
Abstract
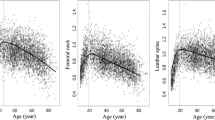
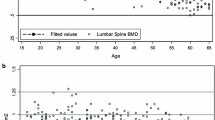
The BMD reference curve is the reference value used for diagnosing osteoporosis and assessing bone mass changes. Its accuracy would affect the correctness of T -score and Z -score values and thus the reliability of diagnostic results. In this paper, we report the use of a new method, a Cartesian coordinate numeration system, to establish BMD reference curves at different skeletal sites in women. In a reference population of 3,919 women ranging in age from 5–85 years, we used the dual X-ray absorptiometry (DXA) bone densitometer to measure BMD at the posteroanterior spine (PA; vertebrae L1–L4), followed by a paired PA/lateral spine scan of the vertebral bodies of L2–L4, expressed in g/cm2 and g/cm3, and of the hip and forearm. We chose the cubic regression model to best fit BMD curves that varied with age at different skeletal sites. We then referred the BMD of the fitting curves established by the method of the coordinate numeration system as reference curves, compared them to BMD reference curves derived from the fitting curve equation or age cross-section, and calculated the deflection degrees of the BMD reference curves acquired from the fitting curve equation. At the PA spine, lateral spine (expressed in g/cm3), femoral neck, Ward’s triangle and radius + ulna ultradistal, the reference curves calculated from the equation were significantly lower than those confirmed by the method of the coordinate numeration system; whereas, at the lateral spine (expressed in g/cm2), total hip, and radius + ulna 1/3 sites, the reference curves derived from the equation were markedly higher than those acquired from the coordinate numeration system. The differences in the two kinds of reference curves calculated by these two different methods gradually increased along with the increment in ages of the women. At the peak value of the reference curves, the BMD calculated from the equation deflected from 2.02% to −10.0% from the BMD acquired from the coordinate numeration system at different skeletal sites, and from 21.5% to −121.8% until the age of 85 years. The highest positive deflection of 65.2% existed at the lateral spine (expressed in g/cm2) and the lowest positive deflection of 21.5% at the total hip. The maximum negative deflection of −121.8% was at the radius + ulna ultradistal, and the minimum negative deflection of −32.6% at the PA spine. The BMD curve acquired from age cross-section was highly positive compared with the one derived from the coordinate numeration system ( r =0.955–0.985 p =0.000) with no significant difference between them. Various analysts used such a method to obtain the coefficient of variance (CV) in BMD precision on each curve that was from 0.05–0.19%. Our study shows that the Cartesian coordinate numeration system is an accurate, precise and reliable method and can serve to reveal the serious drawbacks of using the fitting curve equation to calculate BMD. The BMD reference curves established by this coordinate numeration system maintained the authenticity of the fitting curve, whereas, using the fitting curve equation to obtain BMD reference curves at different skeletal sites led to distortion, and resulted in false increases or decreases in T -score and Z -score values.



Similar content being viewed by others

References
Njeh CF, Boivin CM, Langton CM (1997) The role of ultrasound in the assessment of osteoporosis: a review. Osteoporos Int 7:7–22
Fujiwara S (1995) Estimating incidence of osteoporosis by bone mineral density, from population based study (in Japanese). Jyouju Kagaku Kenkyuu Kenkyuuhoukoku (Report of Aging and Health Research) 4:508–511
Conference Report (1993) Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 94:646–650
Ray NF, Chan JK, Thamer M, Melton LJ 3rd (1997) Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 12:24–35
Liu ZH, Piao JH, Pang LP et al (2002) The diagnostic criteria for primary osteoporosis and the incidence of osteoporosis in China. J Bone Miner Metab 20:181–189
Block JE, Smith R, Glueer CC, Steiger P, Ettinger B, Genant HK (1989) Models of spinal trabecular bone loss as determined by quantitative computed tomography. J Bone Miner Res 4:249–257
Kelly TL (1990) Bone mineral density reference databases for American men and women. J Bone Miner Res 5 [Suppl 2]:S249
Martin JC, Reid DM (1999) Radial bone mineral density and estimated rates of change in normal Scottish women: assessment by peripheral quantitative computed tomography. Calcif Tissue Int 64:126–132
** W et al (2000) Bone mineral density differences at the femoral neck and Ward’s triangle: a comparison study on the reference data between Chinese and Caucasian women. Calcif Tissue Int 67:195–198
Liao EY, Wu XP, Deng XG et al (2002) Age-related bone mineral density, accumulated bone loss rate and prevalence of osteoporosis at multiple skeletal sites in Chinese women. Osteoporos Int 13:669–676
Liao EY, Wu XP, Luo XH, Zhang H, Dai RC, Huang G (2003) Establishment and evaluation of bone mineral density reference databases appropriate for diagnosis and evaluation of osteoporosis in Chinese women. J Bone Miner Metab 21:185–193
Wu XP, Liao EY, Huang G, Dai RC, Zhang H (2003) A comparison study of the reference curves of bone mineral density at different skeletal sites in native Chinese, Japanese, and American Caucasian women. Calcif Tissue Int 73:122–132
Wu XP, Liao EY, Zhang H, Shan PF, Cao XZ, Liu SP (2004) Establishment of BMD reference plots and determination of peak BMD at multiple skeletal regions in mainland Chinese women and the diagnosis of osteoporosis. Osteoporos Int 15:71–79
Kelly TL (1992) Study protocol QDR reference databases. Hologic, Bedford, MA, USA
Bonnick SL, Johnston CC Jr, Kleerekoper M et al (2001) Importance of precision in bone density measurements. J Clin Densitom 4:105–110
QDR 4500 X-ray bone densitometer User’s Guide (1996) Reference database and reports. Hologic, Bedford, MA, USA. Chapter 8–8
Acknowledgements
We wish to thank two anonymous reviewers for comments that helped to improve the manuscript
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wu, XP., Dai, RC., Shan, PF. et al. Establishment of BMD reference curves at different skeletal sites in women, using a Cartesian coordinate numeration system. Osteoporos Int 16, 1655–1662 (2005). https://doi.org/10.1007/s00198-005-1898-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-005-1898-0