
Abstract
Almost 7 % of breast cancers are diagnosed among women age 40 years and younger in Western populations. Clinical outcomes among young women are worse. Early age-of-onset increases the risk of contralateral breast cancer, local and distant recurrence, and subsequent mortality. Breast cancers in young women (BCYW) are more likely to present with triple-negative (TNBC), TP53-positive, and HER-2 over-expressing tumors than among older women. However, despite these known differences in breast cancer outcomes and tumor subtypes, there is limited understanding of the basic biology, epidemiology, and optimal therapeutic strategies for BCYW. Several modifiable lifestyle factors associated with reduced risk of develo** breast cancer have also been implicated in improved prognosis among breast cancer survivors of all ages. Given the treatment-related toxicities and the extended window for late effects, long-term lifestyle modifications potentially offer significant benefits to BCYW. In this review, we propose a model identifying three main areas of lifestyle factors (energy imbalance, inflammation, and dietary nutrient adequacy) that may influence survival in BCYW. In addition, we provide a summary of mechanisms of action and a synthesis of previous research on each of these topics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common cancer among women in Western populations with a lifetime cumulative incidence probability of one in nine [1]. Approximately 6.6 % of breast cancers are diagnosed among women age 40 and younger. The average risk of develo** breast cancer by age 40 is one in 173 [1, 2]. Of all cancers diagnosed among women by age 40 years, 40 % are breast cancers. Traditionally, breast cancers in young women (BCYW) have been thought to be etiologically driven primarily by genetic/hereditary factors [3]. BCYW are more likely to be associated with increased familial risk, but only a relatively small proportion of cases (<10 %) are attributable to inherited germline variations in the known familial breast cancer risk genes (BRCA1/BRCA2) [4, 5] and are highest in those women with very strong family histories of breast or ovarian cancer [5]. Other genomic factors, including mutations in tumor suppressor and oncogenes, copy number variation, and epigenetics, are likely implicated in cancer initiation and progression among young women. However, these alterations do not fully explain carcinogenesis and subsequent progression among young women.
There are four clinically relevant breast cancer phenotypes currently recognized [6]: luminal A (ER+, PR+, HER2−, Ki67 low), luminal B (ER+, HER2−, PR−, or Ki67 high), triple-negative breast cancer (TNBC; ER−, PR−, and HER2−), and HER2 over-expressing tumors (HER2+). The TNBC and HER2+ subtypes are the most aggressive forms of breast cancer and are over-represented in BCYW [7–9]. Approximately 26 % of BCYW are TNBC compared to 12 % overall [10, 11]. Next-generation sequencing of TNBC has suggested that actionable mutations occur in only a small subset (<20 %) of these cancers [12] and do not completely predict survival [13]. Therefore, non-genomic factors, including lifestyle and other epidemiologic factors, may significantly impact recurrence and survival in BCYW.
Here we present a review of the epidemiologic literature on the associations between lifestyle factors, recurrence, and survival for BCYW, defined as a breast cancer diagnosed by age 40 years. The aim of this review is to provide an overview of the associations observed to date among BCYW and how they compare to those that have been observed in the general population of breast cancer survivors. In doing so, we have also aimed to identify gaps in the literature where additional research is needed in this population. BCYW is considered to be distinct from pre-menopausal breast cancer (average age at menopause among North American women is 51 years) [14, 15]. However, since there is limited epidemiologic research specifically examining the effect of candidate risk factors on BCYW, we have included studies on pre-menopausal cases if no BCYW-specific data were available. We propose a biologic model for the impact of selected lifestyle factors on prognosis in BCYW (Fig. 1). In doing so, we provide a conceptual model for the inter-play between these factors and their possible role in cancer progression. We have focused our review on modifiable factors for which, despite evidence for an impact among the general population of breast cancer patients, the research specifically addressing BCYW is limited and needs further investigation.

Proposed biologic model depicting how multiple lifestyle risk factors may influence breast cancer prognosis through a pro-inflammatory state including important exposures, pathways, and impact on the candidate biologic mediators
Green arrows indicate potentially beneficial factors; red arrows indicate potentially detrimental factors. (Color figure online)
A conceptual model for lifestyle factors in breast cancer prognosis among young women
Despite the acknowledged differences in clinical outcomes, tumor subtypes and treatment approaches in young women compared with older women, specific insights into the basic biology, epidemiology, and optimal therapeutic strategies for BCYW are relatively sparse. Several modifiable factors that have been associated with reduced risk of develo** breast cancer may also be implicated in improved prognosis. Given the treatment-related toxicities, and the extended window for late effects, including cardiotoxic effects of systemic and radiation therapy [16–19], bone health issues [20], and elevated risk of second primary cancers [21, 22], these long-term lifestyle factors potentially offer particularly significant benefits in BCYW (Fig. 2). We propose a biologic model to identify three main lifestyle-related factors in BCYW prognosis research (Fig. 1). We hypothesize that positive energy balance (obesity and physical inactivity), specific dietary factors, and inflammatory triggers contribute to a pro-inflammatory state that is conducive to increased risk of progression, recurrence, and decreased survival after a breast cancer diagnosis in young women. The extended period of potential post-diagnostic survival and the lower burden of competing mortality risks in young women provide a context in which lifestyle modification could have a substantial impact on long-term mortality and morbidity.

Potential period for lifestyle modification to impact outcomes in breast cancer patients according to age at first diagnosis
Compared to women at the median age of diagnosis, young women (<40 years) have approximately twice the duration of post-diagnostic/post-treatment life during which their risk of disease and treatment-related consequences are elevated. The opportunity to mitigate these effects through lifestyle modification is much greater for younger women
All of the factors included in our review affect the hypothesized pro-inflammatory state, and our conceptual model seeks to integrate the impact of lifestyle factors that have been implicated in modifying clinical outcomes following a diagnosis of breast cancer (Fig. 1). The contributors to a pro-inflammatory state (red labels) and the potentially beneficial impacts (green labels) of diet, physical activity, sleep, and non-steroidal anti-inflammatory drugs (NSAIDs) are included. The conceptual model provides a framework for this review as well as a roadmap for future research to integrate diet, nutrient levels, shared signaling between obesity and inflammation, and potential lifestyle interventions. Each of the three main areas is reviewed in the sections below.
Clinical context
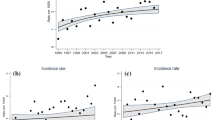
The cumulative incidence of breast cancer rises exponentially until age 40 years and then rises more linearly with age [23]. Incidence rates among young women vary by geographic region, and ethnicity with the highest rates reported among Western populations [24, 25] and among black women [26]. Clinical outcomes of BCYW are relatively poor compared to older women diagnosed with breast cancer. Early age-of-onset increases the risk of contralateral breast cancer [27], local [28–30], and distant recurrence [23]. The European Organisation for Research and Treatment of Cancer (EORTC) trials showed a hazard ratio (HR) of 2.8 (95 % confidence interval [CI] 1.4–5.6) for local recurrence in patients <35 years compared to those >50 [28]. Voogd et al. [31] examined two large clinical trials of women with stage I–II breast cancer and reported a dramatically increased risk (HR = 9.2, 95 % CI 3.7–23.0) of local recurrence in women <35 years of age compared to women age ≥65 years.
Young age at diagnosis is associated with reduced survival, even after controlling for differences in the distribution of prognostic features between older and younger women with breast cancer [9, 32–35]. A retrospective evaluation of outcomes among more than 200,000 women with breast cancer in the SEER database found that women aged <40 were 39 % more likely to die of their disease when compared to those aged ≥40 (HR = 1.39, 95 % CI 1.34–1.45). The largest differences in mortality were seen among women with early-stage disease. Women <40 were more likely to die of stage I or II cancers than older women (44 and 9 %, respectively) [36]. Similar associations between reduced survival in younger, early-stage patients have been observed in other cohorts of BCYW [37, 38]. Furthermore, survival rates were comparatively lower across all histologic subtypes and stages for women <40 years of age [39]. According to SEER data, for cases diagnosed between 1975 and 2000, the 5-year relative survival rate was 84–86 % overall among women aged 45–80 years, but 80, 76, 72, and 75 % among women aged 35–39, 30–34, 25–29, and 20–25 years, respectively [40].
The absolute benefits of treatment, whether local or systemic, tend to be larger in younger women because of the higher proportion of aggressive disease [41, 42], but few trials have specifically evaluated treatment selection for younger women; the median age of patients in most randomized controlled trials (RCTs) is about 55 years [41–45]. Younger patients tend to have fewer comorbidities and better tolerance of treatment toxicities and, consequently, are often treated more aggressively. Most women are treated with breast-conserving surgery (BCS) followed by radiation therapy (RT) [41, 44, 46–49], but population-based analyses have shown higher rates of mastectomy for BCYW compared to older women with similar stage disease [46, 47]. Residual concerns regarding higher overall recurrence rates, a longer potential life span requiring ongoing follow-up/surveillance, and the risk of radiation-induced second primary tumors in young women [50] may contribute to provider recommendations or patient preference for mastectomy in spite of evidence that outcomes following BCS + RT of mastectomy are equivalent, even among BCYW [31, 51–54]. The 2015 National Comprehensive Cancer Network (NCCN) breast cancer management guidelines no longer cite young age (<35 years) as an indication for mastectomy, as was the case in the earlier 1997 NCCN guidelines [55]. However, young women (<40 years) were almost four times more likely to receive bilateral mastectomy than women aged 50–64 years (OR 3.81; 95 % CIs 3.55–4.08) [56].
Younger women also tend to receive more intensive radiation and systemic therapy despite an international expert panel advocating that young age alone should not be sufficient justification for aggressive therapy [15]. Whole breast RT plus a supplementary “boost” dose to the primary site is routinely administered following BCS in younger women [57] because RCTs have shown that they experience the largest absolute improvements in local control [58]. The majority of young women with breast cancer are candidates for chemotherapy and anti-estrogen therapy (for ER-positive disease, usually with tamoxifen) for at least 5 years [3, 15, 42]. Young women increasingly receive neoadjuvant chemotherapy prior to definitive local therapy to downstage disease and, in some cases, to facilitate BCS where mastectomy might have otherwise been indicated [57]. In addition, the tumor subtypes most commonly found in young women are more likely to respond to neoadjuvant chemotherapy and provide an in vivo evaluation of response to systemic therapy. The higher frequency of HER2 over-expression, TNBC, and BRCA mutations in BCYW results in these women being offered novel combinations of systemic therapeutic agents more frequently than older women, particularly within clinical trials.
Lifestyle factors
Positive energy balance
Obesity
Positive energy balance, as a consequence of excess caloric intake and/or insufficient energy expenditure, results in increased adipose tissue leading to overweight and/or obesity. Both obesity [59] and physical inactivity [60] increase the risk of breast cancer development in older women and progression at all ages. Increased risks for overall mortality and breast cancer-specific mortality associated with increasing body mass index (BMI; e.g., HR = 1.41, 95 % CI 1.29–1.53) [61] or waist–hip ratio (HR = 1.31, 95 % CI 1.08–1.58) were reported in a recent meta-analysis [62]. Larger effect sizes for breast cancer mortality are associated with obesity among pre-menopausal (HR = 1.75, 95 % CI 1.26–2.41) compared to post-menopausal women (HR = 1.34, 95 % CI 1.18–1.53) [61].
One of the biologic mechanisms through which obesity could affect cancer survival is by altering the insulin resistance (IR) pathway [63]. Homeostatic model assessment (HOMA) is a method for assessing β-cell function and IR from basal (fasting) glucose and insulin or C-peptide concentrations [64]. Although no data exist specifically for young women, increasing HOMA-IR has been associated with a positive trend for breast cancer recurrence in ER-/PR-negative patients (p for trend = 0.087) and an inverse trend in ER-/PR-positive patients (p for trend = 0.081) among a general population of breast cancer patients [65]. In a multiethnic cohort of 527 women with breast cancer [Health, Eating, Activity, and Lifestyle (HEAL) Study], increasing HOMA scores were associated with reduced breast cancer survival (HR = 1.12, 95 % CI 1.05–1.20) [1). Many of the studies investigating the role of dietary fat intake on breast cancer outcomes have reported associations that fail to reach statistical significance, and the point estimates are too inconsistent to provide a clear consensus [139]. However, the lack of published research regarding the role of fat intake in BCYW combined with both the potential beneficial and detrimental impacts of fat subtypes, presents an opportunity to address the impact of fat intake on post-diagnostic outcomes in BCYW.
Vitamin D
Vitamin D is mostly synthesized in the skin by ultraviolet B radiation (only in the summer at higher latitudes), while dietary intake and supplements also contribute to overall vitamin D status, particularly in the winter in northern populations. The evidence to support an inverse association between breast cancer risk and vitamin D status is complex and uncertain [141], but there is increasing evidence that vitamin D status may be an important factor in breast cancer survival [142]. There are several plausible mechanisms whereby vitamin D may influence the phenotype of the primary tumor and potentially improve outcomes. Vitamin D exhibits pro-differentiation and anti-proliferative properties [143]. Accumulating evidence implicates suboptimal vitamin D status in the development of inflammatory and immunological conditions [144], compatible with the observed immunosuppressive and anti-inflammatory activity of 1,25-dihydroxyvitamin D, the active metabolite of vitamin D [145]. No previous studies have examined the impact of vitamin D status in BCYW, and the impact on pre- versus post-menopausal women has been inconsistent. However, a few studies have identified differences in outcome between tumor phenotypes in pre- and post-menopausal women associated with vitamin D status. Goodwin et al. [142] reported that low serum 25-hydroxyvitamin D concentration (<50 nmol/L) was associated with higher tumor grade at diagnosis, increased risk of distant recurrence (HR = 1.94, 95 % CI 1.16–3.25), and increased risk of breast cancer-specific death (HR = 1.73, 95 % CI 1.05–2.86) compared with patients with levels >72 nmol/L. Similarly, Yao et al. [146] reported that low vitamin D status was associated with the occurrence of higher-grade tumors in pre-menopausal women only. Peppone et al. [147] observed an increased proportion of ER-negative tumors in the vitamin D-deficient group (<20 ng/mL) compared to patients with higher levels. Not all studies have suggested higher serum vitamin D post-diagnosis is associated with better outcomes [148, 149]. These conflicting results are partly attributable to insufficient statistical power, non-population-based sampling, and suboptimal exposure assessment.
Phytoestrogens
The two main classes of phytoestrogens (plant compounds with non-steroidal estrogen-like structures and activities) are isoflavones and lignans. Isoflavones are found primarily in soy foods, while lignans are found in low concentrations in fiber-rich foods such as grains, legumes, seeds, fruits/vegetables, and in high concentration in flaxseeds [150]. Many supplements also contain high concentrations of isoflavones and lignans [151]. For over a decade, researchers have reported that dietary phytoestrogen intake is associated with reduced breast cancer risk, possibly due to demonstrated beneficial effects on proliferation, apoptosis, angiogenesis, as well as estrogen receptor mediated and other activities, including a range of anti-inflammatory effects [152–158]. However, only recently has the association between post-diagnostic phytoestrogen intake with breast cancer recurrence and mortality been investigated. Overall, most studies suggested that post-diagnosis intake improved prognosis [159–164], but findings stratified by menopausal status, if reported, have been inconsistent [159, 160, 162]. Most of the six prognostic studies included predominately post-menopausal women [159, 161, 163, 164], leaving a paucity of information regarding phytoestrogen intake and prognosis among BCYM. The largest soy/isoflavone study found a significantly reduced risk of recurrence and breast cancer mortality combined (HR = 0.77, 95 % CI 0.60–0.98), with no difference by menopausal status. Two meta-analyses reported a statistically significantly reduced risk of recurrence that was restricted to post-menopausal women [173], contrasting evidence also supports that high folate levels may promote cancer progression and actually increase the risk of some cancers, including breast cancer [173–175]. High folate intake may increase breast cancer risk by promoting the progression of existing (pre-)neoplastic lesions, by expanding the breast stem cell population or by preventing terminal differentiation in ductal cells [173, 175, 176]. Since a high proportion of cancer survivors consume supplements containing folic acid [177–179], the role of folate in breast cancer prognosis needs clarification.
To date, eight studies have evaluated the relationship between dietary or plasma folate levels and survival after breast cancer and findings have been inconsistent [133, 180–186]. Four studies found no association [133, 181, 182, 185], three reported a significant inverse relationship [180, 183, 184], and a recent study reported a harmful effect of high folate status on breast cancer prognosis, specifically in ER−/PR− tumors [186]. However, these studies included mostly post-menopausal women and none evaluated the impact of folate in patients diagnosed at a young age. It is also unknown whether the relationship between folate status and survival varies by folate receptor alpha (FRα) expression of the tumor. Positivity for FRα has previously been associated with the occurrence of TNBC and poor prognosis [187]. Interestingly, FRβ was recently identified as a marker for a pro-inflammatory subset of monocytes [188]. Both elevated folate and folate insufficiency may induce inflammatory processes [189].
Alcohol
The role of alcohol consumption in breast cancer development and progression generates great public interest and scientific debate. The exact mechanism of action remains to be elucidated, but alcohol is proposed to cause tissue damage and cancer progression is through the formation of acetaldehyde [190]. Acetaldehyde is the primary product of ethanol oxidation, and its rate of formation is determined by the rate of nicotinamide adenine dinucleotide oxidation through mitochondrial electron transport [191]. Inefficient metabolism or excretion of ethanol and acetaldehyde results in the formation of reactive oxygen species, notably superoxide [192], which affects carcinogenesis through an inflammatory response.
The association between alcohol consumption and prognosis has not been directly evaluated in BCYW. However, a recent meta-analysis of prospective cohort data showed that for pre-menopausal women, high levels of alcohol consumption were associated with increased risk of breast cancer recurrence (HR = 1.52, 95 % CI 1.21–1.90) [136]. Another meta-analysis reported a small reduction in all-cause mortality associated with moderate consumption in ER+ patients and a reduction in breast cancer-specific mortality with moderate consumption in ER-negative breast cancer [193]. The associations overall and across relevant subgroups require additional study because of the high prevalence of the exposure among young women in western populations (54.6 % among women 18–44 in the USA) [194].
Conclusions and strategies for additional research
Given the high rates of recurrence and poorer survival in BCYW, there is an urgent need to optimize lifestyle advice to improve outcomes for these women. Modifiable lifestyle factors offer an opportunity to complement conventional therapies provided to these women. The majority of the factors included in this review show common etiologic links in the progression of breast cancer through altered pathways ultimately leading to a pro-inflammatory state. We acknowledge that the list of factors is not exhaustive; however, the aim of this review is to provide an integrated view of the inter-relationship between the most promising candidate modifiable factors. In doing so, we provide a conceptual model for the inter-play between factors and their possible contributions to cancer progression and survival. This literature review has highlighted the paucity of data on the effect of these modifiable factors on breast cancer prognosis among young women. We propose that the potential for an impact on reducing recurrence and improving survival may be considerable. Additional research on this area will provide directions for lifestyle and clinical interventions that support beneficial behavioral change to improve outcomes in young women diagnosed with breast cancer. Future investigations should aim to maximize the integration of factors so that the relative impacts of multiple lifestyle factors can be assessed both independently and in combination. Furthermore, molecular and genetic markers may help to determine potentially relevant subgroups likely to experience maximal or minimal beneficial impact. Integrated study designs with appropriate biospecimen collections will support the assessment of the relative contributions of these exposures to the pathways proposed in our biologic model focused on survival in BCYW.
References
Canadian Cancer Society/National Cancer Institute of Canada (2015) Canadian Cancer Statistics 2015. Toronto, Canada
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127:2893–2917
Narod SA (2012) Breast cancer in young women. Nat Rev Clin Oncol 9:460–470
Peto J, Collins N, Barfoot R et al (1999) Prevalence of BRCA1 and BRCA2 gene mutations in patients with early-onset breast cancer. J Natl Cancer Inst 91:943–949
Malone KE, Daling JR, Neal C et al (2000) Frequency of BRCA1/BRCA2 mutations in a population-based sample of young breast carcinoma cases. Cancer 88:1393–1402
Sorlie T, Perou CM, Tibshirani R et al (2001) Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA 98:10869–10874
Azim HA Jr, Michiels S, Bedard PL et al (2012) Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin Cancer Res 18:1341–1351
Anders CK, Hsu DS, Broadwater G et al (2008) Young age at diagnosis correlates with worse prognosis and defines a subset of breast cancers with shared patterns of gene expression. J Clin Oncol 26:3324–3330
Keegan TH, DeRouen MC, Press DJ, Kurian AW, Clarke CA (2012) Occurrence of breast cancer subtypes in adolescent and young adult women. Breast Cancer Res 14:R55
Howlader N, Altekruse SF, Li CI et al (2014) US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. doi:10.1093/jnci/dju055
Lund MJ, Butler EN, Hair BY et al (2010) Age/race differences in HER2 testing and in incidence rates for breast cancer triple subtypes: a population-based study and first report. Cancer 116:2549–2559
Shah SP, Roth A, Goya R et al (2012) The clonal and mutational evolution spectrum of primary triple-negative breast cancers. Nature 486:395–399
Cerami E, Gao J, Dogrusoz U et al (2012) The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov 2:401–404
Cheung AM, Chaudhry R, Kapral M, Jackevicius C, Robinson G (2004) Perimenopausal and postmenopausal health. BMC Womens Health 4(Suppl 1):S23
Partridge AH, Pagani O, Abulkhair O et al (2014) First international consensus guidelines for breast cancer in young women (BCY1). Breast 23:209–220
Agrawal S (2014) Late effects of cancer treatment in breast cancer survivors. South Asian J Cancer 3:112–115
Kaufman EL, Jacobson JS, Hershman DL, Desai M, Neugut AI (2008) Effect of breast cancer radiotherapy and cigarette smoking on risk of second primary lung cancer. J Clin Oncol 26:392–398
Darby SC, Ewertz M, McGale P et al (2013) Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med 368:987–998
Bird BR, Swain SM (2008) Cardiac toxicity in breast cancer survivors: review of potential cardiac problems. Clin Cancer Res 14:14–24
Peppone LJ, Mustian KM, Rosier RN et al (2014) Bone health issues in breast cancer survivors: a Medicare Current Beneficiary Survey (MCBS) study. Support Care Cancer 22:245–251
Soerjomataram I, Louwman WJ, Lemmens VE, de Vries E, Klokman WJ, Coebergh JW (2005) Risks of second primary breast and urogenital cancer following female breast cancer in the south of The Netherlands, 1972–2001. Eur J Cancer 41:2331–2337
Rubino C, de Vathaire F, Diallo I, Shamsaldin A, Le MG (2000) Increased risk of second cancers following breast cancer: role of the initial treatment. Breast Cancer Res Treat 61:183–195
Anders CK, Johnson R, Litton J, Phillips M, Bleyer A (2009) Breast cancer before age 40 years. Semin Oncol 36:237–249
Assi HA, Khoury KE, Dbouk H, Khalil LE, Mouhieddine TH, El Saghir NS (2013) Epidemiology and prognosis of breast cancer in young women. J Thorac Dis 5(Suppl 1):S2–S8
Althuis MD, Brogan DD, Coates RJ et al (2003) Breast cancers among very young premenopausal women (United States). Cancer Causes Control 14:151–160
Shavers VL, Harlan LC, Stevens JL (2003) Racial/ethnic variation in clinical presentation, treatment, and survival among breast cancer patients under age 35. Cancer 97:134–147
Fourquet A, Campana F, Zafrani B et al (1989) Prognostic factors of breast recurrence in the conservative management of early breast cancer: a 25-year follow-up. Int J Radiat Oncol Biol Phys 17:719–725
de Bock GH, van der Hage JA, Putter H, Bonnema J, Bartelink H, van de Velde CJ (2006) Isolated loco-regional recurrence of breast cancer is more common in young patients and following breast conserving therapy: long-term results of European Organisation for Research and Treatment of Cancer studies. Eur J Cancer 42:351–356
Wapnir IL, Anderson SJ, Mamounas EP et al (2006) Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in five National Surgical Adjuvant Breast and Bowel Project node-positive adjuvant breast cancer trials. J Clin Oncol 24:2028–2037
Coulombe G, Tyldesley S, Speers C et al (2007) Is mastectomy superior to breast-conserving treatment for young women? Int J Radiat Oncol Biol Phys 67:1282–1290
Voogd AC, Nielsen M, Peterse JL et al (2001) Differences in risk factors for local and distant recurrence after breast-conserving therapy or mastectomy for stage I and II breast cancer: pooled results of two large European randomized trials. J Clin Oncol 19:1688–1697
Bharat A, Aft RL, Gao F, Margenthaler JA (2009) Patient and tumor characteristics associated with increased mortality in young women (≤40 years) with breast cancer. J Surg Oncol 100:248–251
Fredholm H, Eaker S, Frisell J, Holmberg L, Fredriksson I, Lindman H (2009) Breast cancer in young women: poor survival despite intensive treatment. PLoS ONE 4:A38–A46
Tichy JR, Lim E, Anders CK (2013) Breast cancer in adolescents and young adults: a review with a focus on biology. J Natl Compr Cancer Netw 11:1060–1069
Narod SA (2010) BRCA mutations in the management of breast cancer: the state of the art. Nat Rev Clin Oncol 7:702–707
Gnerlich JL, Deshpande AD, Jeffe DB, Sweet A, White N, Margenthaler JA (2009) Elevated breast cancer mortality in women younger than age 40 years compared with older women is attributed to poorer survival in early-stage disease. J Am Coll Surg 208:341–347
Theriault RL, Litton JK, Mittendorf EA et al (2011) Age and survival estimates in patients who have node-negative T1ab breast cancer by breast cancer subtype. Clin Breast Cancer 11:325–331
Christiansen P, Bjerre K, Ejlertsen B et al (2011) Mortality rates among early-stage hormone receptor-positive breast cancer patients: a population-based cohort study in Denmark. J Natl Cancer Inst 103:1363–1372
Bleyer A, Barr R, Hayes-Lattin B et al (2008) The distinctive biology of cancer in adolescents and young adults. Nat Rev Cancer 8:288–298
Bleyer A, O’leary M, Barr R, Ries LAG (eds) (2006) Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. National Cancer Institute, NIH, Bethesda
Early Breast Cancer Trialists’ Collaborative Group, Darby S, McGale P et al (2011) Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 378:1707–1716
Early Breast Cancer Trialists’ Collaborative Group, Peto R, Davies C et al (2012) Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 379:432–444
Early Breast Cancer Trialists’ Collaborative Group, Davies C, Godwin J et al (2011) Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet 378:771–784
Clarke M, Collins R, Darby S et al (2005) Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet 366:2087–2106
McGale P, Taylor C, Correa C et al (2014) Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 383:2127–2135
Gaudette LA, Gao RN, Spence A, Shi F, Johansen H, Olivotto IA (2004) Declining use of mastectomy for invasive breast cancer in Canada, 1981–2000. Can J Public Health 95:336–340
Agarwal S, Pappas L, Neumayer L, Kokeny K, Agarwal J (2014) Effect of breast conservation therapy vs mastectomy on disease-specific survival for early-stage breast cancer. JAMA Surg 149:267–274
Fisher B, Anderson S, Bryant J et al (2002) Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 347:1233–1241
Veronesi U, Cascinelli N, Mariani L et al (2002) Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 347:1227–1232
Grantzau T, Mellemkjaer L, Overgaard J (2013) Second primary cancers after adjuvant radiotherapy in early breast cancer patients: a national population based study under the Danish Breast Cancer Cooperative Group (DBCG). Radiother Oncol 106:42–49
Cao JQ, Truong PT, Olivotto IA et al (2014) Should women younger than 40 years of age with invasive breast cancer have a mastectomy? 15-year outcomes in a population-based cohort. Int J Radiat Oncol Biol Phys 90:509–517
Gentilini O, Botteri E, Rotmensz N et al (2010) Breast-conserving surgery in 201 very young patients (<35 years). Breast 19:55–58
Mahmood U, Morris C, Neuner G et al (2012) Similar survival with breast conservation therapy or mastectomy in the management of young women with early-stage breast cancer. Int J Radiat Oncol Biol Phys 83:1387–1393
Frandsen J, Ly D, Cannon G et al (2015) In the modern treatment era, Is breast conservation equivalent to mastectomy in women younger than 40 years of age? A multi-institution study. Int J Radiat Oncol Biol Phys 93:1096–1103
National Comprehensive Cancer Network (2015) Local management of breast cancer. Version 1
Kurian AW, Lichtensztajn DY, Keegan THM, Nelson DO, Clarke CA, Gomez SL (2014) Use of and mortality after bilateral mastectomy compared with other surgical treatments for breast cancer in California, 1998–2011. J Am Med Assoc 312:902–914
Lyman GH, Temin S, Edge SB et al (2014) Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 32:1365–1383
Bartelink H, Maingon P, Poortmans P et al (2015) Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lancet Oncol 16:47–56
Demark-Wahnefried W, Platz EA, Ligibel JA et al (2012) The role of obesity in cancer survival and recurrence. Cancer Epidemiol Biomark Prev 21:1244–1259
Friedenreich CM (2010) The role of physical activity in breast cancer etiology. Semin Oncol 37:297–302
Chan DS, Vieira AR, Aune D et al (2014) Body mass index and survival in women with breast cancer-systematic literature review and meta-analysis of 82 follow-up studies. Ann Oncol 25:1901–1914
Protani M, Coory M, Martin JH (2010) Effect of obesity on survival of women with breast cancer: systematic review and meta-analysis. Breast Cancer Res Treat 123:627–635
Ballard-Barbash R, Friedenreich CM, Courneya KS, Siddiqi SM, McTiernan A, Alfano CM (2012) Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst 104:815–840
Wallace TM, Levy JC, Matthews DR (2004) Use and abuse of HOMA modeling. Diabetes Care 27:1487–1495
Oh SW, Park CY, Lee ES et al (2011) Adipokines, insulin resistance, metabolic syndrome, and breast cancer recurrence: a cohort study. Breast Cancer Res 13:R34
Duggan C, Irwin ML, **ao L et al (2011) Associations of insulin resistance and adiponectin with mortality in women with breast cancer. J Clin Oncol 29:32–39
Weyer C, Funahashi T, Tanaka S et al (2001) Hypoadiponectinemia in obesity and type 2 diabetes: close association with insulin resistance and hyperinsulinemia. J Clin Endocrinol Metab 86:1930–1935
Arita Y, Kihara S, Ouchi N et al (1999) Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem Biophys Res Commun 257:79–83
Vona-Davis L, Howard-McNatt M, Rose DP (2007) Adiposity, type 2 diabetes and the metabolic syndrome in breast cancer. Obes Rev 8:395–408
Vona-Davis L, Rose DP (2007) Adipokines as endocrine, paracrine, and autocrine factors in breast cancer risk and progression. Endocr Relat Cancer 14:189–206
Tworoger SS, Eliassen AH, Kelesidis T et al (2007) Plasma adiponectin concentrations and risk of incident breast cancer. J Clin Endocrinol Metab 92:1510–1516
Tworoger SS, Mantzoros C, Hankinson SE (2007) Relationship of plasma adiponectin with sex hormone and insulin-like growth factor levels. Obesity (Silver Spring) 15:2217–2224
Grossmann ME, Nkhata KJ, Mizuno NK, Ray A, Cleary MP (2008) Effects of adiponectin on breast cancer cell growth and signaling. Br J Cancer 98:370–379
Grossmann ME, Ray A, Dogan S, Mizuno NK, Cleary MP (2008) Balance of adiponectin and leptin modulates breast cancer cell growth. Cell Res 18:1154–1156
Parekh N, Okada T, Lu-Yao GL (2009) Obesity, insulin resistance, and cancer prognosis: implications for practice for providing care among cancer survivors. J Am Diet Assoc 109:1346–1353
Grossmann ME, Ray A, Nkhata KJ et al (2010) Obesity and breast cancer: status of leptin and adiponectin in pathological processes. Cancer Metastasis Rev 29:641–653
Ye JJ, Jia J, Dong SJ et al (2014) Circulating adiponectin levels and the risk of breast cancer: a meta-analysis. Eur J Cancer Prev 23:158–165
Ellsworth RE, Valente AL, Shriver CD, Bittman B, Ellsworth DL (2012) Impact of lifestyle factors on prognosis among breast cancer survivors in the USA. Expert Rev Pharmacoecon Outcomes Res 12:451–464
Enger SM, Bernstein L (2004) Exercise activity, body size and premenopausal breast cancer survival. Br J Cancer 90:2138–2141
Abrahamson PE, Gammon MD, Lund MJ et al (2006) Recreational physical activity and survival among young women with breast cancer. Cancer 107:1777–1785
Beasley JM, Kwan ML, Chen WY et al (2012) Meeting the physical activity guidelines and survival after breast cancer: findings from the after breast cancer pooling project. Breast Cancer Res Treat 131:637–643
Lynch BM, Dunstan DW, Healy GN, Winkler E, Eakin E, Owen N (2010) Objectively measured physical activity and sedentary time of breast cancer survivors, and associations with adiposity: findings from NHANES (2003–2006). Cancer Causes Control 21:283–288
Courneya KS, Segal RJ, McKenzie DC et al (2014) Effects of exercise during adjuvant chemotherapy on breast cancer outcomes. Med Sci Sports Exerc 46:1744–1751
Friedenreich CM (2011) Physical activity and breast cancer: review of the epidemiologic evidence and biologic mechanisms. Recent Results Cancer Res 188:125–139
Coussens LM, Werb Z (2002) Inflammation and cancer. Nature 420:860–867
Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A (2009) Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis 30:1073–1081
George SM, Neuhouser ML, Mayne ST et al (2010) Postdiagnosis diet quality is inversely related to a biomarker of inflammation among breast cancer survivors. Cancer Epidemiol Biomarkers Prev 19:2220–2228
Ramos-Nino ME (2013) The role of chronic inflammation in obesity-associated cancers. ISRN Oncol 2013:697521
Bachelot T, Ray-Coquard I, Menetrier-Caux C, Rastkha M, Duc A, Blay JY (2003) Prognostic value of serum levels of interleukin 6 and of serum and plasma levels of vascular endothelial growth factor in hormone-refractory metastatic breast cancer patients. Br J Cancer 88:1721–1726
Knupfer H, Preiss R (2007) Significance of interleukin-6 (IL-6) in breast cancer (review). Breast Cancer Res Treat 102:129–135
Green AR, Green VL, White MC, Speirs V (1997) Expression of cytokine messenger RNA in normal and neoplastic human breast tissue: identification of interleukin-8 as a potential regulatory factor in breast tumours. Int J Cancer 72:937–941
De Larco JE, Wuertz BR, Rosner KA et al (2001) A potential role for interleukin-8 in the metastatic phenotype of breast carcinoma cells. Am J Pathol 158:639–646
Lissoni P, Barni S, Rovelli F, Tancini G (1991) Lower survival in metastatic cancer patients with reduced interleukin-2 blood concentrations. Preliminary report. Oncology 48:125–127
Papadopoulou E, Anagnostopoulos K, Tripsianis G et al (2008) Evaluation of predictive and prognostic significance of serum TGF-beta1 levels in breast cancer according to HER-2 codon 655 polymorphism. Neoplasma 55:229–238
Papadopoulou E, Tripsianis G, Anagnostopoulos K et al (2010) Significance of serum tumor necrosis factor-alpha and its combination with HER-2 codon 655 polymorphism in the diagnosis and prognosis of breast cancer. Int J Biol Markers 25:126–135
Dunn GP, Bruce AT, Ikeda H, Old LJ, Schreiber RD (2002) Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol 3:991–998
Di Paola M, Angelini L, Bertolotti A, Colizza S (1974) Host resistance in relation to survival in breast cancer. Br Med J 4:268–270
Hussell TCM, Wissinger E, Findlay EG (2010) Lymphocytes. In: Serhan CNWP, Gilroy DW (eds) Fundamentals of inflammation. Cambridge University Press, New York, pp 107–126
Stagg J, Allard B (2013) Immunotherapeutic approaches in triple-negative breast cancer: latest research and clinical prospects. Ther Adv Med Oncol 5:169–181
Mahmoud SM, Paish EC, Powe DG et al (2011) Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. J Clin Oncol 29:1949–1955
Denkert C, Loibl S, Noske A et al (2010) Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J Clin Oncol 28:105–113
Aaltomaa S, Lipponen P, Eskelinen M et al (1992) Lymphocyte infiltrates as a prognostic variable in female breast cancer. Eur J Cancer 28A:859–864
Carvalho MI, Pires I, Prada J, Queiroga FL (2014) A role for T-lymphocytes in human breast cancer and in canine mammary tumors. BioMed Res Int 2014:130894
Teschendorff AE, Miremadi A, Pinder SE, Ellis IO, Caldas C (2007) An immune response gene expression module identifies a good prognosis subtype in estrogen receptor negative breast cancer. Genome Biol 8:R157
Lehmann BD, Bauer JA, Chen X et al (2011) Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Investig 121:2750–2767
Bertucci F, Finetti P, Cervera N et al (2006) Gene expression profiling shows medullary breast cancer is a subgroup of basal breast cancers. Cancer Res 66:4636–4644
West NR, Milne K, Truong PT, Macpherson N, Nelson BH, Watson PH (2011) Tumor-infiltrating lymphocytes predict response to anthracycline-based chemotherapy in estrogen receptor-negative breast cancer. Breast Cancer Res 13:R126
West NR, Panet-Raymond V, Truong PT et al (2011) Intratumoral immune responses can distinguish new primary and true recurrence types of ipsilateral breast tumor recurrences (IBTR). Breast Cancer (Auckl) 5:105–115
Pierce BL, Ballard-Barbash R, Bernstein L et al (2009) Elevated biomarkers of inflammation are associated with reduced survival among breast cancer patients. J Clin Oncol 27:3437–3444
Pierce JP (2009) Diet and breast cancer prognosis: making sense of the Women’s Healthy Eating and Living and Women’s Intervention Nutrition Study trials. Curr Opin Obstet Gynecol 21:86–91
Ricciotti E, FitzGerald GA (2011) Prostaglandins and inflammation. Arterioscler Thromb Vasc Biol 31:986–1000
Holmes MD, Chen WY, Schnitt SJ et al (2011) COX-2 expression predicts worse breast cancer prognosis and does not modify the association with aspirin. Breast Cancer Res Treat 130:657–662
Ristimaki A, Sivula A, Lundin J et al (2002) Prognostic significance of elevated cyclooxygenase-2 expression in breast cancer. Cancer Res 62:632–635
van Nes JG, de Kruijf EM, Faratian D et al (2011) COX2 expression in prognosis and in prediction to endocrine therapy in early breast cancer patients. Breast Cancer Res Treat 125:671–685
Gasic GJ, Gasic TB, Stewart CC (1968) Antimetastatic effects associated with platelet reduction. Proc Natl Acad Sci USA 61:46–52
Gasic GJ, Gasic TB, Murphy S (1972) Anti-metastatic effect of aspirin. Lancet 2:932–933
Fraser DM, Sullivan FM, Thompson AM, McCowan C (2014) Aspirin use and survival after the diagnosis of breast cancer: a population-based cohort study. Br J Cancer 111:623–627
Rothwell PM, Wilson M, Price JF, Belch JFF, Meade TW, Mehta Z (2012) Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomised controlled trials. Lancet 379:1591–1601
Li YL, Brasky TM, Nie J et al (2012) Use of nonsteroidal anti-inflammatory drugs and survival following breast cancer diagnosis. Cancer Epidemiol Biomark Prev 21:239–242
Kwan ML, Habel LA, Slattery ML, Caan B (2007) NSAIDs and breast cancer recurrence in a prospective cohort study. Cancer Causes Control 18:613–620
Blair CK, Sweeney C, Anderson KE, Folsom AR (2007) NSAID use and survival after breast cancer diagnosis in post-menopausal women. Breast Cancer Res Treat 101:191–197
Retsky M, Demicheli R, Hrushesky WJ et al (2013) Reduction of breast cancer relapses with perioperative non-steroidal anti-inflammatory drugs: new findings and a review. Curr Med Chem 20:4163–4176
Zhang Y, Coogan PF, Palmer JR, Strom BL, Rosenberg L (2005) Use of nonsteroidal antiinflammatory drugs and risk of breast cancer: the case–control surveillance study revisited. Am J Epidemiol 162:165–170
Irwin MR (2013) Depression and insomnia in cancer: prevalence, risk factors, and effects on cancer outcomes. Curr Psychiatry Rep 15:404
Bower JE, Ganz PA, Dickerson SS, Petersen L, Aziz N, Fahey JL (2005) Diurnal cortisol rhythm and fatigue in breast cancer survivors. Psychoneuroendocrinology 30:92–100
Costa AR, Fontes F, Pereira S, Goncalves M, Azevedo A, Lunet N (2014) Impact of breast cancer treatments on sleep disturbances—a systematic review. Breast 23:697–709
Mullington JM, Simpson NS, Meier-Ewert HK, Haack M (2010) Sleep loss and inflammation. Best Pract Res Clin Endocrinol Metab 24:775–784
Besedovsky L, Lange T, Born J (2012) Sleep and immune function. Pflugers Arch 463:121–137
Irwin MR, Olmstead RE, Ganz PA, Hague R (2013) Sleep disturbance, inflammation and depression risk in cancer survivors. Brain Behav Immun 30:S58–S67
Shearer WT, Reuben JM, Mullington JM et al (2001) Soluble TNF-alpha receptor 1 and IL-6 plasma levels in humans subjected to the sleep deprivation model of spaceflight. J Allergy Clin Immunol 107:165–170
Haack M, Sanchez E, Mullington JM (2007) Elevated inflammatory markers in response to prolonged sleep restriction are associated with increased pain experience in healthy volunteers. Sleep 30:1145–1152
Saxe GA, Rock CL, Wicha MS, Schottenfeld D (1999) Diet and risk for breast cancer recurrence and survival. Breast Cancer Res Treat 53:241–253
Holmes MD, Stampfer MJ, Colditz GA, Rosner B, Hunter DJ, Willett WC (1999) Dietary factors and the survival of women with breast carcinoma. Cancer 86:826–835
Izano MA, Fung TT, Chiuve SS, Hu FB, Holmes MD (2013) Are diet quality scores after breast cancer diagnosis associated with improved breast cancer survival? Nutr Cancer 65:820–826
Kim EH, Willett WC, Fung T, Rosner B, Holmes MD (2011) Diet quality indices and postmenopausal breast cancer survival. Nutr Cancer 63:381–388
Gou YJ, **e DX, Yang KH et al (2013) Alcohol consumption and breast cancer survival: a meta-analysis of cohort studies. Asian Pac J Cancer Prev 14:4785–4790
Borugian MJ, Sheps SB, Kim-Sing C et al (2004) Insulin, macronutrient intake, and physical activity: are potential indicators of insulin resistance associated with mortality from breast cancer? Cancer Epidemiol Biomark Prev 13:1163–1172
Research. WCRFAIfC (2010) Continuous Update Project Report. Food, Nutrition, Physical Activity, and the Prevention of Breast Cancer. World Cancer Research Fund/American Institute for Cancer Research
Makarem N, Chandran U, Bandera EV, Parekh N (2013) Dietary fat in breast cancer survival. Annu Rev Nutr 33(33):319–348
Jain M, Miller AB (1997) Tumor characteristics and survival of breast cancer patients in relation to premorbid diet and body size. Breast Cancer Res Treat 42:43–55
Bauer SR, Hankinson SE, Bertone-Johnson ER, Ding EL (2013) Plasma vitamin D levels, menopause, and risk of breast cancer: dose-response meta-analysis of prospective studies. Medicine (Baltimore) 92:123–131
Goodwin PJ, Ennis M, Pritchard KI, Koo J, Hood N (2009) Prognostic effects of 25-hydroxyvitamin D levels in early breast cancer. J Clin Oncol 27:3757–3763
Zehnder D, Bland R, Chana RS et al (2002) Synthesis of 1,25-dihydroxyvitamin D(3) by human endothelial cells is regulated by inflammatory cytokines: a novel autocrine determinant of vascular cell adhesion. J Am Soc Nephrol 13:621–629
Garland CF, Garland FC, Gorham ED et al (2006) The role of vitamin D in cancer prevention. Am J Public Health 96:252–261
Cantorna MT, Zhu Y, Froicu M, Wittke A (2004) Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr 80:1717S–1720S
Yao S, Sucheston LE, Millen AE et al (2011) Pretreatment serum concentrations of 25-hydroxyvitamin D and breast cancer prognostic characteristics: a case–control and a case-series study. PLoS ONE 6:e17251
Peppone LJ, Rickles AS, Janelsins MC, Insalaco MR, Skinner KA (2012) The Association Between Breast Cancer Prognostic Indicators and Serum 25-OH Vitamin D Levels. Ann Surg Oncol 19:2590–2599
Villasenor A, Ballard-Barbash R, Ambs A et al (2013) Associations of serum 25-hydroxyvitamin D with overall and breast cancer-specific mortality in a multiethnic cohort of breast cancer survivors. Cancer Causes Control 24:759–767
Buttigliero C, Monagheddu C, Petroni P et al (2011) Prognostic role of vitamin d status and efficacy of vitamin D supplementation in cancer patients: a systematic review. Oncologist 16:1215–1227
Thompson LU, Boucher BA, Liu Z, Cotterchio M, Kreiger N (2006) Phytoestrogen content of foods consumed in Canada, including isoflavones, lignans, and coumestan. Nutr Cancer 54:184–201
Thompson LU, Boucher BA, Cotterchio M, Kreiger N, Liu Z (2007) Dietary phytoestrogens, including isoflavones, lignans, and coumestrol, in nonvitamin, nonmineral supplements commonly consumed by women in Canada. Nutr Cancer 59:176–184
Trock BJ, Hilakivi-Clarke L, Clarke R (2006) Meta-analysis of soy intake and breast cancer risk. J Natl Cancer Inst 98:459–471
Wu AH, Yu MC, Tseng CC, Pike MC (2008) Epidemiology of soy exposures and breast cancer risk. Br J Cancer 98:9–14
Dong JY, Qin LQ (2011) Soy isoflavones consumption and risk of breast cancer incidence or recurrence: a meta-analysis of prospective studies. Breast Cancer Res Treat 125:315–323
Buck K, Zaineddin AK, Vrieling A, Linseisen J, Chang-Claude J (2010) Meta-analyses of lignans and enterolignans in relation to breast cancer risk. Am J Clin Nutr 92:141–153
Velentzis LS, Cantwell MM, Cardwell C, Keshtgar MR, Leathem AJ, Woodside JV (2009) Lignans and breast cancer risk in pre- and post-menopausal women: meta-analyses of observational studies. Br J Cancer 100:1492–1498
Zaineddin AK, Vrieling A, Buck K et al (2012) Serum enterolactone and postmenopausal breast cancer risk by estrogen, progesterone and herceptin 2 receptor status. Int J Cancer 130:1401–1410
Nagaraju GP, Zafar SF, El-Rayes BF (2013) Pleiotropic effects of genistein in metabolic, inflammatory, and malignant diseases. Nutr Rev 71:562–572
Guha N, Kwan ML, Quesenberry CP Jr, Weltzien EK, Castillo AL, Caan BJ (2009) Soy isoflavones and risk of cancer recurrence in a cohort of breast cancer survivors: the Life After Cancer Epidemiology study. Breast Cancer Res Treat 118:395–405
Kang X, Zhang Q, Wang S, Huang X, ** S (2010) Effect of soy isoflavones on breast cancer recurrence and death for patients receiving adjuvant endocrine therapy. CMAJ 182:1857–1862
Zhang YF, Kang HB, Li BL, Zhang RM (2012) Positive effects of soy isoflavone food on survival of breast cancer patients in China. Asian Pac J Cancer Prev 13:479–482
Shu XO, Zheng Y, Cai H et al (2009) Soy food intake and breast cancer survival. JAMA 302:2437–2443
Caan BJ, Natarajan L, Parker B et al (2011) Soy food consumption and breast cancer prognosis. Cancer Epidemiol Biomarkers Prev 20:854–858
Buck K, Vrieling A, Zaineddin AK et al (2011) Serum enterolactone and prognosis of postmenopausal breast cancer. J Clin Oncol 29:3730–3738
Chi F, Wu R, Zeng YC, **ng R, Liu Y, Xu ZG (2013) Post-diagnosis soy food intake and breast cancer survival: a meta-analysis of cohort studies. Asian Pac J Cancer Prev 14:2407–2412
Nechuta SJ, Caan BJ, Chen WY et al (2012) Soy food intake after diagnosis of breast cancer and survival: an in-depth analysis of combined evidence from cohort studies of US and Chinese women. Am J Clin Nutr 96:123–132
Lucock M (2000) Folic acid: nutritional biochemistry, molecular biology, and role in disease processes. Mol Genet Metab 71:121–138
Ray JG (2004) Folic acid food fortification in Canada. Nutr Rev 62:S35–S39
Shane B (2003) Folate fortification: enough already? Am J Clin Nutr 77:8–9
Kim YI (2004) Folate and DNA methylation: a mechanistic link between folate deficiency and colorectal cancer? Cancer Epidemiol Biomarkers Prev 13:511–519
Kim YI (2003) Role of folate in colon cancer development and progression. J Nutr 133:3731S–3739S
Kim YI (2007) Folate and colorectal cancer: an evidence-based critical review. Mol Nutr Food Res 51:267–292
Kim YI (2007) Folic acid fortification and supplementation–good for some but not so good for others. Nutr Rev 65:504–511
Kim YI (2006) Folate: a magic bullet or a double edged sword for colorectal cancer prevention? Gut 55:1387–1389
Kotsopoulos J, Kim YI, Narod SA (2012) Folate and breast cancer: what about high-risk women? Cancer Causes Control 23:1405–1420
Kim YI (2006) Does a high folate intake increase the risk of breast cancer? Nutr Rev 64:468–475
Giovannucci E, Chan AT (2010) Role of vitamin and mineral supplementation and aspirin use in cancer survivors. J Clin Oncol 28:4081–4085
Bright-Gbebry M, Makambi KH, Rohan JP et al (2011) Use of multivitamins, folic acid and herbal supplements among breast cancer survivors: the black women’s health study. BMC Complement Altern Med 11:30
Velicer CM, Ulrich CM (2008) Vitamin and mineral supplement use among US adults after cancer diagnosis: a systematic review. J Clin Oncol 26:665–673
McEligot AJ, Mouttapa M, Ziogas A, Anton-Culver H (2009) Diet and predictors of dietary intakes in women with family history of breast and/or ovarian cancer. Cancer Epidemiol 33:419–423
Saquib J, Rock CL, Natarajan L et al (2011) Dietary intake, supplement use, and survival among women diagnosed with early-stage breast cancer. Nutr Cancer 63:327–333
Sellers TA, Alberts SR, Vierkant RA et al (2002) High-folate diets and breast cancer survival in a prospective cohort study. Nutr Cancer Int J 44:139–144
Rossi E, Hung J, Beilby JP, Knuiman MW, Divitini ML, Bartholomew H (2006) Folate levels and cancer morbidity and mortality: prospective cohort study from Busselton, Western Australia. Ann Epidemiol 16:206–212
Harris HR, Bergkvist L, Wolk A (2012) Folate intake and breast cancer mortality in a cohort of Swedish women. Breast Cancer Res Treat 132:243–250
Xu X, Gammon MD, Wetmur JG et al (2008) B-vitamin intake, one-carbon metabolism, and survival in a population-based study of women with breast cancer. Cancer Epidemiol Biomarkers Prev 17:2109–2116
Lee Y, Lee SA, Choi JY et al (2012) Prognosis of breast cancer is associated with one-carbon metabolism related nutrients among Korean women. Nutr J 11:59
Zhang Z, Wang J, Tacha DE et al (2014) Folate receptor alpha associated with triple-negative breast cancer and poor prognosis. Arch Pathol Lab Med 138:890–895
Shen JY, Hilgenbrink AR, **a W et al (2014) Folate receptor-beta constitutes a marker for human proinflammatory monocytes. J Leukoc Biol 96:563–570
Abbenhardt C, Miller JW, Song XL et al (2014) Biomarkers of one-carbon metabolism are associated with biomarkers of inflammation in women. J Nutr 144:714–721
Al-Sader H, Abdul-Jabar H, Allawi Z, Haba Y (2009) Alcohol and breast cancer: the mechanisms explained. J Clin Med Res 1:125–131
Poschl G, Seitz HK (2004) Alcohol and cancer. Alcohol Alcohol 39:155–165
Molina PE, Hoek JB, Nelson S et al (2003) Mechanisms of alcohol-induced tissue injury. Alcohol Clin Exp Res 27:563–575
Ali AMG, Schmidt MK, Bolla MK et al (2014) Alcohol consumption and survival after a breast cancer diagnosis: a literature-based meta-analysis and collaborative analysis of data for 29,239 cases. Cancer Epidemiol Biomark Prev 23:934–945
Centers for Disease Control and Prevention. (2009) Alcohol use among pregnant and nonpregnant women of childbearing age—United States, 1991–2005. Morbidity and Mortality Weekly Report, pp 529–32
Author information
Authors and Affiliations
Corresponding author
Additional information
Darren R. Brenner and Nigel T. Brockton have been contributed equally.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Brenner, D.R., Brockton, N.T., Kotsopoulos, J. et al. Breast cancer survival among young women: a review of the role of modifiable lifestyle factors. Cancer Causes Control 27, 459–472 (2016). https://doi.org/10.1007/s10552-016-0726-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-016-0726-5