
Abstract
Background
The adaptation of steroid therapy and the effect of renin–angiotensin–aldosterone system inhibitors (RASIs) for advanced immunoglobulin A nephropathy (IgAN) patients with impaired renal function are still controversial.
Methods
We divided 63 IgAN patients with an estimated glomerular filtration rate (eGFR) of <60 ml/min/1.73 m2 and proteinuria ≥ 0.5 g/day into two groups: the RASI group (RASI, n = 33), treated with RASIs alone; and the combination group (COMBI, n = 30), treated with corticosteroids and RASIs. We analyzed the clinical and histological background, renal survival rate, and the risk factors for progression.
Results
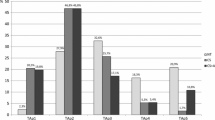
Renal function (mean eGFR: COMBI 46.4 vs. RASI 47.0 ml/min/1.73 m2), the amount of proteinuria (median: COMBI 1.39 vs. RASI 1.17 g/g creatinine) and histological backgrounds were not significantly different between the groups, but urinary red blood cells (U-RBCs) were significantly higher in the COMBI group than in the RASI group (median: COMBI 30.0 vs. RASI 10.0 counts/high-power field, P = 0.0171). The serial change in proteinuria did not differ until 5 years after treatment, but U-RBCs were significantly decreased in both groups (P < 0.0001), and eGFR was significantly decreased in the RASI group (P < 0.001) but not in the COMBI group. The results for each year after treatment did not differ significantly between both groups. The renal survival rate was not significantly different between the groups. There was no independent risk factor for progression by Cox regression analysis.
Conclusion
Combination therapy with steroids and RASIs was not superior to monotherapy with RASIs for advanced IgAN with impaired renal function.





Similar content being viewed by others


References
Locatelli F, Del Vecchio L, Pozzi C. IgA glomerulonephritis: beyond angiotensin-converting enzyme inhibitors. Nat Clin Pract. 2006;2:24–31.
Barratt J, Feehally J. IgA nephropathy. J Am Soc Nephrol. 2005;16:1097–2088.
Tumlin JA, Madaio MP, Hennigar R. Idiopthic IgA nephropathy: pathogenesis, histopathology, and therapeutic options. Clin J Am Soc Nephrol. 2004;2:1054–61.
Cheng J, Zhang X, Zhang W, He Q, Tao X, Chen J. Efficacy and safety of glucocorticoids therapy for IgA nephropathy: a meta-analysis of randomized controlled trials. Am J Nephrol. 2009;30:315–22.
Strippoli GFM. IgA nephropathy: a disease in search of a large-scale clinical trial to reliably inform practice. Am J Kidney Dis. 2009;53:5–8.
Dillon JJ. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for IgA nephropathy. Semin Nephrol. 2004;24:218–24.
Cheng J, Zhang W, Zhang XH, He Q, Tao XJ, Chen JH. ACEI/ARB therapy for IgA nephropathy: a meta analysis of randomized controlled trials. Int J Clin Pract. 2009;63:880–8.
Chan JCM, Trachtman H. Modulating the progression in IgA nephropathy. Nephron Clin Pract. 2006;104:61–8.
Dillon JJ. Treating IgA nephropathy. J Am Soc Nephrol. 2001;12:846–7.
Ballardie FW. Quantitative appraisal of treatment options for IgA nephropathy. J Am Soc Nephrol. 2007;18:2806–9.
Laville M, Alamartine E. Treatment options for IgA nephropathy in adults: aproposal for evidence-based strategy. Nephrol Dial Transpl. 2004;19:1947–51.
Moriyama T, Honda K, Nitta K, Yumura W, Nihei H. The effectiveness of steroid therapy for patients with advanced IgA nephropathy and impaired renal function. Clin Exp Nephrol. 2004;8:237–42.
Moriyama T, Amamiya N, Ochi A, Tsuruta Y, Shimizu A, Kojima C, et al. Long-term beneficial effects of angiotensin-converting enzyme inhibitor and angiotensin receptor blocker therapy for patients with advanced immunoglobulin A nephropathy and impaired renal function. Clin Exp Nephrol. 2011;15:700–07.
Moriyama T, Amemiya N, Ochi A, Tsuruta Y, Shimizu A, Itabashi M, et al. Comparison of steroids and angiotensin receptor blockers for patients with advanced IgA nephropathy and impaired renal function. Am J Nephrol. 2011;34:233–40.
Clinical guidelines for immunoglobulin A (IgA) nephropathy in Japan, third version. Nippon **zo Gakkai Shi 2001; 53:123–135.
Manno C, Torres DD, Rossini M, Pesce F, Schena FP. Randomized controlled clinical trial of corticosteroids plus ACE-inhibitors with long-term follow-up in proteinuric IgA nephropathy. Nephrol Dial Transpl. 2009;24:3694–701.
Lv J, Zhang H, Chen Y, Li G, Jiang L, Singh AK, et al. Combination therapy of prednisolone and ACE inhibitor versus ACE-inhibitor therapy alone in patients with IgA nephropathy: a randomized controlled trial. Am J Kidney Dis. 2009;53:26–32.
Choi S, Lee D, Jeong KH, Moon JY, Lee SH, Lee TW, et al. Prognostic relevance of clinical and histological features in IgA nephropathy treated with steroid and angiotensin receptor blockers. Clin Nephrol. 2009;72:353–9.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Moriyama, T., Nakayama, K., Ochi, A. et al. Comparison of inhibitors of renin–angiotensin–aldosterone system (RAS) and combination therapy of steroids plus RAS inhibitors for patients with advanced immunoglobulin A nephropathy and impaired renal function. Clin Exp Nephrol 16, 231–237 (2012). https://doi.org/10.1007/s10157-011-0545-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-011-0545-7