
Abstract
Background
Photodynamic therapy (PDT) plays an immunoregulatory role in tumours. Here, we conducted a retrospective patient analysis to evaluate the effectiveness of PDT plus immune checkpoint inhibitors (ICIs) in gastric cancer. Further, we performed a dynamic analysis of gastric cancer patients receiving PDT to clarify its effects on anti-tumour immunity.
Methods
Forty ICI-treated patients that received PDT or not were retrospectively analysed. Five patients with gastric adenocarcinoma were enrolled for sample collection before and after PDT. Single-cell RNA/T cell receptor (TCR) sequencing, flow cytometry and histological exanimation were used to analyse the collected specimens.
Results
Patients in PDT group had a significantly better OS after ICI treatment than those in No PDT group. Single-cell analysis identified ten cell types in gastric cancer tissues and four sub-populations of T cells. Immune cell infiltration increased in the tumours after PDT and the circular immune cells showed consistent alterations. TCR analysis revealed a specific clonal expansion after PDT in cytotoxic T lymphocytes (CTL), but a constriction in Tregs. The B2M gene is upregulated in tumour cells after PDT and is associated with immune cell infiltration. Several pathways involving the positive regulation of immunity were enriched in tumour cells in the post-PDT group. The interactions following PDT were increased between tumour cells and effector cells but decreased between Tregs and other immune cells. Some co-stimulatory signaling emerged, whereas co-inhibitory signaling disappeared in intercellular communication after PDT.
Conclusions
PDT elicits an anti-tumour response through various mechanisms and is promising as an adjuvant to enhance ICI benefit.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer remains one of the most common malignant tumours of the digestive tract. Patients with gastric cancer have poor outcomes when the cancer progresses to advanced or metastatic stages, with a 5-year survival rate of < 20% [1, 2]. In recent years, immune checkpoint inhibitors (ICIs) have been developed and approved for the systemic treatment of gastric cancer, which has brought the management of gastric cancer into the era of immunotherapy. In China, ICIs plus chemotherapy are currently the first-line treatment for metastatic diseases [3]. However, not many patients with gastric cancer can benefit from ICIs despite remarkable tumour regression in some patients, which limits ICI use in clinical practice. The success of ICIs is highly dependent on the immune microenvironment within the tumour. The so-called “hot tumour”, indicated by increased immune cell infiltration, is always associated with better outcomes with ICIs [4]. As most patients present with ‘cold’ tumours in gastric cancer, it is important to adjust the immune microenvironment to facilitate improved efficacy of ICI treatments.
Photodynamic therapy (PDT) is a local tumour treatment, in which a photosensitive drug is injected into the body, followed by focusing laser light on the tumour site to generate reactive oxygen species to induce cytotoxic effects. In several studies, PDT was found to produce an immunostimulatory effect on various cancer types [5, 6]. PDT reportedly increases tumour antigen exposure in other cancers and promotes immunogenic cell death (ICD), resulting in the activation of an anti-tumour immune response [7]. The combination of PDT and CTLA-4 antibody was verified to control tumours in mouse models [8, 9]. These studies showed the potential of PDT to improve anti-tumour immunity. However, most of this evidence comes from preclinical models, and human studies on gastric cancer are scarce. In addition, the mechanism underlying the PDT-induced immune response is still poorly understood. The clinical value of PDT in combination with ICIs remains unclear in gastric cancer.
Single-cell sequencing technology has developed rapidly in recent years. This method allowed us to explore the spatiotemporal characteristics of biological tissues at the single-cell level. It has been widely used for analysing the tumour environment, including that in gastric cancer [10,11,12]. In this study, we first, retrospectively, compared the outcome of patients receiving PDT plus ICIs to those receiving ICIs alone, aimed at preliminarily evaluating their synergistic effects. We also performed single-cell transcriptome (scRNA-seq) and T cell receptor (scTCR-seq) sequencing accompanied by flow cytometry and histological examination of matched specimens before and after PDT in gastric cancer patients to identify the immunological changes following PDT in gastric cancer and explore the underlying mechanisms.
Material and methods
Patients and treatments
Collection of information of the retrospective cohorts
We retrospectively included the patients who received ICIs with or without PDT in our centre to explore the effect of PDT on improving ICI benefits. The detailed methodology of the retrospective study can be found in the supplementary methods (Electronic Supplementary Material 1). The inclusion criteria were as follows: (1) patients with confirmed gastric adenocarcinoma; (2) advanced patients (III or IV stage); (3) receiving at least one cycle of ICIs for first- or second-line treatment; and (4) having a follow-up time of > 2 mo. Patients were excluded if they had poor conditions, severe comorbidities, and/or a combination with immunomodulator drugs. Patients were classified as PDT and No PDT groups according to the usage of PDT prior to ICIs. Patients in PDT group received PDT treatment within one month before receiving the first dose of ICI. Baseline information and overall survival (OS) were collected from each patient. OS was defined as the time from ICI initiation to death of any cause or last follow-up.
Sample collection
We recruited five PDT-planned patients with gastric adenocarcinoma confirmed by pathological examination to collect samples for detection. The exclusion criteria were patients with PDT contraindications, poor general condition (ECOG ≥ 3), combination of immunoregulatory drugs, and multiple primary tumours. Once the patients were included, they received PDT of the standard protocol. The photosensitizer (hematoporphyrin injection, Hiporfin®) was intravenously administered to patients 48 h before the operation. The injected dose was calculated based on the patient weight (3 mg/kg). Patients remained in a dark room to avoid light exposure until PDT. On the day of the PDT operation, peripheral blood (pt1–3) and tumour biopsy samples (pt1–5) were collected from recruited patient as pre-PDT samples. For blood collection, 4 ml blood was obtained per patient and preserved in EDTA tubes, and tumour samples were obtained through endoscopic biopsy. Thereafter, PDT was performed. A columnar fibre (4–6 cm) was introduced into the stomach and placed close to the tumour site. Two or three illumination segments were used, with an illumination power of 800 mW. The duration of illumination per segment was determined based on tumour size, location, and invasiveness, and ranged from 10 to 15 min. The illuminated sites were washed with normal saline (NaCl 0.9%) solution when the PDT illumination was completed. The PDT protocol included four operations performed every 24 h. Post-PDT matched samples were collected from the same patients 48 h after the initial PDT operation (that is, on the third operation), using the same methods employed for pre-PDT sample collection. This decision was based on our observation during clinical practice, where we noted a significant inflammatory response in the majority of patients at the 48-h mark following PDT. The collected blood was used for flow cytometry, whereas the tumour samples were used for single-cell RNA/TCR sequencing (scRNA/TCR-seq) (n = 6) and histological examination (n = 4).
Study design and group
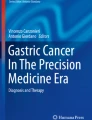
The workflow of this study is illustrated in Fig. 1. Two studies were conducted, including retrospective analysis of an ICI cohort and detection of the collected samples. Flow cytometry was performed to detect the levels of immune cells in peripheral blood. Single-cell sequencing was used to characterise the tumour microenvironment, including gene expression (scRNA-seq) and immune profiles (scTCR-seq). Hematoxylin–Eosin (HE) staining was conducted on tumour samples to show the spatial changes of PDT-treated tumours. To ensure an adequate collection of tumour tissues for evaluation while avoiding the risks of adverse events associated with repetitive endoscopic biopsy, patients were divided into two groups for specialized tumour collections. Patients 1–3 were exclusively used for the scRNA/TCR-seq analysis, while patients 4 and 5 were dedicated to the HE evaluation. The samples were classified into pre- and post-PDT groups according to the time of collection. The cohort of patients receiving ICIs were grouped into PDT and No PDT to compare their benefits from ICIs.

Design and workflow of the study. a retrospective analysis of an ICI cohort with or without PDT. b sample detection of patients receiving PDT (n = 5). ICI immune checkpoint inhibitor, PDT photodynamic therapy
Tissue dissociation and preparation of single-cell suspensions
The obtained tumour samples were washed with 1 × phosphate-buffered saline (PBS) two to three times, then cut into small pieces. The tumour was digested using the hydrolysate prepared using collagenases 1 and 4. For this process, the sample was incubated in a constant-temperature water bath at 37 °C, and the dissociation was terminated when the tissue mass disappeared. The cell suspension was filtered through a 40 µm cell strainer and centrifuged at 300×g for 5 min at 4 °C. After discarding the supernatant, the cells were re-suspended and incubated with 3 ml pre-cooled erythrocyte lysis liquid (Solarbio, China) for 5 min at 4 °C. Subsequently, the cell suspension was centrifuged again under the same conditions, fully re-suspended, and maintained on ice after removing the supernatant. Finally, the cells were counted using a cell counter (Countstar Rigel S2; Alit Biotech Shanghai, China) and adjusted for concentration until the following criteria were met: cell concentration ranging from 700 to 1200 cell/µL, live cell proportion > 85%, and agglomeration proportion < 15%.
10X genomics single-cell RNA and immune profiling sequencing
scRNA-seq and scTCR-seq were performed using the Single Cell Immune Profiling Solution from 10X Genomics (California, USA). Single-cell capture, reverse transcription, cell lysis, cDNA amplification, and library preparation were performed according to the manufacturer’s protocols (10X Genomics V(D)J+ 5’ Gene Expression). Up to 7000 cells were loaded onto the Chromium Controller for each sample. The constructed libraries were sequenced on an Illumina NovaSeq 6000 platform (California, USA) using the 150 bp paired-end protocol.
Data analysis of scRNA-seq and scTCR-seq
Acquirement of single-cell expression matrices
Raw data were imported into the 10X CellRanger (v6.0.0) software and mapped to the human reference genome using default parameters. Cells were identified according to the barcode and unique molecule identifiers (UMIs) were counted for each gene to create expression matrices. The R package Seurat (v4.0.1) was used for the secondary filtration. Only genes expressed in ≥ 10 cells were considered. Cells with total expressed genes < 500, UMI count < 100, or mitochondria-expressed genes > 20% were excluded. After filtering, the remaining cells were used for downstream analysis. Seurat was used for the normalisation of data. Since the same barcode lists were used, the scRNA-seq data were analysed with the scTCR-seq data.
Cluster identification and cell annotation
Seurat was used to cluster the cells. The top 3000 highly variable genes were selected and principal component analysis (PCA) was applied to reduce dimensionality. The 50 most informative principal components were finally selected for t-distributed stochastic neighbour embedding (t-SNE) clustering visualisation. The resolution parameter was set to 0.2. The FindAllMarkers function was used to identify the marker genes of each cluster. The cell types were identified using the singleR package. For cells that could not be annotated automatically, manual correction was performed using the reported cell markers. T cells were retrieved, and de novo clustering was performed to identify the sub-clusters of these T cells. The same method was applied for sub-cluster annotation. For sub-clustering, a resolution of 0.5 was applied when performing t-SNE analysis. According to the sample source, cells were divided into pre- and post-PDT groups, and the change in cell proportions following PDT was analysed.
Distinction of malignant and non-malignant cell
Epithelial cells were classified as malignant or non-malignant using the method defined by Liu et al. [10]. In brief, malignant and non-malignant cells were determined using the k-means clustering algorithm according to the malignant and non-malignant scores that were calculated using the corresponding marker genes. The FindAllMarkers function was used to identify marker genes of the identified malignant cells. The proportions of malignant and non-malignant cells in the pre- and post-PDT groups were compared. Differential gene analysis was performed on malignant cells in the pre- and post-PDT groups using the FindAllMarker function. Significant differential genes were selected with |log2FC|> log2(3/2) and p_val_adj < 0.05. Volcano plots and heat maps were drawn to visualise differentially expressed genes. In addition, functional annotation and enrichment analysis, including Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analyses, were performed using the clusterProfiler package, and the pathways with p_val_adj < 0.05 were considered as significantly enriched. The GO plot package was used to calculate the z score and create a functional annotation plot. The expression of B2M (one of the genes encoding the MHC I molecule) was separately compared between pre- and post-PDT groups by drawing a violin plot. The Cancer Genome Atlas (TCGA)-based online tool in the TIMER database [13] was used to evaluate the association between B2M and immune cell infiltration in gastric cancer.
Analysis of cell-to-cell communication
The CellPhoneDB algorithm (v2.1.7) was applied to evaluate cell-to-cell communication, as indicated by the detection of ligand-receptor interactions. This algorithm allows for the identification of ligand-receptor interactions between two cell types [14]. The direction of interactions was not considered during the CellPhoneDB analysis. In other words, for the ligand A-receptor B interaction, the condition of A in cell 1 and B in cell 2 was the same as that of A in cell 2 and B in cell 1. We evaluated the interactions among the following cell subsets: malignant epithelial cells, non-malignant epithelial cells, natural killer T (NKT) cells, T helper (Th) cells, CD4+ regulatory T (Treg) cells, and CD8+ cytotoxic T cells (CTL). The number of interactions between these cells was evaluated and the differences observed before and after PDT were analysed using heatmaps. We also searched for specific interactions that emerged or disappeared after PDT. Dot plots were drawn to indicate specific interactions.
Assessment of the TCR repertoire
The CellRanger vdj pipeline was used to process TCR sequencing data. CDR3 region and TCR genes were identified to generate clonotypes. We mapped the TCR data to scRNA-seq data-identified cell types. Only cells with productive TCR sequencing, annotated as T-cell types, were included in the following analyses. Clonal cells were defined as having a clonotype shared by ≥ 2 cells. The frequency of clonal expansion is defined as the proportion of clonal cells in a specific cluster. Clones for an identified clonotype were counted to determine the clonotype size. The Shannon-Weiner and Simpson indices were calculated using the vegan package to analyse the TCR diversity. These analyses were performed on total T cells and individually in each T cell subgroup. Differences in TCR were explored between T cells in the pre- and post-PDT groups.
Flow cytometry
The collected peripheral blood was sent for flow cytometry after pre-processing. The detected cells and corresponding label antibodies were as follows: total T lymphocytes (CD3+), total B lymphocytes (CD19+), NK cells (CD3-CD56+), NK-T cells (CD3+ CD56+), Th cells (CD3+ CD4+), CTL (CD3+ CD8+), naïve CD4+ T cells (CD4+ CD45RA+), effector/memory CD4+ T cells (CD4+ CD45RO+), naïve CD8+ T cells (CD8+ CD45RA+), effector/memory CD8+ T cells (CD8+ CD45RO+), PD1+ T cells (PD1+), and Treg cells (CD4+CD25+CD127-). Antibodies were purchased from BD Biosciences (New Jersey, USA) and Tian** Kuangbo Tongsheng Biotechnology (Tian**, China). Flow cytometry was performed on a BD FACSCanto II (BD Biosciences, California, USA), and the cell populations were recognised with a specific gate setting. The data were analysed using FlowJo software (v10.4).
Histological examination
The collected tumour tissues were fixed in 10% neutral formalin overnight and fixed tissues were dehydrated and embedded in paraffin. Subsequently, they were sectioned into 4 um slices and attached onto a glass slide. HE staining was finally performed and all sections were observed under a light field microscope. The final assessment of histological changes was performed by an experienced pathologist.
Statistical analysis
Some statistical methods used for independent analyses have been described previously. Quantitative data were presented as violin plots or summarized with mean ± standard deviation. Categorical data were presented as number with percentage. The constituents of the cell sets were present in proportions. If the quantitative data were normally distributed, Student’s t or paired-t tests were used for hypothesis testing; otherwise, Mann–Whitney U or Wilcoxon signed-rank tests were used. For the testing of categorical data, χ2 or Fisher’s exact test were used. Survival curve was drawn using the Kaplan Meier method and log-rank test was used to compare the difference between two curves. Univariate and multivariate Cox regression analyses were performed to calculate the hazard ratios (HRs) with 95% confidence intervals (CIs) and identify independent factors associated with OS. Data analysis and plot drawing were completed using R software (v4.0.3) and the specific analytical tools mentioned above. All statistical tests were two-tailed, and statistical significance was set at p < 0.05.
Results
The effectiveness of PDT in improving ICI benefits
Forty patients receiving ICIs were finally included for survival analysis. Nineteen patients received PDT prior to ICI treatment, whereas 21 patients did not. There was no significant difference of baseline characteristics between PDT group and No PDT group (Supplementary Table S1). The OS was superior in PDT group than that in No PDT group with median 17.2 vs 10.1 months (HR = 0.33, 95% CI [0.12, 0.93], p = 0.030; Fig. 2a). Univariate Cox regression analysis identified that PDT and stage were two factors associated with OS (Fig. 2b). After adjusting for the prognostic factor of stage, multivariate Cox regression analysis still showed that the usage of PDT was associated with significantly better OS (HR = 0.33, 95% CI [0.11, 0.97], p = 0.043; Fig. 2c). A subgroup analysis was performed on patients in the PDT group based on the timing of PDT usage. The analysis revealed no significant difference in OS between patients who received PDT within one week before ICI initiation and those who received PDT over one week, although the former group tended to have a better OS (HR = 0.66, 95% CI [0.14, 3.20], p = 0.600; Fig. 2d, e). In the analysis conducted separately for patients in the PDT and No PDT groups, a comparison was made regarding the OS between individuals with and without distant metastases. The results demonstrated that in the PDT group, there was no significant difference in OS between patients with metastatic and non-metastatic diseases (HR = 2.06, 95% CI [0.53, 8.00], p = 0.286; Fig. 2f). However, in the No PDT group, patients with metastatic diseases exhibited a significantly worse OS compared to those without metastases (HR = 7.44, 95% CI [1.69, 32.73], p = 0.002; Fig. 2g). This suggested that the use of PDT in conjunction with ICIs may have a beneficial effect in controlling metastatic diseases, and could improving the OS, regardless of whether patients have metastases or not.

Association between PDT usage and the prognosis of patients with ICIs in gastric cancer. a survival curve showing the OS of patients in PDT and No PDT group. b, c forest plots showing the univariate and multivariate Cox regression results of each variable. d survival curve showing the OS of patients who received PDT at different time intervals prior to ICI initiation. e risk plot showing the survival status and timing of PDT administration for each patient who received PDT. f survival curve showing the OS of patients with or without metastases in PDT group. g survival curve showing the OS of patients with or without metastases in No PDT group. PDT photodynamic therapy, ICIs immune checkpoint inhibitors, OS overall survival
Single-cell profiling from patients receiving PDT
To further clarify the role of PDT in anti-tumour immune response, we included three patients who received PDT for single-cell analysis. The clinical characteristics of each patient are shown in Supplementary Table S2. Tumour samples were successfully collected from all patients before and after PDT and were sent for single-cell sequencing. After cell filtration, 26,254 cells were retained for data analysis. The median numbers of genes and transcripts per cell were 1314 and 2678, respectively. We classified these cells into 13 clusters after dimension reduction (Fig. 3a). By map** them to the known cell types through marker genes, these clusters were annotated as ten cell types, including epithelial cells, fibroblasts, endothelial cells, B cells, CD4+ T cells, CD8+ T cells, macrophages, neutrophils, NK cells, and haematopoietic stem cells (HSC) (Fig. 3b; Supplementary Fig. S1–2). These ten cell types were found in both pre- and post-PDT biopsies (Fig. 3b–d). The T lymphocytes were further divided into four subpopulations: Treg, CTL, NKT, and Th cells (Fig. 3e; Supplementary Fig. S3). Four sub-populations of T cells were also identified in both pre-PDT and post-PDT biopsies (Fig. 3e–g). Subsequently, we made a group comparison. The cell composition of the tumour changed after PDT, as indicated by a great increase in the proportion of B cells, CD4+ T cells, CD8+ T cells, macrophages, and neutrophils, with a decrease in epithelial cells (Fig. 3h). The CTL sub-populations also showed an increase in the post-PDT biopsies, while the proportion of Treg and Th cells decreased (Fig. 3i).

Cell map of gastric cancer by scRNA-seq and intratumoural composition of immune cells before and after PDT. a Thirteen clusters were identified from scRNA-seq data and indicated using a t-SNE plot. b t-SNE plot of all cells showing ten annotated cell types. c t-SNE plot showing the PDT status for all cells. d t-SNE plots showing the distribution of all cell types in pre-PDT and post-PDT biopsies. e Four sub-populations were identified from T lymphocytes and shown in a t-SNE plot. f t-SNE plot showing the PDT status for T lymphocytes. g t-SNE plots showing the distribution of T cell sub-populations in pre-PDT and post-PDT biopsies. h The proportion of each cell type among all cells in pre-PDT and post-PDT biopsies. i The proportion of T cell sub-populations in pre-PDT and post-PDT biopsies. scRNA-seq single-cell RNA sequencing, PDT photodynamic therapy, t-SNE t-distributed stochastic neighbour embedding
Peripheral and histological verification of immunological changes following PDT
Peripheral blood analysis from the same patients showed consistent results: an increase was observed for most of the detected immune cells in the post-PDT biopsies compared to the pre-PDT biopsies if a few exceptions were ignored; however, a decreasing trend for the Treg was detected after PDT despite the inverse observed in one patient (Fig. 4a). Histological assessment of biopsies from two additional patients further confirmed these findings. HE staining of pt4 showed that substantial haemorrhage and necrosis were observed in tumour tissues after PDT and the infiltration of lymphocytes increased in the fibrous stroma of the tumour area (Fig. 4b). A more obvious change of lymphocyte infiltration was observed in pt5. Sparse lymphocytes were detected around the tumour area in the pre-PDT biopsy, but considerable lymphocytes infiltrated within the tumour area and the surrounding fibrous stroma in the post-PDT biopsy (Fig. 4b).

Peripheral and histological changes following PDT. a The proportion of each immune cell in pre-PDT and post-PDT peripheral blood from pt1, pt2 and pt3. b HE stained slices of pre-PDT and post-PDT biopsies from pt4 and pt5. PDT photodynamic therapy, pt patient
The intratumoural TCR repertoire before and after PDT
Clonotypes were identified from the scTCR-seq data and linked to scRNA-seq clusters. Finally, 7236T cells were retained for TCR analysis. Taking all T cells together, the total T cells exhibited an increased frequency of clonal cells after PDT (Fig. 5a, b). When considering the T cell sub-populations separately, the frequency of clonal cells increased after PDT in the sub-populations of CTL and Th cells but decreased in Treg and NKT cells (Fig. 5c, d). The clonotype size (clone amount of a clonotype) was larger in post-PDT (mean size: 2.20) than in pre-PDT biopsies (mean size: 1.60) when assessing T cells together (Fig. 5e). For the sub-populations after PDT, the clonotype size was significantly enlarged in CTL (Post- vs. Pre-PDT, mean size: 6.83 vs 1.98), but slightly contracted in NKT cells (mean size: 1.46 vs 1.53), Treg cells (mean size: 1.10 vs 1.16), and Th cells (mean size: 1.46 vs 1.49) (Fig. 5f). These clonality analyses suggested that CTL expanded greatly, while Treg and NKT cells calmed down in tumour tissues after PDT. We also performed diversity analysis for the total T cells and sub-populations. No difference in diversity was identified for any cell type in the pre-PDT vs. post-PDT biopsies (Supplementary Fig. S4).

The dynamic variation of intratumoural TCR repertoire following PDT. a The proportion of clonal cells in total T cells before and after PDT. Clonal cells were defined as cells with a clonotype that was shared by ≥ 2 cells. b t-SNE plot showing the clonal status of total T cells before and after PDT. c The proportion of clonal cells in each T cell sub-population before and after PDT. d t-SNE plot showing the clonal status of each T cell sub-population before and after PDT. e The distribution of clonotype size in total T cells before and after PDT. f The distribution of clonotype size in each T cell sub-population before and after PDT. Difference was tested using the Mann–Whitney U method. *p < 0.05, **p < 0.01, ***p < 0.001, NS not significant, TCR T cell receptor, PDT photodynamic therapy, t-SNE t-distributed stochastic neighbour embedding
Classification of malignant and non-malignant cells
For epithelial cells, we calculated the malignant and non-malignant scores for each cell and classified them into two clusters (Fig. 6a). Finally, we identified 2628 malignant and 6012 non-malignant epithelial cells (Fig. 6b). A list of the marker genes for gastric cancer cells was determined, and we presented the top ten expressed genes (Fig. 6c, d). We next explored the expression levels of these ten genes in tumour tissues from TCGA stomach cohort. These marker genes were also upregulated in gastric cancer tissues compared to normal tissues in TCGA cohort (Supplementary Fig. S5), which demonstrated the reliability of our identification of malignant cells. According to the clustering results, we observed a slight decrease in the proportion of malignant epithelial cells in the post-PDT group compared to the pre-PDT group (Fig. 6e–g). This suggests that PDT resulted in a change in tumour purity, which was found to be negatively associated with lymphocyte infiltration (Fig. 3h, i).

Classification of epithelial cells as malignant and non-malignant cells. a t-SNE plot showing the epithelial cells coloured according to malignant score minus non-malignant score. b t-SNE plot showing the malignant and non-malignant classifications. c, d t-SNE plots and the corresponding violin plots showing the expression and distribution of top ten malignant cell markers in different clusters. e t-SNE plot showing the PDT status for epithelial cells. f t-SNE plots showing the distribution of malignant and non-malignant cells before and after PDT. g The proportion of malignant and non-malignant cells before and after PDT. t-SNE t-distributed stochastic neighbour embedding, PDT photodynamic therapy
The underlying mechanism of activated anti-tumour immunity after PDT
To explore the possible mechanism underlying the PDT-induced immune response and T-cell expansion, we first performed differential gene analysis on malignant cells before and after PDT. A variety of differential genes were identified following PDT. Among them, we observed that the B2M gene, which is one of the most important genes encoding MHC I molecules, was upregulated in malignant cells after PDT (Fig. 7a, b). The association between B2M and immune cell infiltration was explored using TCGA stomach cohort in the TIMER database. The results showed that the expression of B2M was positively correlated with the levels of infiltrated immune cells (indicated by the reverse correlation with tumour purity), especially with CD8+ T cells, macrophages, neutrophils, and dendritic cells (Fig. 7c). Next, enrichment analysis was performed for differentially expressed genes. We found that several immune-related pathways were enriched after PDT, including the regulation of immune cell activation, proliferation, differentiation, migration, and cytokine and adhesion molecules production (Fig. 7d). We also investigated cell-to-cell communication by calculating ligand-receptor interactions. The malignant cells showed more interactions with NKT cells, Th cells, and CTLs, but less with Tregs in the post-PDT group than in the pre-PDT group (Fig. 7e–g). After PDT, the interactions increased between Th cells and CTLs and decreased between Tregs and other immune cells (Fig. 7e–g). These changes in interactions provided direct evidence that PDT induced an enhanced killing effect by effector cells and removed suppression by Tregs. Several interactions emerged between malignant and immune cells after PDT, including adhesion-mediated (COL16A1_a1b1 complex, VCAM1_a4b1 complex, VCAM1_a4b7 complex, FN1_a5b1 complex), immunostimulatory (PLXNB1_SEMA4D, ALOX5_ALOX5AP, ICAM2_aLb2 complex, CD226_NECTIN2, LTA_TNFRSF1A), and pro-apoptotic/proliferation-inhibiting interactions (EFNA1_EPHA1, EPHA1_EFNA4, EGFR_MIF, LTA_LTBR) involving CTL, NKT, and Th cells (Fig. 7h). In addition, some immunosuppressive interactions disappeared after PDT, including CTLA4_CD80 between Tregs and other immune cells, TGFB1_TGFbeta receptor1 between malignant cells and Tregs, and EPHB6_EFNB1/2 between malignant cells and Th cells (Fig. 7h). Overall, these data suggest that PDT may promote T cell recruitment by upregulating antigen presentation and T cell killing effects by increasing co-stimulatory and decreasing co-inhibitory signaling, resulting in an enhanced specific anti-tumour immune response.

Analysis of potential mechanisms underlying PDT-induced immunity a Volcano plot showing the differential genes comparing malignant cells before and after PDT. b Violin plot showing the expression of the B2M gene in malignant cells before and after PDT. The difference was tested using the Mann–Whitney U method. ***p < 0.001. c Scatterplots showing the correlation between B2M expression with immune cell infiltrations in the TCGA stomach cohort. The correlation analysis was performed using the Spearman method in the TIMER database. d Enrichment analysis of differential genes showing the significant enriched pathways in malignant cells after PDT. e, f Heat maps showing the number of significant cell-to-cell interactions before and after PDT, respectively. g Heat map showing the numerical difference of interactions before and after PDT. The red box indicates more interactions for that cell pair after PDT. Conversely, the blue box indicates more interactions for that cell pair before PDT. h Dot plot showing the changes of significance and strength for specific interactions before and after PDT. PDT photodynamic therapy, TCGA the cancer genome atlas
Discussion
Previous studies have shown that the response to ICIs is significantly associated with T cell infiltration, especially CD8+ T cells [15, 16]. Others also identified a positive association between the proliferation of PD1+CD8+ T cells in peripheral blood and the benefits of ICIs [17, 18]. Several combinations have been developed to address the resistance to ICIs [19, 20], but limited results were achieved. Based on previous findings regarding the increased immune cell infiltration by PDT [7, 21, 22], we assumed that PDT would be helpful in ICI treatment. We thus investigated the effects of PDT in retrospective patients of gastric cancer treated with ICIs. PDT was found to reduce 63% risk of death in the OS of ICI-treated patients and this effect was independent of other clinical features. Furthermore, the timing of PDT usage did not significantly affect its synergistic effect with ICIs, although a longer time interval between PDT and ICI administration showed a diminishing trend in survival benefits. This observation may be attributed to the fact that only patients who received PDT within one month before ICI initiation were included in the analysis. In patients without PDT, those with metastatic diseases had nearly a seven-fold increased risk of death compared to those without metastases. However, the survival difference was eliminated when PDT was combined, suggesting a potential relationship with the abscopal activated effect of PDT. These findings illustrated that PDT can serve as an effective adjuvant approach to alleviate resistance to ICIs and enhance their benefits as long as it is administered within appropriate time intervals prior to ICI treatment. However, its safety was not evaluated owing to incomplete records of adverse events in retrospective data. Based on our experience, the adverse events related to PDT were not common in clinical practice because PDT seldom works outside the tumour tissues causing harm to the entire body. However, whether the combination of PDT and ICIs increases the risk of toxic effects is expected to be further clarified in a well-designed clinical trial. We are currently conducting a clinical trial (Phase 2–3) to investigate the effectiveness and safety of combining PDT with ICIs and chemotherapy. The trial will address unanswered questions from the current retrospective study [23]. Patient recruitment has begun, and we expect to complete the trial in 18 months, following the protocol [23].
When we observed a synergistic effect of PDT and ICIs-based immunotherapy, we are interested in how PDT plays a role in improving ICIs benefits. Thus, we performed a single-cell sequencing experiment accompanied by flow cytometry and histological examination, which allowed us to explore the PDT-induced alteration of anti-tumour immunity from several aspects. Our scRNA-seq data identified ten main classes of cells and four sub-populations of T cells within the gastric cancer microenvironment from three patients. According to the annotated cell types, we found that the alteration in cell composition was pronounced after PDT, as indicated by an increase in most effector immune cells (such as CTLs) and a decrease in suppressive cells (Tregs). Furthermore, the tumour purity, which refers to the proportion of malignant epithelial cells, exhibited a decrease following PDT. Tumour purity has been observed to exhibit an inverse correlation with immune cell infiltration in various types of solid tumours [24]. However, a study conducted on gastric cancer revealed that low tumour purity may not lead to an increase in the number of anti-tumour cells, such as CD8+ and NK cells, in treatment-naïve gastric cancer, likely due to the establishment of a protective shield around gastric cancer cells [25]. In contrast, PDT-induced reduction in tumour purity was accompanied by a significant infiltration and expansion of effector immune cells, indicating a positive indication of immunological regulation. This phenomenon could be attributed to the destruction of the immune evasion shield following the death of malignant cells caused by PDT. HE staining of tumour tissues also indicated a spatial change of immune cells following PDT, which referred to the infiltration of substantial lymphocytes into the tumour area induced by PDT. All these suggest that PDT can reconstruct the tumour immune microenvironment by increasing immune cell infiltration. The peripheral analysis was consistent with the results from scRNA-seq, which further confirmed that PDT affects systemic immunity.
TCR analysis provided an overview of the dynamic variation in the immune repertoire after PDT. We observed PDT-induced enrichment of the T-cell repertoire. After PDT, the clonal cells and clonotype size in CTLs increased greatly, which showed activation of a specific anti-tumour response by PDT. This phenomenon is linked to ICD caused by PDT. Photochemical damage to tumour cells increases the exposure of tumour specific antigens (TSAs), and the processed TSAs are then presented to naïve T cells, resulting in a specific expansion of T cells with TSA-reactive TCR. The presentation of TSAs is often a cross-presentation to CD8+ T cells by dendritic cells [26], which explains why Th cells did not expand greatly following PDT in our study. The clonality of Tregs opposed that of CTLs. The effect was suppressed by PDT, suggesting that PDT relieves immunosuppressive effects induced by Tregs. The diversity analysis of the clonotypes did not show any variation following PDT. This finding is consistent with the hypothesis developed by Hasan et al. [5]. They speculated that PDT did not create any neoantigens but can increase the accessibility of pre-existing antigens to the immune system, which contributes to the enrichment of the TCR repertoire rather than diversification. Our findings supported this hypothesis.
Although PDT-induced immune response has been demonstrated in many studies, the underlying mechanism remains unclear. First, we focused on the tumour cells. We identified a panel of differential genes following PDT in tumour cells and several enriched immune pathways involving various aspects of anti-tumour immunity. We observed that B2M was upregulated after PDT, highlighting the role of PDT in promoting antigen presentation. It should be noted that B2M level was associated with immune cell infiltration and response to ICIs [26, 27]. However, no other genes encoding MHC I were detected in the present study. This limits the comprehensive analysis of the change in antigen presentation capacity in tumour cells following PDT. As antigen presentation is the first step in anti-tumour immunity, PDT can elicit priming, activation, and recruitment of T cells by upregulation of antigen presentation. In addition, during T cell recruitment, the trafficking of T cells into the tumour requires the assistance of both chemokines and adhesion molecules [28]. Pathways related to chemokines and adhesion molecules were enriched in tumour cells following PDT, demonstrating that these mechanisms may also be utilised by PDT to improve T cell infiltration. More cell-to-cell interactions between malignant cells and effector immune cells were identified after PDT, but the opposite phenomenon was observed between Tregs and other cells. This finding provided direct evidence that after PDT, the killing activity against tumour cells increased within the tumour microenvironment. Several immune-related communications between cells were reversed following PDT, including the emergence of immunostimulatory signaling and the disappearance of immunosuppressive signaling. Thus, PDT may enhance the anti-tumour response dependent on the regulation of cell communication.
Our study established a single-cell map of gastric cancer in patients undergoing PDT. We observed an enhanced anti-tumour immune response following PDT and provided clinical evidence supporting the combination strategy of PDT coupled with ICIs. Our study has some limitations. First, only five patients were enrolled for sample detection. The small sample size made it difficult to perform statistical tests between the groups. Second, the histological validation of lymphocyte infiltration was conducted using additional patients. It is important to note that the presence of heterogeneity among patients may introduce a level of indirectness to the validation of the results. Third, scRNA-sequencing was the exclusive technique employed in this study to detect gene expression. The detected number of genes was smaller than that of bulk-RNA sequencing owing to the limitations of scRNA-sequencing. Thus, detection of genes using the bulk-RNA method is required in future studies. Fourth, risk of biases was inevitable in analysing the ICI cohort because of the nature of retrospective study. The results should be verified in future clinical trials with large samples.
In conclusion, we found that PDT influences both systematic and local immune responses in gastric cancer. PDT increases the infiltration of immune cells into tumours and directs the tumour towards a ‘hot’ immunotype. PDT also led to clonal expansion of TSA-specific T cells while suppressing the clonality of Tregs. Several mechanisms have been employed by PDT to promote anti-tumour immunity. PDT may promote T cell activation and trafficking by increasing B2M-dependent antigen presentation. An increase in chemokines and adhesion molecules by tumour cells after PDT may help T cell infiltration. The specific anti-tumour response may be enhanced via cell-to-cell communication by increasing cytotoxic interactions and removing escape interactions. PDT combined with ICIs could prolong survival in patients with gastric cancer and narrow the gap between metastatic and non-metastatic disease, showing the potential of PDT in changing the clinical practice of gastric cancer with ICIs. Cautions should be exercised when applying the findings of this study into clinical practice, as the analyses were conducted using a limited sample size.
Availability of data and materials
All data supporting this study have been presented in the full text or online supplementary files. Other relevant materials can be obtained on reasonable request to the corresponding author.
Abbreviations
- ICIs:
-
Immune checkpoint inhibitors
- PDT:
-
Photodynamic therapy
- ICD:
-
Immunogenic cell death
- scRNA/TCR-seq:
-
Single-cell RNA/T cell receptor (TCR) sequencing
- OS:
-
Overall survival
- HE:
-
Hematoxylin–eosin
- PBS:
-
Phosphate buffered saline
- UMIs:
-
Unique molecule identifiers
- PCA:
-
Principal component analysis
- t-SNE:
-
T-distributed stochastic neighbour embedding
- GO:
-
Gene ontology
- KEGG:
-
Kyoto encyclopedia of genes and genomes
- TCGA:
-
The cancer genome atlas
- NKT:
-
Natural killer T cells
- Th:
-
T helper cells
- Treg:
-
CD4+ regulatory T cells
- CTL:
-
CD8+ cytotoxic T cells
- HRs:
-
Hazard ratios
- CIs:
-
Confidence intervals
- HSC:
-
Haematopoietic stem cells
- TSAs:
-
Tumour specific antigens
References
Yang L, Ying X, Liu S, Lyu G, Xu Z, Zhang X, et al. Gastric cancer: epidemiology, risk factors and prevention strategies. Chin J Cancer Res = Chung-kuo yen cheng yen chiu. 2020;32(6):695–704.
Kahraman S, Yalcin S. Recent advances in systemic treatments for HER-2 positive advanced gastric cancer. Onco Targets Ther. 2021;14:4149–62.
Committee CGW. The Chinese Society of clinical oncology (CSCO): clinical guidelines for the diagnosis and treatment of gastric cancer, 2022. Bei**g: People’s Medical Publishing House; 2022.
Chyuan IT, Chu CL, Hsu PN. Targeting the tumor microenvironment for improving therapeutic effectiveness in cancer immunotherapy: focusing on immune checkpoint inhibitors and combination therapies. Cancers. 2021;13(6):1188.
Nath S, Obaid G, Hasan T. The course of immune stimulation by photodynamic therapy: bridging fundamentals of photochemically induced immunogenic cell death to the enrichment of T-cell repertoire. Photochem Photobiol. 2019;95(6):1288–305.
Falk-Mahapatra R, Gollnick SO. Photodynamic therapy and immunity: an update. Photochem Photobiol. 2020;96(3):550–9.
Beltrán Hernández I, Yu Y, Ossendorp F, Korbelik M, Oliveira S. Preclinical and clinical evidence of immune responses triggered in oncologic photodynamic therapy: clinical recommendations. J Clin Med. 2020;9(2):333.
Cavin S, Gkasti A, Faget J, Hao Y, Letovanec I, Reichenbach M, et al. Low-dose photodynamic therapy promotes a cytotoxic immunological response in a murine model of pleural mesothelioma. Eur J Cardio-thorac Surg Off J Eur Assoc Cardio-thorac Surg. 2020;58(4):783–91.
Kleinovink JW, Fransen MF, Löwik CW, Ossendorp F. Photodynamic-immune checkpoint therapy eradicates local and distant tumors by CD8(+) T cells. Cancer Immunol Res. 2017;5(10):832–8.
Zhang M, Hu S, Min M, Ni Y, Lu Z, Sun X, et al. Dissecting transcriptional heterogeneity in primary gastric adenocarcinoma by single cell RNA sequencing. Gut. 2021;70(3):464–75.
Kumar V, Ramnarayanan K, Sundar R, Padmanabhan N, Srivastava S, Koiwa M, et al. Single-cell atlas of lineage states, tumor microenvironment, and subtype-specific expression programs in gastric cancer. Cancer Discov. 2022;12(3):670–91.
Bassez A, Vos H, Van Dyck L, Floris G, Arijs I, Desmedt C, et al. A single-cell map of intratumoral changes during anti-PD1 treatment of patients with breast cancer. Nat Med. 2021;27(5):820–32.
Li T, Fan J, Wang B, Traugh N, Chen Q, Liu JS, et al. TIMER: a web server for comprehensive analysis of tumor-infiltrating immune cells. Can Res. 2017;77(21):e108–10.
Efremova M, Vento-Tormo M, Teichmann SA, Vento-Tormo R. Cell PhoneDB: inferring cell-cell communication from combined expression of multi-subunit ligand-receptor complexes. Nat Protoc. 2020;15(4):1484–506.
Li F, Li C, Cai X, **e Z, Zhou L, Cheng B, et al. The association between CD8+ tumor-infiltrating lymphocytes and the clinical outcome of cancer immunotherapy: a systematic review and meta-analysis. EClinicalMedicine. 2021;41:101134.
Gide TN, Quek C, Menzies AM, Tasker AT, Shang P, Holst J, et al. Distinct immune cell populations define response to anti-PD-1 monotherapy and anti-PD-1/anti-CTLA-4 combined therapy. Cancer Cell. 2019;35(2):238-55.e6.
Kim KH, Cho J, Ku BM, Koh J, Sun JM, Lee SH, et al. The first-week proliferative response of peripheral blood PD-1(+)CD8(+) T cells predicts the response to anti-PD-1 therapy in solid tumors. Clin Cancer Res Off J Am Assoc Cancer Res. 2019;25(7):2144–54.
Kamphorst AO, Pillai RN, Yang S, Nasti TH, Akondy RS, Wieland A, et al. Proliferation of PD-1+ CD8 T cells in peripheral blood after PD-1-targeted therapy in lung cancer patients. Proc Natl Acad Sci USA. 2017;114(19):4993–8.
Vafaei S, Zekiy AO, Khanamir RA, Zaman BA, Ghayourvahdat A, Azimizonuzi H, et al. Combination therapy with immune checkpoint inhibitors (ICIs); a new frontier. Cancer Cell Int. 2022;22(1):2.
Yan YD, Cui JJ, Fu J, Su YJ, Chen XY, Gu ZC, et al. A Network comparison on safety profiling of immune checkpoint inhibitors in advanced lung cancer. Front Immunol. 2021;12:760737.
Theodoraki MN, Lorenz K, Lotfi R, Fürst D, Tsamadou C, Jaekle S, et al. Influence of photodynamic therapy on peripheral immune cell populations and cytokine concentrations in head and neck cancer. Photodiagn Photodyn Ther. 2017;19:194–201.
Hass R, Jacobs R, Kaufmann AM, Hillemanns P, Soergel P. Sensitization of immune cells following hexylaminolevulinate photodynamic therapy of cervical intraepithelial neoplasia. Photodiagn Photodyn Ther. 2017;17:82–6.
Yu Y, Yu R, Wang N, Bai Y, Shi Q, Maswikiti EP, et al. Photodynamic therapy in combination with immune checkpoint inhibitors plus chemotherapy for first-line treatment in advanced or metastatic gastric or gastroesophageal junction cancer: a phase 2–3 clinical trial protocol. Front Pharmacol. 2023;14:1063775.
Rhee JK, Jung YC, Kim KR, Yoo J, Kim J, Lee YJ, et al. Impact of tumor purity on immune gene expression and clustering analyses across multiple cancer types. Cancer Immunol Res. 2018;6(1):87–97.
Lou S, Zhang J, Yin X, Zhang Y, Fang T, Wang Y, et al. Comprehensive characterization of tumor purity and its clinical implications in gastric cancer. Front Cell Dev Biol. 2021;9:782529.
Jhunjhunwala S, Hammer C, Delamarre L. Antigen presentation in cancer: insights into tumour immunogenicity and immune evasion. Nat Rev Cancer. 2021;21(5):298–312.
Wang H, Liu B, Wei J. Beta2-microglobulin(B2M) in cancer immunotherapies: biological function, resistance and remedy. Cancer Lett. 2021;517:96–104.
Chen DS, Mellman I. Elements of cancer immunity and the cancer-immune set point. Nature. 2017;541(7637):321–30.
Acknowledgements
The authors would like to thank BMKCloud (http://www.biocloud.net/) for providing supports in data process, management and figure drawing. We thank Chen Yu, Tianliang Lu, and Rui Zhang for their advice in bioinformatics analysis and ** Bai, Peng Zheng, Chenhui Ma, Bofang Wang, Xueyan Wang & Hao Chen
Contributions
YY and HC: had the idea of this study. YY and HC: conceived and designed the study. YY: performed most of the experiments, including single-cell sequencing, flow cytometry, and data analysis. BX, LX, NW, RY, and LG: contributed to the recruitment and management of patients. TLD, EPM, BX, and YPW: performed sample collection. HYL and BHG: helped with the processing and preparation of single-cell suspensions. CHM, BFW, and XYW: collected patient information and made the follow-up. YY and TZ: generated the statistical strategy. YY: visualised and interpreted the results and drafted the manuscript. YPB, LX, PZ and HC: provided clinical perspectives for the interpretation of results. HC and LX: reviewed and revised the manuscript. HC obtained funding to support all aspects of this study. YY and HC: have read and verified the underlying data. All authors read and approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval and consent to participate
This study was approved by the Institutional Research Ethics Committee of the Lanzhou University Second Hospital (2021A-146). Informed consent was obtained from all included patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yu, Y., Xu, B., **ang, L. et al. Photodynamic therapy improves the outcome of immune checkpoint inhibitors via remodelling anti-tumour immunity in patients with gastric cancer. Gastric Cancer 26, 798–813 (2023). https://doi.org/10.1007/s10120-023-01409-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-023-01409-x