
Abstract
Purpose
Lidocaine diffuses across endotracheal tube cuffs, which may serve as a reservoir for local anesthetic to assist in the prevention of ETT-induced cough while emerging from general anesthesia. However, the rate of diffusion is slow. Two techniques, alkalization and warming, may increase the proportion of uncharged drug available for diffusion. The purpose of this study is to determine the effectiveness of warming alkalization or warming with alkalization on diffusion.
Methods
Four preparations of lidocaine 4% were studied. Group (Gr) L-lidocaine (24°C), Gr WL — warmed lidocaine (38°C), Gr AL — alkalized lidocaine (24°C), Gr WAL — warmed, alkalized lidocaine (38°C). Twenty-four Mallinckrodt 8.0 ID (Mallinckrodt Critical Care Division of Mallinckrodt, Inc., Glens Falls, New York) endotracheal tube cuffs were filled with 6 ml of one of the four preparations. They were then placed in a 20 ml water bath at 38°C and samples were drawn from the water bath at intervals for up to 360 min. The lidocaine concentration in each sample was determined by gas chromatography.
Results
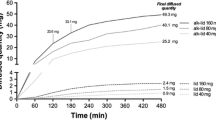
The highest lidocaine concentration was reached in Gr WAL (410.98 ± 8.53 μ·ml−1) after 300 min and then decreased to 376.18 ± 4.59 μ·ml−1 after 360 min. In Gr AL the highest concentration (235.05 ± 2.99 μ·ml−1) was reached after 360 min. Lidocaine concentrations in Gr L and WL after 360 min were 3.19 ± 1.16 μ·ml−1 and 4.32 ± 2.02 μ·ml−1 respectively.
Conclusion
Alkalization with or without warming, but not warming alone, promotes lidocaine diffusion from endotracheal tube cuff.
Résumé
Objectif
La lidocaine diffuse, lentement toutefois, au travers des ballonnets des tubes endotrachéaux. Les ballonnets peuvent servir de réservoir à l’anesthésique local et participer à la prévention de la toux induite par le TET pendant la récupération de l’anesthésie générale. L’alcalinisation et le réchauffement peuvent accroître la proportion de médicament susceptible de diffuser. Lobjectif de la présente étude est de déterminer l’efficacité du réchauffement, seul ou avec alcalinisation, sur la diffusion.
Méthode
On a étudié quatre préparations de lidocaïne. Le groupe (Gr) L-lidocaïne (24 °C), Gr LR — lidocaïne réchauffée (38 °C), Gr LA — lidocaïne alcalinisée (24 °C), Gr LRA - lidocaïne réchauffée, alcalinisée (38 °C). Vingtquatre tubes endotrachéaux à ballonnets Mallinckrodt de Dl 8,0 (Mallinckrodt Critical Care Division of Mallinckrodt, Inc., Glens Falls, New York) ont été remplis de 6 ml de l’une des préparations. Placés ensuite dans un bain d’eau de 20 ml à 38 °C, on en a ensuite retiré des échantillons à des intervalles pouvant aller jusqu’à 360 min. La concentration de lidocaïne a été déterminée par Chromatographie en phase gazeuse.
Résultats
La plus forte concentration de lidocaïne a été atteinte dans le Gr LRA, 410,98 ± 8,53 μ·ml−1, après 300 min, puis elle a baissé à 376,18 ± 4,59 μ·ml−1 après 360 min. Dans le Gr LA, la concentration maximale était de 235,05 ± 2,99 μ·ml−1 après 360 min. Dans les Gr L et LR, la lidocaïne était, après 360 min de 3,19 ± 1,16 μ·ml−1 et de 4,32 ± 2,02 μ·ml−1 respectivement.
Conclusion
Lalcalinisation avec ou sans réchauffement, mais non le réchauffement employé seul, favorise la diffusion de la lidocaïne au travers du ballonnet du tube endotrachéal.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Bidwai AV, Bidwai VA, Rogers CR, Stanley TH. Blood-pressure and pulse-rate responses to endotracheal extubation with and without prior injection of lidocaine. Anesthesiology 1979; 51: 171–3.
Leech P, Barker J, Fitch W. Changes in intracranial pressure and systemic arterial pressure during the termination of anaesthesia. Br J Anaesth 1974; 46: 315–6.
Gonzalez RM, Bjerke RJ, Drobycki T, et al. Prevention of endotracheal tube-induced coughing during emergence from general anesthesia. Anesth Analg 1994; 79: 792–5.
Steinhaus JE, Gaskin L. A study of intravenous lidocaine as a suppressant of cough reflex. Anesthesiology 1963; 24: 285–90.
Poulton TJ, James FM III. Cough suppression by lidocaine. Anesthesiology 1979; 50: 470–2.
Gefke K, Andersen LW, Friesel E. Lidocaine given intravenously as a suppressant of cough and laryngospasm in connection with extubation after tonsillectomy. Acta Anaesthesiol Scand 1983; 27: 111–2.
Christensen V, Ladegaard-Pedersen HJ, Skovsted P. Intravenous lidocaine as a suppressant of persistent cough caused by bronchoscopy. Acta Anaesthesiol Scand 1978; 67(Suppl): 84–6.
Tukioka H, Yoshimoto N, Nishimura K, Fujimori M. Intravenous lidocaine as a suppressant of coughing during tracheal intubation. Anesth Analg 1985; 64: 1189–92.
Nishino T, Hiraga K, Sugimori K. Effects of i.v. lignocaine on airway reflexes elicited by irritation of the tracheal mucosa in humans anaesthetized with enflurane. Br J Anaesth 1990; 64: 682–7.
Bartlett D Jr, Jeffrey P, Sant’Ambrogio G, Wise JCM. Location of stretch receptors in the tracheal and bronchi of the dog. J Physiol (Lond) 1976; 258: 409–20.
Camporesi EM, Mortola JP, Sant’Ambrogio F, Sant’Ambrogio G. Topical anesthesia of tracheal receptors. J Appl Physiol 1979; 47: 1123–6.
Strobel GE, Bianchi CP. The effects of pH gradients on the uptake and distribution of C14-procaine and lidocaine in intact and desheathed sciatic nerve trunks. J Pharmacol Exp Ther 1970; 172: 18–32.
Sconzo JM, Moscicki JC, Difazio CA.In vitro diffusion of lidocaine across endotracheal tube cuffl. Reg Anesth 1990; 15: 37–40.
dejong RH. Cm-The minimum blocking concentration.In: dejong RH (Ed.). Local Anesthetics. Springfield, Illinois: Charles C Thomas, 1977: 51–62.
Butterworth JF, Strichartz GR. Molecular mechanisms of local anesthesia: a review. Anesthesiology 1990; 72: 711–34.
Sanchez V, Arthur GR, Strichartz GR. Fundamental properties of local anesthetics. I. The dependence of lidocaine’s ionization and octanol: buffer partitioning on solvent and temperature. Anesth Analg 1987; 66: 159–65.
Strichartz GR, Sanchez V, Arthur GR, Chafetz R, Martin D. Fundamental properties of local anesthetics. II. Measured octanol: buffer partition coefficients and pKa values of clinically used drugs. Anesth Analg 1990; 71: 158–70.
Difazio CA, Carron H, Grosslight KR, Moscicki JC, Bolding WR, Johns RA. Comparison of pH-adjusted lidocaine solutions for epidural anesthesia. Anesth Analg 1986; 65: 760–4.
Fernando R, Jones HM. Comparison of plain and alkalinized local anaesthetic mixtures of lignocaine and bupivacaine for elective extradural Caesarean section. Br J Anaesth 1991; 67: 699–703.
Galindo A. pH-Adjusted local anesthetics: clinical experience. Reg Anaesth 1983; 8: 35–6.
Clark V, McGardy E, Sugden C, Dickson J, McLeod G. Speed of onset of sensory block for elective extradural Caesarean section: choice of agent and temperature of injectate. Br J Anaesth 1994;72: 221–3.
Matias E. Effect of NaHCO3 On the diffusion of lignocaine through the wall of endotracheal tube’s cuff. Br J Anaesth 1995; 74: A.238.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by a grant of the Mackay Memorial Hospital, Taipei, Taiwan, R.O.C. (MME-8503).
Rights and permissions
About this article
Cite this article
Huang, CJ., Tsai, MC., Chen, CT. et al. In vitro diffusion of lidocaine across endotracheal tube cuffs. Can J Anesth 46, 82–86 (1999). https://doi.org/10.1007/BF03012520
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012520