
Abstract
Summary
We examined variations in proportions of hip fractures and major fractures among postmenopausal women using the Global Longitudinal Study of Osteoporosis in Women (GLOW). The proportion of major fractures that were hip fractures varied with age and region, whereas variations in the proportion of fractures that were major fractures appeared modest.
Introduction
In many countries, the World Health Organization fracture risk assessment tool calculates the probability of major fractures by assuming a uniform age-associated proportion of major fractures that are hip fractures in different countries. We further explored this assumption, using data from the GLOW.
Methods
GLOW is an observational population-based study of 60,393 non-institutionalized women aged ≥55 years who had visited practices within the previous 2 years. Main outcome measures were self-reported prevalent fractures after the age of 45 years and incident fractures during the 2 years of follow-up.
Results
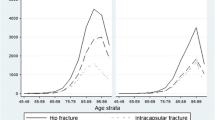
The adjusted proportion of prevalent and incident major fractures after the age of 45 years that were hip fractures was higher in North America (16%, 17%) than in northern (13%, 12%) and southern Europe (10%, 10%), respectively. The proportion of incident major fractures that were hip fractures increased more than five-fold with age, from 6.6% among 55–59-year-olds to 34% among those aged ≥85 years. Regional and age-associated variations in the proportion of all incident fractures that were major fractures were less marked, not exceeding 16% and 28%, respectively.
Conclusions
The data suggest that there may be regional differences in the proportion of major fractures that are hip fractures in postmenopausal women. In contrast, the regional and age-related variations in the proportion of fractures that are major fractures appear to be modest. However, because of the limited number of fractures in our sample, further studies are necessary to confirm these findings.

Similar content being viewed by others

References
Kanis JA, Oden A, Johnell O, Jonsson B, de Laet C, Dawson A (2001) The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int 12:417–427
Kanis JA, Johansson H, Oden A, Dawson-Hughes B, Melton LJ 3rd, McCloskey EV (2010) The effects of a FRAX revision for the USA. Osteoporos Int 21:35–40
Johansson H, Kanis JA, McCloskey EV, Odén A, Devogelaer JP, Kaufman JM, Neuprez A, Hiligsmann M, Bruyere O, Reginster JY (2011) A FRAX® model for the assessment of fracture probability in Belgium. Osteoporos Int 22:453–461
Leslie WD, Lix LM, Langsetmo L, Berger C, Goltzman D, Hanley DA, Adachi JD, Johansson H, Oden A, McCloskey E, Kanis JA (2011) Construction of a FRAX® model for the assessment of fracture probability in Canada and implications for treatment. Osteoporos Int 22:817–827
Ettinger B, Black DM, Dawson-Hughes B, Pressman AR, Melton LJ 3rd (2010) Updated fracture incidence rates for the US version of FRAX. Osteoporos Int 21:25–33
Kanis JA, Johnell O, Oden A, Sembo I, Redlund-Johnell I, Dawson A, De Laet C, Jonsson B (2000) Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int 11:669–674
Leslie WD, Lix LM (2010) Manitoba Bone Density Program. Imputation of 10-year osteoporotic fracture rates from hip fractures: a clinical validation study. J Bone Miner Res 25:388–392
Adachi JD, Ioannidis G, Pickard L, Berger C, Prior JC, Joseph L, Hanley DA, Olszynski WP, Murray TM, Anastassiades T, Hopman W, Brown JP, Kirkland S, Joyce C, Papaioannou A, Poliquin S, Tenenhouse A, Papadimitropoulos EA (2003) The association between osteoporotic fractures and health-related quality of life as measured by the Health Utilities Index in the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int 14:895–904
Adachi JD, Adami S, Gehlbach S, Anderson FA Jr, Boonen S, Chapurlat RD, Compston JE, Cooper C, Delmas P, Díez-Pérez A, Greenspan SL, Hooven FH, LaCroix AZ, Lindsay R, Netelenbos JC, Wu O, Pfeilschifter J, Roux C, Saag KG, Sambrook PN, Silverman S, Siris ES, Nika G, Watts NB, GLOW Investigators (2010) Impact of prevalent fractures on quality of life: baseline results from the Global Longitudinal Study of Osteoporosis in Women. Mayo Clin Proc 85:806–813
Hooven FH, Adachi JD, Adami S, Boonen S, Compston J, Cooper C, Delmas P, Diez-Perez A, Gehlbach S, Greenspan SL, LaCroix A, Lindsay R, Netelenbos JC, Pfeilschifter J, Roux C, Saag KG, Sambrook P, Silverman S, Siris E, Watts NB, Anderson FA Jr (2009) The Global Longitudinal Study of Osteoporosis in Women (GLOW): rationale and study design. Osteoporos Int 20:1107–1116
Ware JE, Kosinski M, Dewey JE (2000) How to score version 2 of the SF-36 Heath Survey. Quality Metric, Lincoln
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19:385–397
Kanis JA, McCloskey EV, Johansson H, Oden A, Ström O, Borgström F (2010) Development and use of FRAX in osteoporosis. Osteoporos Int 21(Suppl 2):S407–S413
Kanis JA, Johnell O, Oden A, Dawson A, De Laet C, Jonsson B (2001) Ten year probabilities of osteoporotic fractures according to BMD and diagnostic thresholds. Osteoporos Int 12:989–995
Díez-Pérez A, Hooven FH, Adachi JD, Adami S, Anderson FA, Boonen S, Chapurlat R, Compston JE, Cooper C, Delmas P, Greenspan SL, Lacroix AZ, Lindsay R, Netelenbos JC, Pfeilschifter J, Roux C, Saag KG, Sambrook P, Silverman S, Siris ES, Watts NB, Nika G, Gehlbach SH (2011) Regional differences in treatment for osteoporosis. The Global Longitudinal Study of Osteoporosis in Women (GLOW). Bone 49:493–498
Leslie WD, Sadatsafavi M, Lix LM, Azimaee M, Morin S, Metge CJ, Caetano P (2010) Secular decreases in fracture rates 1986–2006 for Manitoba, Canada: a population-based analysis. Osteoporos Int 7:2137–2143
Sanders KM, Seeman E, Ugoni AM, Pasco JA, Martin TJ, Skoric B, Nicholson GC, Kotowicz MA (1999) Age- and gender-specific rate of fractures in Australia: a population-based study. Osteoporos Int 10:240–247
Bergström U, Jonsson H, Gustafson Y, Pettersson U, Stenlund H, Svensson O (2009) The hip fracture incidence curve is shifting to the right. Acta Orthop 80:520–524
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Järvinen M (2006) Nationwide decline in incidence of hip fracture. J Bone Miner Res 21:1836–1838
Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P, Rapin CH, Rizzoli R (2007) Incidence of hip fracture over a 10-year period (1991–2000): reversal of a secular trend. Bone 40:1284–1289
Leslie WD, O’Donnell S, Jean S, Lagacé C, Walsh P, Bancej C, Morin S, Hanley DA, Papaioannou A (2009) Osteoporosis Surveillance Expert Working Group. Trends in hip fracture rates in Canada. JAMA 302:883–889
Dimai HP, Svedbom A, Fahrleitner-Pammer A, Pieber T, Resch H, Zwettler E, Chandran M, Borgström F (2011) Epidemiology of hip fractures in Austria: evidence for a change in the secular trend. Osteoporos Int 22:685–692
Maravic M, Taupin P, Landais P, Roux C (2011) Change in hip fracture incidence over the last 6 years in France. Osteoporos Int 22:797–801
Gehlbach SH, Avrunin JS, Puleo E (2007) Trends in hospital care for hip fractures. Osteoporos Int 18:585–591
Siris ES, Brenneman SK, Barrett-Connor E, Miller PD, Sajjan S, Berger ML, Chen YT (2006) The effect of age and bone mineral density on the absolute, excess, and relative risk of fracture in postmenopausal women aged 50–99: results from the National Osteoporosis Risk Assessment (NORA). Osteoporos Int 17:565–574
Icks A, Haastert B, Wildner M, Becker C, Meyer G (2008) Trend of hip fracture incidence in Germany 1995–2004: a population-based study. Osteoporos Int 19:1139–1145
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22:465–475
Nevitt MC, Cummings SR, Browner WS, Seeley DG, Cauley JA, Vogt TM, Black DM (1992) The accuracy of self-report of fractures in elderly women: evidence from a prospective study. Am J Epidemiol 135:490–499
Ismail AA, O’Neill TW, Cockerill W, Finn JD, Cannata JB, Hoszowski K, Johnell O, Matthis C, Raspe H, Raspe A, Reeve J, Silman AJ, EPOS Study Group, European Prospective Osteoporosis Study Group (2000) Validity of self-report of fractures: results from a prospective study in men and women across Europe. Osteoporos Int 11:248–254
Ivers RQ, Cumming RG, Mitchell P, Peduto AJ (2002) The accuracy of self-reported fractures in older people. J Clin Epidemiol 55(5):452–457
Chen Z, Kooperberg C, Pettinger MB, Bassford T, Cauley JA, LaCroix AZ, Lewis CE, Kipersztok S, Borne C, Jackson RD (2004) Validity of self-report for fractures among a multiethnic cohort of postmenopausal women: results from the Women’s Health Initiative observational study and clinical trials. Menopause 11:264–274
Rapp K, Becker C, Lamb SE, Icks A, Klenk J (2008) Hip fractures in institutionalized elderly people: incidence rates and excess mortality. J Bone Miner Res 23:1825–1831
Dennis MS, Lo KM, McDowall M, West T (2002) Fractures after stroke: frequency, types, and associations. Stroke 33:728–734
Ramnemark A, Nyberg L, Borssén B, Olsson T, Gustafson Y (1998) Fractures after stroke. Osteoporos Int 8:92–95
Acknowledgments
We thank the physicians and project coordinators participating in GLOW. Editorial support for the final version of this article, comprising language editing, content checking, formatting, and referencing was provided by Sophie Rushton-Smith, Ph.D. Financial support for the GLOW study is provided by Warner Chilcott Company, LLC and sanofi-aventis to the Center for Outcomes Research, University of Massachusetts Medical School.
Conflicts of interest
Johannes Pfeilschifter has received a research grant from AMGEN, Kyphon, Novartis, and Roche and other research support like the equipment from GE LUNAR; has served on the speakers’ bureau for AMGEN, sanofi-aventis, GlaxoSmithKline, Roche, Lilly Deutschland, Orion Pharma, Merck Sharp and Dohme, Merckle, Nycomed, and Procter & Gamble; and has served as an advisory board member for Novartis, Roche, Procter & Gamble, and TEVA.
Cyrus Cooper has received consulting fees and lectured for AMGEN, The Alliance for Better Bone Health (sanofi-aventis and Warner Chilcot), Eli Lily, Merck Sharp and Dohme, Servier, Novartis, and Roche-GSK.
Nelson B. Watts has no stock options/holdings, royalties, company owner, patent owner, and official role to declare; has received honoraria for lectures in the past year from Amgen, Novartis, Procter & Gamble, and sanofi-aventis and consulting fees in the past year from Amgen, Baxter, InteKrin, Johnson & Johnson, MannKind, Novo Nordisk, NPS, Pfizer, Procter & Gamble, sanofi-aventis, Takeda Pharmaceuticals, and Warner Chilcott; and has received research support (through University) from Amgen, Eli Lilly, Merck, and NPS.
Julie Flahive has received a research grant from The Alliance for Better Bone Health (sanofi-aventis and Warner Chilcot).
Stephen Gehlbach has received a research grant from The Alliance for Better Bone Health (sanofi-aventis and Warner Chilcot).
Frederick H. Hooven has received a research grant from The Alliance for Better Bone Health (sanofi-aventis and Warner Chilcot).
Kenneth G. Saag has served on the speakers’ bureau for Novartis; has received consulting fees or other remuneration from Eli Lilly & Co., Merck, Novartis, Amgen, Roche, Procter & Gamble, and sanofi-aventis; has been undertaking paid research for Eli Lilly & Co, Merck, Novartis, Amgen, Procter & Gamble, and sanofi-aventis; and has served as an advisory committee or other paid committee member for Eli Lily & Co.
Jonathan D. Adachi has served as a consultant/speaker for Amgen, Astra Zeneca, Eli Lilly, GlaxoSmithKline, Merck, Novartis, Nycomed, Pfizer, Procter & Gamble, Roche, sanofi-aventis, Servier, Wyeth, and Bristol-Myers Squibb; has undertaken clinical trials for Amgen, Eli Lilly, GlaxoSmithKline, Merck, Novartis, Pfizer, Procter & Gamble, Roche, sanofi-aventis, Wyeth, and Bristol-Myers Squibb; and has no stocks to declare.
Steven Boonen has received a research grant from Amgen, Eli Lilly, Novartis, Pfizer, Procter & Gamble, sanofi-aventis, Roche, and GlaxoSmithKline; has served on the speakers’ bureau for Amgen, Eli Lilly, Merck, Novartis, Procter & Gamble, sanofi-aventis, and Servier; has received honoraria from Amgen, Eli Lilly, Merck, Novartis, Procter & Gamble, sanofi-aventis, and Servier; and has served as a consultant/advisory board member for Amgen, Eli Lilly, Merck, Novartis, Procter & Gamble, sanofi-aventis, and Servier. He is also a senior clinical investigator of the Fund for Scientific Research, Flanders, Belgium (FWO-Vlaanderen) and holder of the Leuven University Chair in Metabolic Bone Diseases
Roland Chapurlat has received research grants from French Ministry of Health, Merck, Servier, Lilly, and Procter & Gamble; has not yet served on the speakers’ bureau; has received honoraria from Amgen, Servier, Novartis, Lilly, Roche, and sanofi-aventis; and has served as a consultant/advisory board member for Amgen, Merck, Servier, Nycomed, and Novartis.
Juliet Compston has been undertaking paid consultancy work for Servier, Shire, Nycomed, Novartis, Amgen, Procter & Gamble, Wyeth, Pfizer, Alliance for Better Bone Health, Roche, and GlaxoSmithKline and paid speaking engagements, reimbursement, and travel and accommodation for Servier, Procter & Gamble, and Eli Lilly; has received research grants from Servier R&D and Procter & Gamble; and has no stocks or shares in relevant companies.
Adolfo Diez-Perez has received honoraria from Novartis, Eli Lilly, Amgen, Procter & Gamble, and Roche and has served as an expert witness for Merck and a consultant/advisory board member for Novartis, Eli Lilly, Amgen, and Procter & Gamble.
Susan L. Greenspan has served as a consultant/advisory board member for Amgen, Lilly, and Merck and received research grants from The Alliance for Better Bone Health (sanofi-aventis and Procter & Gamble) and Lilly.
Andrea LaCroix has received support from The Alliance for Better Bone Health (sanofi-aventis and Warner Chilcot).
J. Coen Netelenbos has been undertaking paid consultancy work for Roche Diagnostics, Daiichi-Sankyo, Procter & Gamble, and Nycomed and paid speaking engagements, reimbursement, and travel and accommodation for Roche Diagnostics, Novartis, Daiichi-Sankyo, and Procter & Gamble and has received research grants from Alliance for Better Bone Health and Amgen.
Maurizio Rossini has served as a speaker for Roche, Merck Sharp & Dohme, and GlaxoSmithKline.
Christian Roux has received honoraria from Alliance, Amgen, Lilly, Merck Sharp and Dohme, Novartis, Nycomed, Roche, GlaxoSmithKline, Servier, and Wyeth and has served as a consultant/advisory board member for Alliance, Amgen, Lilly, Merck Sharp and Dohme, Novartis, Nycomed, Roche, GlaxoSmithKline, Servier, and Wyeth.
Philip N. Sambrook has received honoraria from Merck, sanofi-aventis, Roche, and Servier and has served as a consultant/advisory board member for Merck, sanofi-aventis, Roche, and Servier.
Stuart Silverman has received research grants from Wyeth, Lilly, Novartis, and Alliance; has served on the speakers’ bureau for Lilly, Novartis, Pfizer, and Procter & Gamble; has received honoraria from Procter & Gamble; and has served as a consultant/advisory board member for Lilly, Argen, Wyeth, Merck, Roche, and Novartis.
Ethel S. Siris has served as a consultant for Amgen, Lilly, Novartis, and The Alliance for Better Bone Health and has served on the speakers’ bureau for Amgen and Lilly.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pfeilschifter, J., Cooper, C., Watts, N.B. et al. Regional and age-related variations in the proportions of hip fractures and major fractures among postmenopausal women: the Global Longitudinal Study of Osteoporosis in Women. Osteoporos Int 23, 2179–2188 (2012). https://doi.org/10.1007/s00198-011-1840-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-011-1840-6