
Summary
Since 1980 we have performed valgus tibial osteotomies by a closing wedge. The osteosynthesis was always made with staples, and weight-bearing was resumed the day after operation, protected by a whalebone splint, with 2 elbow crutches for 6 weeks. This technique allowed early mobilisation of the joint and rehabilitation. The incidence of pseudarthrosis did not exceed 1%. In order to obtain more precise correction and avoid the removal of an iliac graft, while retaining the same advantages (simplified osteosynthesis, early weight-bearing), we used a block of biocoral.
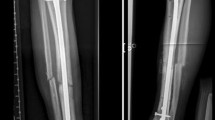
47 tibial osteotomies were done: 39 to produce valgus, 6 for varisation and two opening osteotomies for recurvatum. The common valgus osteotomy was done by a medial parapatellar route of approach; the inner aspect of the tibia was rasped to give an osteotomy line oblique upward and outward, virtually at the level of the superior tibiofibular joint. This line was made to gape by creating a “greenstick” fracture of the external cortex using Meary forceps, so as to embed the coral graft. A coral graft was embedded whose dimensions vary from 5° t0 15°. Osteosynthesis was with two staples. The disadvantage was that sometimes there was a loss of correction during the initial weight-bearing, especially when the internal cortex had been breached.
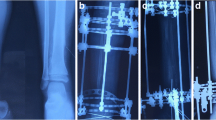
Consolidation of the osteotomy site, tolerance of the coral block, osteo-integration of the latter and the global result of the procedure were assessed at maximum follow-up. Of the 47 osteotomies, 18 required surgical revision between the 4th month and 2nd year after operation to remove the coral block, usually when union of the osteotomy was complete. Only 4 patients required reoperation for pseudarthrosis. In the others, pain or degree of swelling, have justified reoperation, to eliminate a necrotic abscess in the midst of the united bony focus. All the patients save one had an aseptic course with rapid disappearance of pain after removal of the necrotic tissue.
The less angled coral blocks were incorporated more easily, whereas the blocks of 15° are not revascularised and have been abandoned.
Résumé
Depuis 1980, nous avons l'habitude d'effectuer les ostéotomies tibiales de valgisation par une ostéotomie de fermeture. L'ostéosynthèse a toujours été réalisée par des agrafes et, surtout, la mise en charge s'effectue le lendemain de l'op#x00E9;ration sous couvert d'une attelle baleinée. Cette technique nous permet de mobiliser précocement l'articulation et d'entreprendre la rééducation proprement dite dès la sixième semaine dans d'excellentes conditions puisque les patients marchent avec appui pendant six semaines. Le taux de pseudarthrose ne dépasse pas 1% dans notre expérience.
Dans le but d'obtenir une correction plus précise, d'éviter le prélèvement d'un greffon iliaque, tout en conservant les mêmes avantages (ostéosynthèse simplifiée, mise en charge précoce), nous avons, à Mulhouse et à Reims, utilisé un bloc de biocorail.
47 ostéotomies tibiales ont été effectuées : par une voie d'abord para-patellaire interne, 0n rugine la face interne du tibia de façon à réaliser un trait d'ostéotomie oblique en haut et en-dehors pratiquement en regard de l'articulation péronéo-tibiale supérieure. On encastre un greffon de corail dont les dimensions vont de 5° jusqu'à 15°. L'ostéosynthèse est obtenue par deux agrafes. La mise en charge du patient est très précoce sous couvert d'une attelle en coutil baleiné.
La consolidation du foyer d'ostéotomie, la tolérance du bloc de corail, l'ostéo-intégration de celui-ci et le résultat global de l'intervention ont été jugés au recul maximum. Sur les 47 ostéotomies, 18 ont nécessité une reprise chirurgicale entre le 4e mois et la 2e année des suites opératoires pour élimination du bloc de corail. Cette élimination s'est produite alors que dans la grande majorité des cas la consolidation du foyer d'ostéotomie était acquise. Seuls 4 patients ont nécessité une reprise chirurgicale pour pseudarthrose. Pour les autres, apparition de douleurs, tuméfaction plus ou moins importante, ont justifié d'une réintervention : l'incision a permis d'éliminer un abcès crayeux et nécrotique au sein du foyer osseux consolidé. Tous les patients sauf un ont eu une évolution aseptique avec une disparition rapide des douleurs après élimination du tissu nécrotique.
Nous avons l'impression que les blocs de corail de 5° s'intègrent plus facilement alors que les blocs de 10° ou plus ne peuvent être colonisés par le bourgeon vasculaire, notion confirmée par l'anatomie pathologique.
Nous avons complètement abandonné l'utilisation de ces blocs de corail dont l'ostéo-intégration est insuffisante et qui, surtout, ont une fâcheuse tendance à s'éliminer.
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Petit, R., Segal, P. Use of a coral graft in superior metaphyseal osteotomies of the tibia. Eur J Orthop Surg Traumatol 7, 127–129 (1997). https://doi.org/10.1007/BF00578787
Issue Date:
DOI: https://doi.org/10.1007/BF00578787