
Abstract
Background
Laparoscopic sleeve gastrectomy (LSG) is gaining popularity as a procedure for the treatment of morbid obesity. Its indications and long-term results are currently under evaluation. Initially started as a first-stage procedure for superobese patients, it is now emerging as a standalone procedure in Asia and other parts of the world. Early results suggest that, at the end of 1 year, weight loss and resolution of comorbidities with LSG is comparable to laparoscopic Roux-en-Y gastric bypass (LRYGB). Whether LSG alone can replace LRYGB as a standard bariatric procedure is questionable. The aim of this study is to compare the results, resolution of comorbidities, and complications between LSG and LRYGB.
Methods
A retrospective comparative analysis was done of 50 patients in each arm who underwent LSG and LRYGB from October 2007 to March 2008. Both groups were matched for age, sex, and body mass index. The resolution of comorbidities, percentage of excess weight loss (EWL), and complications were studied at 6 months and 1 year in our study.
Results
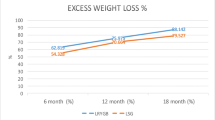
It was seen that resolution of most comorbidities such as type 2 diabetes, hypertension, dyslipidemia, sleep apnea, joint pains, and percentage of EWL in both groups was comparable at the end of 6 months and 1 year. Though early resolution of type 2 diabetes was seen to be better in the LRYGB group, the results matched up at 1 year. There was increased incidence of gastroesophageal reflux disease in LSG patients. On comparison, it was also observed that the Asian studies have shown better results with LSG when compared to studies done in a largely Caucasian population.
Conclusions
Long-term studies are needed to evaluate the efficacy of LSG alone as a procedure for the treatment of morbid obesity and its comorbidities.




Similar content being viewed by others


References
Chu CA, Gagner M, Quinn T, et al. Two stage laparoscopic biliopancreatic diversion with duodenal switch: an alternative approach to super-super morbid obesity. Surg Endosc. 2002;16:S069.
Baltasar A, Serra C, Perez N, et al. Laparoscopic sleeve gastrectomy: a multipurpose bariatric operation. Obes Surg. 2005;15:1124–8.
Mognol P, Chosidow D, Marmuse JP. Laparoscopic sleeve gastrectomy as an initial bariatric operation for high risk patients: initial results in 10 patients. Obes Surg. 2005;15:1030–3.
Han MS, Kim WW, Oh JH. Results of laparoscopic sleeve gastrectomy (LSG) at 1 year in morbidly obese Korean patients. Obes Surg. 2005;15:1469–75.
Langer FB, Reza Hoda MA, Bohdjalian A, et al. Sleeve gastrectomy and gastric banding: effects on plasma ghrelin levels. Obes Surg. 2005;15:1204–9.
Lee CM, Feng JJ, Cirangle PT, et al. Laparoscopic vertical sleeve gastrectomy for morbid obesity in 216 patients: report of two-year results. Surg Endosc. 2006;20(Suppl):255.
MacLean LD, Rhode B, Forse RA. Late results of vertical banded gastroplasty for morbid obesity. Surgery. 1990;107:20–7.
Martin MJ, Mullenix PS, Steel SR, et al. A case-match analysis of prior failed bariatric procedures converted to resectional gastric bypass. Am J Surg. 2004;187:666–70.
Ortega J, Sala F, Flor B, et al. Vertical banded gastroplasty converted to Roux-en-Y gastric bypass: little impact on nutritional status after 5-year follow-up. Obes Surg. 2004;14:638–43.
Jouhnston D, Dachtler J, Sue-Ling HM, et al. The Magentrasse and Mill operation for morbid obesity. Obes Surg. 2003;13:10–6.
Cottam D, Qureshi FG, Mattar SG, et al. Laparoscopic sleeve gastrectomy as an initial weight- loss procedure for high risk patients with morbid obesity. Surg Endosc. 2006;20(6):859–63.
Silecchia G, Boru C, Pecchia A, et al. Effectiveness of laparoscopic sleeve gastrectomy (first stage of laparoscopic biliopancreatic diversion with a duodenal switch) on comorbidities in superobese high-risk patients. Obes Surg. 2006;16(9):1138–44.
Broglio F, Arvat E, Benso A, et al. Ghrelin, a natural GH sectretagogue produced by the stomach, induces hyperglycaemia and reduces insulin secretion in humans. J Clin Endocrinol Metab. 2001;86:5083–6.
Ikezaki A, Hosoda H, Ito K, et al. Fasting plasma ghrelin levels are negatively correlated with insulin resistance and PAI-1, but not with leptin, in obese children and adolescents. Diabetes. 2002;51:3408–11.
Toshihiko Y, Katsuya D, Hideyuki S, et al. Ghrelin regulates insulin release and glycaemia: physiological ole and therapeutic potential. Curr Diabetes Rev. 2008;4:18–23.
Simmons D, Dr W, Powell MJ. The Coventry Diabetes Study: prevalence of diabetes and impaired glucose tolerance in Europids and Asians. Q J Med. 1991;81:1021–30.
Himpens J, Dapri G, Cadiere GB, et al. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg. 2006;16:1450–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lakdawala, M.A., Bhasker, A., Mulchandani, D. et al. Comparison Between the Results of Laparoscopic Sleeve Gastrectomy and Laparoscopic Roux-en-Y Gastric Bypass in the Indian Population: A Retrospective 1 Year Study. OBES SURG 20, 1–6 (2010). https://doi.org/10.1007/s11695-009-9981-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-009-9981-9