Grella, C. E. (2017). Influence of gender and race/ethnicity on perceived barriers to help-seeking for alcohol or drug problems. Journal of Substance Abuse Treatment, 75, 54–61. https://doi.org/10.1016/j.jsat.2016.12.013
Vogel, E. A., Ly, K., Ramo, D. E., & Satterfield, J. (2020). Strategies to improve treatment utilization for substance use disorders: a systematic review of intervention studies. Drug Alcohol Depend, 212, 108065. https://doi.org/10.1016/j.drugalcdep.2020.108065
Wen, H., Druss, B. G., & Saloner, B. (2020). Self-help groups and medication use in opioid addiction treatment: A national analysis. Health Aff (millwood), 39(5), 740–746. https://doi.org/10.1377/hlthaff.2019.01021
Wilson, N., Kariisa, M., Seth, P., Smith, H., IV., & Davis, N. L. (2020). Drug and opioid-involved overdose deaths - United States, 2017–2018. MMWR Morb Mortal Wkly Rep, 69(11), 290–297. https://doi.org/10.15585/mmwr.mm6911a4
Wu, L. T., Zhu, H., & Swartz, M. S. (2016). Treatment utilization among persons with opioid use disorder in the United States. Drug and Alcohol Dependence, 169, 117–127. https://doi.org/10.1016/j.drugalcdep.2016.10.015
Yang, Y. (2006). Bayesian inference for hierarchical age-period-cohort models of repeated cross-section survey data. Sociological Methodology, 36, 39–74.
Yang, Y., Fu, W. J., & Land, K. C. (2004). A methodological comparison of age-period-cohort models: the intrinsic estimator and conventional generalized linear models. Sociol Methodol, 34, 75–110. https://doi.org/10.1111/j.0081-1750.2004.00148.x
Yang, Y., & Land, K. C. (2008). Age–period–cohort analysis of repeated cross-section surveys fixed or random effects? Sociol Methods Res, 36(3), 297–326.
Yang, Y., & Land, K. C. (2013). Mixed effects models: Hierarchical APC-cross- classified random effects models (HAPC-CCREM), Part I: The Basics. In N. Keiding, B. J. T. Morgan, C. K. Wikle, & P. van der Heijden (Eds.), Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications (pp. 191–230). CRC Press.
Zemore, S. E., Gilbert, P. A., Pinedo, M., Tsutsumi, S., McGeough, B., & Dickerson, D. L. (2021). Racial/ethnic disparities in mutual help group participation for substance use problems. Alcohol Res, 41(1), 03. https://doi.org/10.35946/arcr.v41.1.03
Acknowledgements
The authors would like to thank Erin Annunziato for her assistance formatting the paper.
Funding
This work was supported by the National Institute on Drug Abuse grants K01DA045224 (PI: Mauro) and R01DA048853 (PI: Keyes), the National Institute on Alcohol Abuse and Alcoholism grant R01AA026861 (PI: Keyes), and the National Institute on Mental Health grant T32MH013043 (PI: Keyes). Funding sources had no involvement in the study design or manuscript writing.
Author information
Authors and Affiliations
Contributions
Pia M. Mauro: conceptualization, supervision, writing—original draft preparation. Navdep Kaur: methodology, software, formal analysis, writing—review and editing. Melanie S. Askari: writing—review and editing. Katherine M. Keyes: methodology, supervision, writing—review and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
The RTI institutional review board approved the NSDUH protocol and insured informed consent from all individual participants included in the study (Center for Behavioral Health Statistics and Quality, 2019). Our secondary data analysis used de-identified publicly available data that was not considered human subjects research, and therefore, did not require additional ethical approval beyond what was obtained through the NSDUH informed consent process.
This is an observational study using de-identified public data. The Columbia University Institutional Review Board determined Dr. Pia Mauro’s National Institute on Drug Abuse grant K01DA045224 protocol to be exempt.
Competing Interests
K. Keyes has received compensation for expert witness consultation in product litigation. PM Mauro, N Kaur, and MS Askari declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mauro, P.M., Kaur, N., Askari, M.S. et al. Alcohol or Drug Self-Help Use Among Adults in the United States: Age, Period, and Cohort Effects Between 2002 and 2018. Int J Ment Health Addiction (2023). https://doi.org/10.1007/s11469-023-01012-2
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-023-01012-2