
Abstract
Purpose
Although hemorrhage within pituitary adenomas frequently exacerbates the symptoms, there are many grades of severity. Moreover, the contributing factors for symptom severity are still controversial.
Methods
This retrospective study included 82 patients who underwent transsphenoidal surgery for pituitary adenomas with intratumoral hemorrhage. The grades of preoperative symptoms were classified into group A, asymptomatic or minor symptoms; group B, moderate symptoms sufficient for complain; and group C, severe symptoms disturbing daily life.
Results
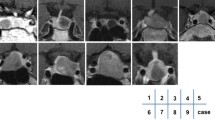
The hemorrhage volume within an adenoma was significantly higher in group C (92.6%) than in groups A (48.6%) and B (58.7%). Both headache and diplopia were dominant in group C, occurring in 72.2% and 27.8% of the patients, respectively. In group C, there was no significant difference in frequency between adenoma extensions into the sphenoid sinus (0%) and involvement of the cavernous sinus of Knosp grade 4 (0%), and extensions into the suprasellar region were not common (38.9%). The most distinctive feature was that “no extrasellar extension” was found only in group C (41.2%), and “multidirectional extension” was not detected in this group (0%). Multiple regression analysis revealed that the most powerful determining factors were the high frequencies of intratumoral hemorrhage and lack of extrasellar and multidirectional extensions.
Conclusion
Rapid volume expansion of a hematoma and lack of extension or unidirectional extension might lead to significant compression of the sellar and surrounding structures. Of note, the integrity of the sellar dura might contribute to the acute onset of symptom manifestations caused by hemorrhage in pituitary adenomas.



Similar content being viewed by others


Abbreviations
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- TSS:
-
Transsphenoidal surgery
- WI:
-
Weighted image
References
Chuang CC, Chen E, Huang YC, Tu PH, Chen YL, Pai PC (2011) Surgical outcome of oculomotor nerve palsy in pituitary adenoma. J Clin Neurosci 18:1463–1468
Fleseriu M, Yedinak C, Campbell C, Delashaw JB (2009) Significant headache improvement after transsphenoidal surgery in patients with small sellar lesions. J Neurosurg 110:354–358
Hayashi Y, Kita D, Iwato M, Fukui I, Oishi M, Tsutsui T, Tachibana O, Nakada M (2016) Significant improvement of intractable headache after transsphenoidal surgery in patients with pituitary adenomas; preoperative neuroradiological evaluation and intraoperative intrasellar pressure measurement. Pituitary 19:175–182
Singh TD, Valizadeh N, Meyer FB, Atkinson JL, Erickson D, Rabinstein AA (2015) Management and outcomes of pituitary apoplexy. J Neurosurg 122:1450–1457
Briet C, Salenave S, Bonneville JF, Laws ER, Chanson P (2015) Pituitary apoplexy. Endocr Rev 36:622–645
Semple PL, de Villiers JC, Bowen RM, Lopes MBS, Laws ER Jr (2006) Pituitary apoplexy: do histological features influence the clinical presentation and outcome? J Neurosurg 104:931–937
Semple PE, Webb MK, de Villers JC, Laws ER Jr (2005) Pituitary apoplexy. Neurosurgery 56:65–73
Briet C, Salenave S, Chanson P (2015) Pituitary apoplexy. Endocrinol Metab Clin North Am 44:199–209
Ogawa Y, Niizuma K, Mugikura S, Tominaga T (2016) Ischemic pituitary adenoma apoplexy-Clinical appearance and prognosis after surgical intervention. Clin Neurol Neurosurg 148:142–146
Randeva HP, Schoebel J, Byrne J, Esiri M, Adams CB, Wass JA (1999) Classical pituitary apoplexy: Clinical features, management and outcomes. Clin Endocrinol 51:181–188
Semple LE, Jane JA Jr, Laws ER Jr (2007) Clinical relevance of precipitating factors in pituitary apoplexy. Neurosurgery 61:956–962
Glezer A, Bronstein MD (2015) Pituitary apoplexy: pathophysiology, diagnosis and management. Arch Endocrinol Metab 59:259–264
Koutourousiou M, Gardner PA, Fernandez-Miranda JC, Paluzzi A, Wang EW, Snyderman CH (2013) Endoscopic endonasal surgery for giant pituitary adenomas: advantages and limitations. J Neurosurg 118:621–631
Zaidi HA, Cote DJ, Burke WT, Castlen JP, Bi WL, Laws ER Jr, Dunn IF (2016) Time course of symptomatic recovery after endoscopic transsphenoidal surgery for pituitary adenoma apoplexy in the modern era. World Neurosurg 96:434–439
Liu JK, Couldwell WT (2006) Pituitary Apoplexy in the magnetic resonance imaging era: clinical significance of sphenoid sinus mucosal thickening. J Neurosurg 104:892–898
Piotin M, Tampieri D, Rufenachr DA, Mohr G, Garant M, Del Carpio R (1999) The various MRI patterns of pituitary apoplexy. Eur Radiol 9:918–923
Nomura M, Tachibana O, Yamashima T, Yamashita J, Suzuki M (2002) MRI evaluation of the diaphragmal opening: using MRI parallel to the transsphenoidal surgical approach. J Clin Neurosci 9:175–177
Arita K, Tominaga A, Sugiyama K, Eguchi K, Iida K, Sumida M, Migita K, Kurisu K (2006) Natural course of incidentally found nonfunctioning pituitary adenoma, with special reference to pituitary apoplexy during follow-up examination. J Neurosurg 104:884–891
Giammattei L, Mantovani G, Carrabba G, Ferrero S, Di Cristofori A, Verrua E, Guastella C, Pignataro L, Rampini P, Minichiello M, Locatelli M (2016) Pituitary apoplexy: considerations on a single center experience and review of the literature. J Endocrinol Invest 39:739–746
Reid RL, Qulgley M, Yen SS (1985) Pituitary apoplexy. Arch Neurol 42:712–719
Gondim JA, Tella OI Jr, Schops M (2006) Intrasellar pressure and tumor volume in pituitary tumor. Arq Neuropsiquiatr 64:971–975
Ramakrishnan VR, Suh JD, Lee JY, O’Malley BW Jr, Grady MS, Palmer JN (2013) Sphenoid sinus anatomy and suprasellar extension of pituitary tumors. J Neurosurg 119:669–674
Zada G, Agarwalla PK, Mukundan S Jr, Dunn I, Golby AJ, Laws ER Jr (2011) The neurosurgical anatomy of the sphenoid sinus and sellar floor in endoscopic transsphenoidal surgery. J Neurosurg 114:1319–1330
Zayour DH, Selman WR, Arafah BM (2004) Extreme elevation of intrasellar pressure in patients with pituitary tumor apoplexy: relation to pituitary function. J Clin Endocrinol Metab 89:5649–5654
Destrieux C, Kakou MK, Velut S, Lefrancq T, Jan M (1998) Microanatomy of the hypophyseal fossa boundaries. J Neurosurg 88:743–752
Levy MJ, Jager HR, Powell M, Marthau MS, Meeran K, Goadsby PJ (2004) Pituitary volume and headache: size is not everything. Arch Neurol 61:721–725
Jho DH, Biller BMK, Agarwalla PK, Swearingen B (2014) Pituitary apoplexy: large surgical series with grading system. World Neurosurg 82:781–790
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have no conflict of interests.
Rights and permissions
About this article

Cite this article
Hayashi, Y., Sasagawa, Y., Kita, D. et al. Contribution of sellar dura integrity to symptom manifestation in pituitary adenomas with intratumoral hemorrhage. Pituitary 20, 531–538 (2017). https://doi.org/10.1007/s11102-017-0814-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-017-0814-x